You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- SCR - 9 - Pulp and Periradicular PathosisDocument12 pagesSCR - 9 - Pulp and Periradicular PathosisCWT2010No ratings yet
- Scr.7 - Intracanal Medicaments and TemporizationDocument13 pagesScr.7 - Intracanal Medicaments and TemporizationCWT2010No ratings yet
- SCR - 9 - Pulp and Periradicular PathosisDocument14 pagesSCR - 9 - Pulp and Periradicular PathosisCWT2010No ratings yet
- Slide - 11 - Procedural AccidentsDocument31 pagesSlide - 11 - Procedural AccidentsCWT2010100% (1)
- Special Impression ProceduresDocument27 pagesSpecial Impression ProceduresCWT2010No ratings yet
- Slides 9 - Pulp and Periradicular PathosisDocument39 pagesSlides 9 - Pulp and Periradicular PathosisCWT2010100% (1)
- Metal FrameWork Try inDocument20 pagesMetal FrameWork Try inCWT2010No ratings yet
- Opiods in AnesthesiaDocument16 pagesOpiods in AnesthesiaCWT2010100% (1)
- Slides 8 - Dental Pup BiologyDocument45 pagesSlides 8 - Dental Pup BiologyCWT2010No ratings yet
- Slide - 11 - Procedural AccidentsDocument31 pagesSlide - 11 - Procedural AccidentsCWT2010100% (1)
- Added Notes On Lab 1Document71 pagesAdded Notes On Lab 1CWT2010100% (1)
- Lab 1 CH 8Document59 pagesLab 1 CH 8CWT2010No ratings yet
- Slides - 7 - Intracanal Medicaments & TemporizationDocument53 pagesSlides - 7 - Intracanal Medicaments & Temporizationبراءة أحمد السلاماتNo ratings yet
- Hand Out (Internal Anatomy)Document11 pagesHand Out (Internal Anatomy)CWT2010No ratings yet
- Slides 3 - Internal AnatomyDocument45 pagesSlides 3 - Internal AnatomyCWT2010100% (1)
- Slides 2 - Wounds, UlcersDocument80 pagesSlides 2 - Wounds, UlcersCWT2010No ratings yet
- Slides 2 - Access CavityDocument7 pagesSlides 2 - Access CavityCWT2010No ratings yet
- Slide 4 - Working LengthDocument28 pagesSlide 4 - Working LengthCWT2010No ratings yet
- Slide 4 - ProbabilityDocument31 pagesSlide 4 - ProbabilityCWT2010No ratings yet
- Bleeding Tendency For DentistDocument58 pagesBleeding Tendency For Dentistshanfiza_92No ratings yet
- Anemia LectureDocument56 pagesAnemia Lectureshanfiza_92No ratings yet
- Scr.2 Access CavityDocument8 pagesScr.2 Access CavityCWT2010No ratings yet
- Slide 2 - 2 - Access Cavity PreparationDocument12 pagesSlide 2 - 2 - Access Cavity PreparationCWT2010No ratings yet
- Scr. 1 - History & ExaminationDocument21 pagesScr. 1 - History & ExaminationCWT2010No ratings yet
- Scr.1 - CT Hyperplasia 1Document10 pagesScr.1 - CT Hyperplasia 1CWT2010No ratings yet
- Lab 1 - Prostho IIDocument11 pagesLab 1 - Prostho IICWT2010No ratings yet
- Slide 3 - Data - PresentationDocument28 pagesSlide 3 - Data - PresentationCWT2010No ratings yet
- Krol, Removable Partial Denture Design-Outline SyllabusDocument231 pagesKrol, Removable Partial Denture Design-Outline SyllabusPrince Ahmed77% (22)
- Prostho II Dent 344 2012 SyllabusDocument15 pagesProstho II Dent 344 2012 SyllabusCWT2010No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Mtwo NiTi Rotary SystemDocument10 pagesMtwo NiTi Rotary SystemVioleta BotnariNo ratings yet
- Multiple Choice RatioDocument14 pagesMultiple Choice RatioDivine Joe Grace Marcelino100% (2)
- PALS Provider Manual Suggested Reading List: © 2016 American Heart AssociationDocument17 pagesPALS Provider Manual Suggested Reading List: © 2016 American Heart AssociationVitor Hugo G CorreiaNo ratings yet
- MediShield Life: Better Protection for AllDocument20 pagesMediShield Life: Better Protection for Alljakovach7No ratings yet
- Er LFD 11Document1 pageEr LFD 11EldwinCauilanNo ratings yet
- Clinical AssignmentDocument9 pagesClinical AssignmentkomalNo ratings yet
- Antifungal LectureDocument62 pagesAntifungal LectureVandana TayalNo ratings yet
- Haematology Laboratory User Handbook - Updated July 2020 JWDocument25 pagesHaematology Laboratory User Handbook - Updated July 2020 JWBassam AlharaziNo ratings yet
- Open Bone Grafting: Papineau TechniqueDocument7 pagesOpen Bone Grafting: Papineau TechniqueAlireza MirzasadeghiNo ratings yet
- AtelectasisDocument9 pagesAtelectasisArni ZulsitaNo ratings yet
- Poster PresentationDocument1 pagePoster PresentationAayat KhanNo ratings yet
- MS Nursing ReviewerDocument16 pagesMS Nursing ReviewerSunshine SiopaoNo ratings yet
- Effects of Maitland Mobilization and Mul PDFDocument6 pagesEffects of Maitland Mobilization and Mul PDFKuroha Hagane KunNo ratings yet
- The Management of Ovarian Hyperstimulation SyndromeDocument22 pagesThe Management of Ovarian Hyperstimulation SyndromeSitha MahendrataNo ratings yet
- ORTHOPAEDICS TRAUMADocument33 pagesORTHOPAEDICS TRAUMARhomizal MazaliNo ratings yet
- The Cognitive Assessment Toolkit Copy - v1 PDFDocument26 pagesThe Cognitive Assessment Toolkit Copy - v1 PDFTzoutzoukinaNo ratings yet
- Dialysis Nurse Responsibilities and DutiesDocument22 pagesDialysis Nurse Responsibilities and DutiesWyn Agustin0% (1)
- Ldust Resume 04-2014Document2 pagesLdust Resume 04-2014api-234544335No ratings yet
- Peads - Diamond Blackfan AnemiaDocument40 pagesPeads - Diamond Blackfan AnemiaBaran PalanimuthuNo ratings yet
- ATLS ProtocoloDocument21 pagesATLS Protocoloedgarjavier65100% (2)
- Eeg BookDocument102 pagesEeg BookmacrufoNo ratings yet
- Jurnal Pendukung 2Document13 pagesJurnal Pendukung 2Eko PrasNo ratings yet
- CPR GuidelinesDocument30 pagesCPR GuidelineswvhvetNo ratings yet
- Community Health Nursing Bag TechniqueDocument10 pagesCommunity Health Nursing Bag TechniqueKBDNo ratings yet
- Infectious Diseases Consultation ReportDocument5 pagesInfectious Diseases Consultation ReportRohitKumar100% (1)
- Swiss Medical ObjectivesDocument142 pagesSwiss Medical ObjectivesAndrés AlanísNo ratings yet
- Variable TypesDocument2 pagesVariable Typesmarmar418No ratings yet
- Case Report Consent Form TemplateDocument2 pagesCase Report Consent Form TemplateDaniel Antonio Valderrama Merejildo100% (1)
- Fitz Cardiology Paces NotesDocument26 pagesFitz Cardiology Paces NotesMuhammad BilalNo ratings yet
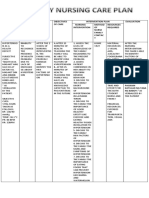
- Nelson FNCPDocument2 pagesNelson FNCPDenisse Shazz Mae MaretNo ratings yet