You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Vitamins and Minerals 09 V 2Document42 pagesVitamins and Minerals 09 V 2giannidietNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Vegetarian Diet-Panacea For Modern Lifestyle DiseasesDocument14 pagesVegetarian Diet-Panacea For Modern Lifestyle DiseasesgiannidietNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Session5E-SixWaystoBuildStamina - ManageFatigueDocument4 pagesSession5E-SixWaystoBuildStamina - ManageFatiguegiannidiet100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Carbohydrate Ingestion Can Completely Suppress Endogenous Glucose Production During ExerciseDocument13 pagesCarbohydrate Ingestion Can Completely Suppress Endogenous Glucose Production During ExercisegiannidietNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Eating in The ZoneDocument7 pagesEating in The ZonejafrinkNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- GSSI Carbs Hormones EndDocument5 pagesGSSI Carbs Hormones EndgiannidietNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Training RecoveryDocument23 pagesTraining Recoveryapi-3835136100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Studi Scient RugbyDocument6 pagesStudi Scient RugbygiannidietNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- EFSA - 2010 - Stevia GRASSDocument84 pagesEFSA - 2010 - Stevia GRASSLiliana CelayaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Energy Density of Foods, But Not Beverages, Is Positively Associated With Body Mass Index in Adult WomenDocument8 pagesEnergy Density of Foods, But Not Beverages, Is Positively Associated With Body Mass Index in Adult WomengiannidietNo ratings yet
- Soccer Sports Nutrition Presentation U11 U14Document11 pagesSoccer Sports Nutrition Presentation U11 U14giannidietNo ratings yet
- Brain FuelDocument2 pagesBrain FuelgiannidietNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- International Journal Sports NutritionDocument13 pagesInternational Journal Sports NutritiongiannidietNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- 12weeks WomenDocument49 pages12weeks Womenusmanmughal111100% (5)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Medium Chain TriglyceridesDocument3 pagesMedium Chain TriglyceridesgiannidietNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Cism08 Sports DieteticsDocument12 pagesCism08 Sports DieteticsgiannidietNo ratings yet
- GSSI-High Carbohydrate Meals and PerformanceDocument8 pagesGSSI-High Carbohydrate Meals and PerformancegiannidietNo ratings yet
- Scientific Abstracts About Dairy and HealthDocument5 pagesScientific Abstracts About Dairy and HealthgiannidietNo ratings yet
- Salt Intake, Stroke, and Cardiovascular Disease Meta-Analysis of Prospective StudiesDocument9 pagesSalt Intake, Stroke, and Cardiovascular Disease Meta-Analysis of Prospective StudiesPatrícia BentoNo ratings yet
- Sports Nutrition For Young Adults: HydrationDocument4 pagesSports Nutrition For Young Adults: HydrationgiannidietNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Cut DietDocument76 pagesThe Cut DietMarc David83% (6)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Early Postexercise Muscle Glycogen Recovery IsDocument9 pagesEarly Postexercise Muscle Glycogen Recovery IsgiannidietNo ratings yet
- Multivitamin Use and Telomere Length in WomenDocument7 pagesMultivitamin Use and Telomere Length in WomengiannidietNo ratings yet
- Game DayDocument20 pagesGame Daygiannidiet100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Martial Arts News and Report: Women's DefenseDocument4 pagesMartial Arts News and Report: Women's DefensegiannidietNo ratings yet
- Dados-Artigos-Nutricao-Nutricao Esportiva e Suplementacao-Supplementation of L-Carnitine in AthletesDocument7 pagesDados-Artigos-Nutricao-Nutricao Esportiva e Suplementacao-Supplementation of L-Carnitine in AthletesSri Nowo MinartiNo ratings yet
- Talbott CV 2008Document4 pagesTalbott CV 2008giannidietNo ratings yet
- Whole-Body Skeletal Muscle MassDocument7 pagesWhole-Body Skeletal Muscle MassgiannidietNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The 7th Workshop On The Assessment of Adequate Intake of Dietary Amino Acids-Summary of General DiscussionDocument3 pagesThe 7th Workshop On The Assessment of Adequate Intake of Dietary Amino Acids-Summary of General DiscussiongiannidietNo ratings yet
- Omics of Nutrition A New ParadigmDocument7 pagesOmics of Nutrition A New ParadigmgiannidietNo ratings yet
- Moluccas Health Journal: Jurnal Kesehatan UKIMDocument8 pagesMoluccas Health Journal: Jurnal Kesehatan UKIMIPS RSUNo ratings yet
- Mycosphere 5 Dulayetal.2015Document9 pagesMycosphere 5 Dulayetal.2015egemNo ratings yet
- Food DiaryDocument14 pagesFood Diaryandreea.mitroescuNo ratings yet
- Nutrition Final Print-Ready April 2011Document207 pagesNutrition Final Print-Ready April 2011jrence100% (1)
- SOS Approach To FeedingDocument6 pagesSOS Approach To FeedingBarbara OoNo ratings yet
- Healthy Eating - EbookDocument47 pagesHealthy Eating - EbookFernandoNo ratings yet
- EU Food Label GuidanceDocument99 pagesEU Food Label GuidanceMunteanu CristianNo ratings yet
- Detailed Lesson Plan in TVL - SCCDocument6 pagesDetailed Lesson Plan in TVL - SCCSuzette CorpuzNo ratings yet
- Metabolic Syndrome: Denz Marc Ray T. Alea First Year ResidentDocument38 pagesMetabolic Syndrome: Denz Marc Ray T. Alea First Year ResidentDenz Marc Ray Alea100% (2)
- CBLM - Food Processing NC2Document54 pagesCBLM - Food Processing NC2mike gilbert boadoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Kristina Saha Mintel and SimmonsDocument16 pagesKristina Saha Mintel and SimmonsKristina SahaNo ratings yet
- Connect Plus, U 3&5Document7 pagesConnect Plus, U 3&5Sameh IbrahimNo ratings yet
- C-NATTOLIN CatalogueDocument6 pagesC-NATTOLIN CatalogueFroggiesNo ratings yet
- CHAPTER 2 Nutrition Form 5 ScienceDocument10 pagesCHAPTER 2 Nutrition Form 5 SciencesakinahsulaimanNo ratings yet
- Effect of Multigrain Soya Panjiri Supplementation On Quetelet Index and Anaemia Profile of Malnourished Women of ChhattisgarhDocument4 pagesEffect of Multigrain Soya Panjiri Supplementation On Quetelet Index and Anaemia Profile of Malnourished Women of ChhattisgarhIJRASETPublicationsNo ratings yet
- Feeding Management of Poultry: Dr. Pankaj Kumar SinghDocument52 pagesFeeding Management of Poultry: Dr. Pankaj Kumar Singhshahbaz zafarNo ratings yet
- Chloe Ting - 2 Weeks Shred Challenge - Free Workout ProgramDocument8 pagesChloe Ting - 2 Weeks Shred Challenge - Free Workout ProgramNanciya LoomphaNo ratings yet
- LESSON 3 Types of MenuDocument37 pagesLESSON 3 Types of MenulobelynNo ratings yet
- News Lessons Joy of Eating Worksheet Elementary 503617Document4 pagesNews Lessons Joy of Eating Worksheet Elementary 503617Алёна ШариповаNo ratings yet
- Tribhuvan University Course Details for BHM 3rd SemesterDocument12 pagesTribhuvan University Course Details for BHM 3rd SemesterBijan GurungNo ratings yet
- Food and Nutrition Jean DrezeDocument7 pagesFood and Nutrition Jean DrezeSamridh NangiaNo ratings yet
- Complete Catalogue: Singing DragonDocument40 pagesComplete Catalogue: Singing DragonFrancesco Papa100% (2)
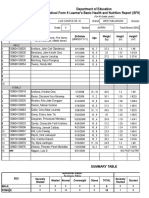
- School Form 8 SF8 (G5)Document4 pagesSchool Form 8 SF8 (G5)Melieza Melody AmpanNo ratings yet
- HEP Mommy and Me Mothers ClassDocument4 pagesHEP Mommy and Me Mothers ClassRoy CabuenasNo ratings yet
- DR Carl Reich MD FRCP - Calcium Vitamin D PaperDocument6 pagesDR Carl Reich MD FRCP - Calcium Vitamin D PaperAnonymous gwFqQcnaX100% (1)
- For PutoDocument15 pagesFor PutoRAYMON ROLIN HILADONo ratings yet
- Marketing Plan Project: - Ankita Bose Roll No:5Document9 pagesMarketing Plan Project: - Ankita Bose Roll No:5Vidhi BajajNo ratings yet
- 1 IntroductionDocument11 pages1 Introductionjvr341138No ratings yet
- Censored Health Secrets - DrWrightDocument24 pagesCensored Health Secrets - DrWrightKujua GigiNo ratings yet
- Factual EssayDocument8 pagesFactual EssayPang Fui ShihNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 5 out of 5 stars5/5 (1)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Proteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItFrom EverandProteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItRating: 4.5 out of 5 stars4.5/5 (19)
- The Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthFrom EverandThe Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthRating: 5 out of 5 stars5/5 (37)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodFrom EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodRating: 4.5 out of 5 stars4.5/5 (18)