You might also like
- Endorsement SheetDocument1 pageEndorsement SheetLucelle MarieNo ratings yet
- Focus Charting Example PDFDocument1 pageFocus Charting Example PDFRegine Lorenzana Mey-AngNo ratings yet
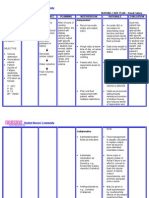
- OCAMPO, Maria Cecilia R. BSN 3d2 - 8i / MS Nursing Care Plan Related To Hypercalcemia Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesOCAMPO, Maria Cecilia R. BSN 3d2 - 8i / MS Nursing Care Plan Related To Hypercalcemia Assessment Diagnosis Planning Intervention Rationale Evaluationchurva_freak433533% (9)
- Ahmed Copd Case StudyDocument6 pagesAhmed Copd Case StudyAhmad BaolayyanNo ratings yet
- Nursing Care Plan for Breast CancerDocument2 pagesNursing Care Plan for Breast CancerMaina BarmanNo ratings yet
- Factors Affecting The Nurse Licensure ExaminationDocument3 pagesFactors Affecting The Nurse Licensure ExaminationPaul Ryan Tagaduar50% (2)
- SDH Nursing Health HistoryDocument2 pagesSDH Nursing Health HistorybojumsNo ratings yet
- You Are Caring For A Patient With An NG Feeding TubeDocument2 pagesYou Are Caring For A Patient With An NG Feeding TubeWen Silver100% (1)
- NCP 3Document3 pagesNCP 3Grae TaclobNo ratings yet
- Drug StudyDocument20 pagesDrug StudydjanindNo ratings yet
- Nursing Care Plan Template for Student Fideli L. AbaquitaDocument1 pageNursing Care Plan Template for Student Fideli L. AbaquitafabaquitaNo ratings yet
- Nursing Care Plan Renal FailureDocument2 pagesNursing Care Plan Renal FailureMark Jason Rabadan100% (1)
- Nursing Care Plan: CancerDocument6 pagesNursing Care Plan: Cancerneuronurse71% (7)
- Nursing Care Plan For Myocardial InfarctionDocument1 pageNursing Care Plan For Myocardial InfarctionIshaBrijeshSharmaNo ratings yet
- Aaa Gastrectomy NCP FinalDocument13 pagesAaa Gastrectomy NCP Finallexzaf100% (1)
- Narrative ReportDocument2 pagesNarrative ReportSam AlipioNo ratings yet
- Two Mechanisms of Hypertensive NephrosclerosisDocument2 pagesTwo Mechanisms of Hypertensive NephrosclerosisJessica Damasen Caballero0% (1)
- Inneffective Health Maintenence Care PlanDocument3 pagesInneffective Health Maintenence Care PlanTammy Litzenberger-HarrisNo ratings yet
- DP For Acute Respiratory FailureDocument1 pageDP For Acute Respiratory FailurePauline SalgadoNo ratings yet
- NCP For CTTDocument1 pageNCP For CTTJen Rhae LimNo ratings yet
- NCP Ineffective TissueDocument2 pagesNCP Ineffective TissueFhel AragonNo ratings yet
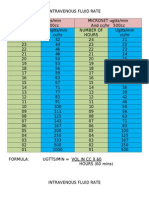
- Intravenous Fluid RateDocument2 pagesIntravenous Fluid RatePbNo ratings yet
- Care Plan ExampleDocument2 pagesCare Plan Exampleincess27100% (1)
- Multiple MyelomaDocument2 pagesMultiple MyelomaKolin JandocNo ratings yet
- Nursing care plan for post-CS patient with pre-eclampsiaDocument3 pagesNursing care plan for post-CS patient with pre-eclampsiaGiezel PeraltaNo ratings yet
- Why Join PNADocument2 pagesWhy Join PNADarren CariñoNo ratings yet
- Post-CS Pain Charting SampleDocument1 pagePost-CS Pain Charting SampleErika Grace Modelo100% (1)
- Breast Ca NCPDocument3 pagesBreast Ca NCPThirdy AquinoNo ratings yet
- 5NCPDocument4 pages5NCPSara ThorntonNo ratings yet
- Nursing Research-Title PageDocument1 pageNursing Research-Title PageKatherine 'Chingboo' Leonico LaudNo ratings yet
- Thyroidectomy procedure detailsDocument2 pagesThyroidectomy procedure detailsFeridan Roi Manzano100% (3)
- BSNURSE: NCP - HypertensionDocument3 pagesBSNURSE: NCP - Hypertensionmickey_beeNo ratings yet
- Nursing Care Plan for Patient with LymphedemaDocument1 pageNursing Care Plan for Patient with Lymphedemayasira50% (2)
- Nursing Student TPR Monitoring SheetDocument2 pagesNursing Student TPR Monitoring SheetAnnalou Amadure JoaquinNo ratings yet
- Giving of Medication 12 RightsDocument41 pagesGiving of Medication 12 RightsLeslie PaguioNo ratings yet
- NCP ModsDocument6 pagesNCP ModsNickos Andrew Magno Asanza Jr.No ratings yet
- NCP Patient 3 Cervical CADocument8 pagesNCP Patient 3 Cervical CAFatima LabaoNo ratings yet
- NCP 2 and Soapie 1Document5 pagesNCP 2 and Soapie 1narsD100% (1)
- Teaching Plan for Chronic Kidney Disease PatientDocument5 pagesTeaching Plan for Chronic Kidney Disease PatientYhan-yhan Rodriguez Khou100% (1)
- MG Problem Solving ProcessDocument2 pagesMG Problem Solving Processidadang0% (1)
- FdarDocument1 pageFdarEloisa Claire DayananNo ratings yet
- NCP KoDocument3 pagesNCP KoGerard Paul OrizaNo ratings yet
- NCP Micu Hascvd Cad - RioDocument5 pagesNCP Micu Hascvd Cad - RioRio BonifacioNo ratings yet
- NCP (Postpartum Hemmorhage)Document3 pagesNCP (Postpartum Hemmorhage)Anne DyNo ratings yet
- Case Management and InnovativeDocument2 pagesCase Management and InnovativeNur SanaaniNo ratings yet
- Hypertonic SolutionsDocument4 pagesHypertonic SolutionsVanessa PaguiriganNo ratings yet
- Gordon's Functional Health Pattern For Geriatric ClientsDocument8 pagesGordon's Functional Health Pattern For Geriatric ClientsGEN ERIGBUAGASNo ratings yet
- NCP For Laryngeal CancerDocument5 pagesNCP For Laryngeal CancerMădălina PinciucNo ratings yet
- DBFMH - Junior Staff Nurse Endorsement SheetDocument1 pageDBFMH - Junior Staff Nurse Endorsement SheetthrdNo ratings yet
- Ca2 Mood Disorder Q&ADocument7 pagesCa2 Mood Disorder Q&AgeejeiNo ratings yet
- Nursery ChartingDocument3 pagesNursery ChartingRI NANo ratings yet
- Cebu Doctors' University Hospital Summary of Nursing Care PlanDocument2 pagesCebu Doctors' University Hospital Summary of Nursing Care PlanSam PansoyNo ratings yet
- Endorsement SheetDocument1 pageEndorsement SheetMon DoceNo ratings yet
- Mini TicklerDocument1 pageMini TicklerTrisha Mae MacatangayNo ratings yet
- Asessment and Evaluation FormsDocument11 pagesAsessment and Evaluation FormsJU DYNo ratings yet
- Hiv Lab Initial ApplicationDocument5 pagesHiv Lab Initial ApplicationJohn SmithNo ratings yet
- NCP MaternalDocument21 pagesNCP MaternalDorothee GumisadNo ratings yet
- CH 1 TetDocument2 pagesCH 1 Tetapi-381832809No ratings yet
- Rle WorksheetDocument9 pagesRle WorksheetLiza AingelicaNo ratings yet
- OBSTETRIC ASSESSMENT TOOLDocument5 pagesOBSTETRIC ASSESSMENT TOOLDud AccNo ratings yet
- Pdhpe Notes FullDocument79 pagesPdhpe Notes FullFarhad HakimiNo ratings yet
- Images Dickson County, TN: 2012-13Document54 pagesImages Dickson County, TN: 2012-13Journal CommunicationsNo ratings yet
- ANDREI Research StudyDocument8 pagesANDREI Research StudyJennifer CabacunganNo ratings yet
- Myasthenia Gravis With Respiratory Failure in The Intensive Care UnitDocument4 pagesMyasthenia Gravis With Respiratory Failure in The Intensive Care UnitDr. FarhanNo ratings yet
- Best Books For FMGEDocument3 pagesBest Books For FMGEPrabesh Raj JamkatelNo ratings yet
- Revolutionizing Healthcare in Antipolo: A Cardiovascular and Respiratory HospitalDocument19 pagesRevolutionizing Healthcare in Antipolo: A Cardiovascular and Respiratory HospitalNellyn GutierrezNo ratings yet
- Malawi National Health Indicators FINAL v11 Clean WT Sign ComboDocument118 pagesMalawi National Health Indicators FINAL v11 Clean WT Sign ComboMarwa El SayedNo ratings yet
- Allied Doctor Bahrain DataDocument12 pagesAllied Doctor Bahrain DataShibu KavullathilNo ratings yet
- 1.Mcn FamilyDocument45 pages1.Mcn FamilymanilynNo ratings yet
- International Ayurvedic Medical Journal: Case Report ISSN: 2320 5091 Impact Factor: 4.018Document4 pagesInternational Ayurvedic Medical Journal: Case Report ISSN: 2320 5091 Impact Factor: 4.018triplete123No ratings yet
- A Simple Practice Guide For Dose Conversion Between Animals and HumanDocument6 pagesA Simple Practice Guide For Dose Conversion Between Animals and Humannisa yulianti suprahmanNo ratings yet
- Rebekah Antoine: WORK EXPERIENCEDocument6 pagesRebekah Antoine: WORK EXPERIENCEapi-416398178No ratings yet
- CHED MEMORANDUM ORDER (CMO) No. 14 Series of 2009Document129 pagesCHED MEMORANDUM ORDER (CMO) No. 14 Series of 2009lylesantos85% (48)
- PainDocument9 pagesPainSwati SharmaNo ratings yet
- Limited Access To Health CareDocument5 pagesLimited Access To Health CarezeeshanNo ratings yet
- Triaje SaltDocument2 pagesTriaje SaltoscuralizthNo ratings yet
- PHARMA Sep 08 1-15Document8 pagesPHARMA Sep 08 1-15medigistNo ratings yet
- Haad RequirementsDocument3 pagesHaad RequirementsMichael GerardNo ratings yet
- 06 PSUR PBRER Thomas MunzDocument35 pages06 PSUR PBRER Thomas MunzMohabKamalNo ratings yet
- License Application (LIC1558941)Document2 pagesLicense Application (LIC1558941)souq alkanzNo ratings yet
- 5th Edition Hospital STD April 2020 PDFDocument148 pages5th Edition Hospital STD April 2020 PDFFeroz Ikbal100% (1)
- Overview of pediatric nursing الباب الاولDocument2 pagesOverview of pediatric nursing الباب الاولmathio medhatNo ratings yet
- List of Life - MembersDocument100 pagesList of Life - Membersdrdineshsuman100% (1)
- MD II Material Pentru 14.04.2020Document3 pagesMD II Material Pentru 14.04.2020Irina Panciu StefanNo ratings yet
- 75 5056am0703 614 623Document10 pages75 5056am0703 614 623Rizkhy WahyuNo ratings yet
- ZZZZZZZDocument34 pagesZZZZZZZmikeNo ratings yet
- Ifcc CCLM Workshop Praveen Sharma Ethics in Clinical Laboratory PracticeDocument26 pagesIfcc CCLM Workshop Praveen Sharma Ethics in Clinical Laboratory PracticeAl- ImanuddinNo ratings yet
- Neuropsychopharmacology The Fifth Generation of Progress: 5th EditionDocument2,054 pagesNeuropsychopharmacology The Fifth Generation of Progress: 5th EditiondanilomarandolaNo ratings yet
- Mba20238 A Rosemont CaseDocument2 pagesMba20238 A Rosemont CaseJeevanandam PNo ratings yet
- Manage healthcare facility designs in RevitDocument1 pageManage healthcare facility designs in RevitSoporte LexemaNo ratings yet