You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Kebijakan High AlertDocument8 pagesKebijakan High AlertheavyrainNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
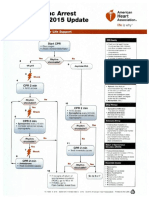
- ACLS 2015 Algorithm PDFDocument8 pagesACLS 2015 Algorithm PDFheavyrain100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Dermatophyta Non KandidiasisDocument32 pagesDermatophyta Non KandidiasisheavyrainNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Benign Positional Vertigo: Taleb Mohammed Mansoor Khaleil Ebrahem Al-MatroushiDocument27 pagesBenign Positional Vertigo: Taleb Mohammed Mansoor Khaleil Ebrahem Al-MatroushiSheila CantikNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Alcoholic CardiomyopathyDocument9 pagesAlcoholic CardiomyopathyheavyrainNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Acute Coronary SyndromeDocument19 pagesAcute Coronary SyndromeheavyrainNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Eye EmergenciesDocument18 pagesEye EmergenciesdrDre91No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- BPPVDocument27 pagesBPPVheavyrainNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Panic Away EbookDocument61 pagesPanic Away Ebooknobi_69100% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Nebulizer TherapyDocument2 pagesNebulizer Therapymarie100% (6)
- f3 Chapter 1Document110 pagesf3 Chapter 1miracleambitiousNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Breathing RetrainingDocument10 pagesBreathing RetrainingMarivic DianoNo ratings yet
- Tactical BreathingDocument3 pagesTactical Breathingsergio661204No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Labbio - Tue - Lab Report 3 - Group 5 TuesdayDocument5 pagesLabbio - Tue - Lab Report 3 - Group 5 TuesdayVân Anh Nguyễn NgọcNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- ECG (Cardiology Clinic 2006)Document127 pagesECG (Cardiology Clinic 2006)VuqarNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Thelemic Middle Pillar ExerciseDocument3 pagesThelemic Middle Pillar Exercisearalim4311100% (3)
- Fluid and Electrolytes BalanceDocument6 pagesFluid and Electrolytes BalanceMichelle Dona MirallesNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Craniofacial Biology Notes Unit 1Document37 pagesCraniofacial Biology Notes Unit 1nohacksNo ratings yet
- Asphyxia: DR Kaleem KhanDocument81 pagesAsphyxia: DR Kaleem KhanShafira WidiaNo ratings yet
- Zincum ValerianicumDocument3 pagesZincum ValerianicumKamalNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Uog15821 Online PDFDocument17 pagesUog15821 Online PDFernestosandNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- JasmonatesDocument38 pagesJasmonatesSpinu LiliaNo ratings yet
- Hands On-Equine Craniosacral NHMDocument4 pagesHands On-Equine Craniosacral NHMapi-237342656100% (1)
- SPM 4551 2006 Biology k2 BerjawapanDocument15 pagesSPM 4551 2006 Biology k2 Berjawapanpss smk selandarNo ratings yet
- PathologyDocument36 pagesPathologySayeed KhanNo ratings yet
- Neocortex Size As A Constraint On Group Size in Primates (Dunbar)Document25 pagesNeocortex Size As A Constraint On Group Size in Primates (Dunbar)David HeNo ratings yet
- Per Dev Lesson For 1 WeekDocument2 pagesPer Dev Lesson For 1 WeekEjay Balils IINo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Bio Chapter 5Document10 pagesBio Chapter 5Rosfaizzati MarnunNo ratings yet
- Peng Kaji AnDocument54 pagesPeng Kaji Anmabuhay crewNo ratings yet
- The Toxic Mind: The Biology of Mental Illness and ViolenceDocument27 pagesThe Toxic Mind: The Biology of Mental Illness and Violencemkljhrguyt100% (1)
- Capillary Blood CollectionDocument8 pagesCapillary Blood CollectionARIF AHAMMED P100% (1)
- Loco For Cocoa 1 Running Head: LOCO FOR COCOADocument13 pagesLoco For Cocoa 1 Running Head: LOCO FOR COCOAapi-310439970No ratings yet
- Observations During Fundus ExaminationDocument3 pagesObservations During Fundus ExaminationAn'umillah Arini ZidnaNo ratings yet
- Slid CH13Document93 pagesSlid CH13Senior TitopecNo ratings yet
- E01723 Yogic Asanas For Health and Vigour TextDocument138 pagesE01723 Yogic Asanas For Health and Vigour TextAnonymous nKVk2VC2VENo ratings yet
- Renal Emergency RevisiDocument103 pagesRenal Emergency Revisidesy f sarahNo ratings yet
- Trophical Fishes PDFDocument558 pagesTrophical Fishes PDFzlatko5No ratings yet
- Metabolic Basis of Human DiseaseDocument25 pagesMetabolic Basis of Human DiseaseDr Science YNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)