You might also like
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationFrom EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationRating: 3 out of 5 stars3/5 (1)
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!From EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!No ratings yet
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- Essential Facts in Cardiovascular Medicine: Board Review and Clinical PearlsFrom EverandEssential Facts in Cardiovascular Medicine: Board Review and Clinical PearlsNo ratings yet
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasFrom EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasRating: 3 out of 5 stars3/5 (5)
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Basic EKG For DummiesDocument133 pagesBasic EKG For Dummieseduardocmoura86% (7)
- ECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasFrom EverandECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasRating: 5 out of 5 stars5/5 (2)
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Advance Cardiac Life Support: Short, Sweet and to the PointFrom EverandAdvance Cardiac Life Support: Short, Sweet and to the PointRating: 3 out of 5 stars3/5 (2)
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- ArrhythmiaDocument2 pagesArrhythmiaChris Pritchard93% (30)
- ECG Interpretation Guide - Key Components and AbnormalitiesDocument1 pageECG Interpretation Guide - Key Components and Abnormalitieshirsi20051879% (24)
- Dysrhythmias ChartDocument6 pagesDysrhythmias Chartjkrix100% (1)
- Basic Arrhythmia RulesDocument3 pagesBasic Arrhythmia Rulesgreenflames0997% (30)
- A Simplified ECG GuideDocument4 pagesA Simplified ECG Guidejalan_z96% (27)
- EKG Cheat SheetDocument9 pagesEKG Cheat SheetAlert Twitter100% (5)
- Cardiac Dysrhythmia Chart Med-Surg NUR4Document3 pagesCardiac Dysrhythmia Chart Med-Surg NUR4ktfosterfd2096% (97)
- EKG Flash CardsDocument5 pagesEKG Flash CardsRyann Sampino FreitasNo ratings yet
- EKG ExamplesDocument9 pagesEKG ExamplesMayer Rosenberg99% (235)
- Bonehead Electrocardiography: The Easiest and Best Way to Learn How to Read Electrocardiograms—No Bones About It!From EverandBonehead Electrocardiography: The Easiest and Best Way to Learn How to Read Electrocardiograms—No Bones About It!Rating: 5 out of 5 stars5/5 (2)
- Cardiac DysrhythmiasDocument3 pagesCardiac DysrhythmiasKatherine Santiago92% (62)
- ECG Rhythm Interpretation GuideDocument3 pagesECG Rhythm Interpretation Guideis_aradanas0% (1)
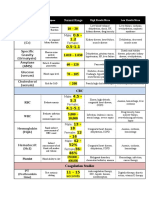
- Lab ValuesDocument3 pagesLab Valuessurviving nursing school100% (1)
- ECG ReadingDocument11 pagesECG ReadingSuresh Shrestha100% (1)
- Pakya ECG BasicsDocument5 pagesPakya ECG BasicsFrederick CokroNo ratings yet
- EKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXFrom EverandEKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXRating: 5 out of 5 stars5/5 (2)
- Basic EKG ECG Rhythms CheatsheetDocument1 pageBasic EKG ECG Rhythms CheatsheetAhmad83% (6)
- EKG Interpretation GuideDocument2 pagesEKG Interpretation GuideFabian Ramirez HincapiéNo ratings yet
- ACLS EKG Rhythms and InterpretationDocument10 pagesACLS EKG Rhythms and Interpretationdonheyzz_02No ratings yet
- The Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesFrom EverandThe Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesNo ratings yet
- Ekg Guidelines PDFDocument7 pagesEkg Guidelines PDFd.ramadhan100% (1)
- Reading A EKGDocument10 pagesReading A EKGMayer Rosenberg100% (15)
- ECG Interpretation - Axis and Conduction AbnormalitiesDocument9 pagesECG Interpretation - Axis and Conduction Abnormalitiesradha1000100% (1)
- ECG StripsDocument5 pagesECG StripsNursingSchoolNotes100% (1)
- ECGDocument6 pagesECGMatthew MackeyNo ratings yet
- ECGFactsMadeIncrediblyQuick 1steditionDocument127 pagesECGFactsMadeIncrediblyQuick 1steditionLisandra Damian100% (2)
- Acid-Base WorksheetDocument2 pagesAcid-Base WorksheetMayer Rosenberg100% (18)
- ECG InterpretationDocument5 pagesECG InterpretationRichelle Dianne Ramos-Giang100% (3)
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesRating: 4 out of 5 stars4/5 (6)
- Critical Care - Hemodynamic Monitoring TableDocument7 pagesCritical Care - Hemodynamic Monitoring TableVictoria Romero100% (2)
- Haemodynamic Monitoring & Manipulation: an easy learning guideFrom EverandHaemodynamic Monitoring & Manipulation: an easy learning guideNo ratings yet
- EKG Practice Test QuizDocument16 pagesEKG Practice Test QuizAbdul Rohim100% (1)
- Quick Ekg ReferenceDocument23 pagesQuick Ekg Referencekowaikowar100% (2)
- PATHOPHYSIOLOGY: Passbooks Study GuideFrom EverandPATHOPHYSIOLOGY: Passbooks Study GuideRating: 4.5 out of 5 stars4.5/5 (2)
- Ecg Reading NotesDocument17 pagesEcg Reading NotesMarian FloresNo ratings yet
- A&PDocument3 pagesA&PjessjayleeNo ratings yet
- High Yield Surgery Shelf ReviewDocument77 pagesHigh Yield Surgery Shelf ReviewDuke71% (7)
- The Liver LectureDocument13 pagesThe Liver LectureEmmi Maliza HutagaolNo ratings yet
- ANEMIA - PathologyDocument89 pagesANEMIA - Pathologyjessjaylee100% (1)
- Glycogen Metabolism and RegulationDocument34 pagesGlycogen Metabolism and RegulationjessjayleeNo ratings yet
- Bob Page 12lead WorkbookDocument44 pagesBob Page 12lead Workbookjessjaylee100% (3)
- Usmle LabsDocument3 pagesUsmle LabsAdnan KhurshidNo ratings yet
- Developmental PsychologyDocument56 pagesDevelopmental Psychologyjessjaylee100% (1)
- Fatty Acid OxidationDocument43 pagesFatty Acid OxidationjessjayleeNo ratings yet
- Naming Compounds and Balancing EquationsDocument18 pagesNaming Compounds and Balancing EquationsjessjayleeNo ratings yet
- Lab5 GeneExpressionDocument26 pagesLab5 GeneExpressionjessjayleeNo ratings yet
- Using ABAQUS to Reduce Tire Belt Edge StressesDocument10 pagesUsing ABAQUS to Reduce Tire Belt Edge StressesGautam SharmaNo ratings yet
- The Great GatsbyDocument23 pagesThe Great Gatsbychia simNo ratings yet
- Assessment 2 Stat20053 Descriptive Statistics - CompressDocument2 pagesAssessment 2 Stat20053 Descriptive Statistics - CompressDon RatbuNo ratings yet
- Bretzing y Kulhavy (1981) Note-Taking Passage Style PDFDocument9 pagesBretzing y Kulhavy (1981) Note-Taking Passage Style PDFSergio Andrés Quintero MedinaNo ratings yet
- United States Court of Appeals, Fourth CircuitDocument4 pagesUnited States Court of Appeals, Fourth CircuitScribd Government DocsNo ratings yet
- Puddu v. 6D Global Tech. - Securities Complaint PDFDocument57 pagesPuddu v. 6D Global Tech. - Securities Complaint PDFMark JaffeNo ratings yet
- Automatic Analysis of Annual Financial Reports: A Case StudyDocument11 pagesAutomatic Analysis of Annual Financial Reports: A Case StudyYuliana MargarettaNo ratings yet
- Classroom Management and DisciplineDocument2 pagesClassroom Management and DisciplineMonaida Umpar IbrahimNo ratings yet
- Guía BaccettiDocument11 pagesGuía BaccettiPercy Andree Bayona GuillermoNo ratings yet
- WHLP in Rws Week 5 and 6 q3Document6 pagesWHLP in Rws Week 5 and 6 q3Rebhie DiezaNo ratings yet
- Ich Validation 2qaDocument9 pagesIch Validation 2qaBishal AdhikariNo ratings yet
- Cinderella Play ScriptDocument6 pagesCinderella Play ScriptKhayla Khairunnisa81% (21)
- TM55 1520 242 MTFDocument192 pagesTM55 1520 242 MTFJakub Kostka100% (1)
- Simple PresentDocument2 pagesSimple PresentJulio MedinaNo ratings yet
- Bagi Latihan Soal 3Document3 pagesBagi Latihan Soal 3MUH LULU BNo ratings yet
- Calculus Problems Solutions BlogDocument5 pagesCalculus Problems Solutions BlogheeraNo ratings yet
- Hospital Ship Feasibility StudyDocument10 pagesHospital Ship Feasibility StudyRhona JhoyNo ratings yet
- Module 6 - Arabic LiteratureDocument26 pagesModule 6 - Arabic LiteratureFrancis TatelNo ratings yet
- The Lair of Arachas - A Mausritter AdventureDocument8 pagesThe Lair of Arachas - A Mausritter AdventureGladstone PinheiroNo ratings yet
- Pride and Prejudice Plot StructureDocument3 pagesPride and Prejudice Plot StructureGeetanjali Joshi100% (2)
- The Cell Cycle: How Cells Grow and DivideDocument21 pagesThe Cell Cycle: How Cells Grow and DivideAqsa YaminNo ratings yet
- Final Addendum to Report on Clergy AbuseDocument2 pagesFinal Addendum to Report on Clergy AbuseJustin BobbyNo ratings yet
- The Effect of Work Discipline and Leadership On Organizational Commitments With Work Satisfaction As Intervening Variables (Case Study at Asam Jujuhan Sub-District Office Dharmasraya Regency)Document11 pagesThe Effect of Work Discipline and Leadership On Organizational Commitments With Work Satisfaction As Intervening Variables (Case Study at Asam Jujuhan Sub-District Office Dharmasraya Regency)International Journal of Innovative Science and Research TechnologyNo ratings yet
- AOE 5104 Class Notes and ScheduleDocument26 pagesAOE 5104 Class Notes and ScheduleverbicarNo ratings yet
- Mini CompactionDocument8 pagesMini CompactionFei Zhen CatteryNo ratings yet
- dll-4th QTR.-MUSIC-MAY-3-4-2023Document5 pagesdll-4th QTR.-MUSIC-MAY-3-4-2023Dennis MartinezNo ratings yet
- Learning Activity Sheet in 3is (Inquiries, Investigation, Immersion)Document5 pagesLearning Activity Sheet in 3is (Inquiries, Investigation, Immersion)Roselyn Relacion LucidoNo ratings yet
- Test Tenses en AnswersDocument4 pagesTest Tenses en AnswersAmit Kumar LalNo ratings yet
- Moon Landing ConspiracyDocument17 pagesMoon Landing ConspiracyElianeSalamNo ratings yet
- Sacha Doucet-Kim Cancer AssignmentDocument3 pagesSacha Doucet-Kim Cancer AssignmentSacha Doucet-KimNo ratings yet