You might also like
- Potential Theory of Steady Ship MotionDocument49 pagesPotential Theory of Steady Ship MotionhossamNo ratings yet
- Dtic Ada058534 PDFDocument382 pagesDtic Ada058534 PDFAndyNo ratings yet
- FUSELAGE-MOUNTED ANTENNA CODE USER'S MANUALDocument76 pagesFUSELAGE-MOUNTED ANTENNA CODE USER'S MANUALssvivekanandhNo ratings yet
- Semiconductor Pyq LectureDocument25 pagesSemiconductor Pyq LectureAyush KumarNo ratings yet
- New York State PCRDocument3 pagesNew York State PCRdandude505No ratings yet
- Trombone Symphony "The Lord of the RingsDocument1 pageTrombone Symphony "The Lord of the RingsAlbert BellmuntNo ratings yet
- TR-18!05!110 7th Joint Inspection and Sign-Off Punchlist For Masonry Opening Handover at 9th Floor Prior To Window Panel InstallationDocument4 pagesTR-18!05!110 7th Joint Inspection and Sign-Off Punchlist For Masonry Opening Handover at 9th Floor Prior To Window Panel InstallationRodelNo ratings yet
- CDPL-EEL-SNM-PUMP-MEC-0002 - Booster Pump Performance Curves - 4PC-47938 - R1Document4 pagesCDPL-EEL-SNM-PUMP-MEC-0002 - Booster Pump Performance Curves - 4PC-47938 - R1Amit KumarNo ratings yet
- Student Involved Shootings, by Tom GivensDocument6 pagesStudent Involved Shootings, by Tom GivensxurxinhooNo ratings yet
- Gretchaninov, Alexander - Clarinet MiniaturesDocument34 pagesGretchaninov, Alexander - Clarinet MiniaturesMário Batalha100% (4)
- Bassclarinet PièceDocument2 pagesBassclarinet PièceBelén Ojeda RojasNo ratings yet
- Evening Song FlutesDocument2 pagesEvening Song FlutesTaylor ReheNo ratings yet
- 7. 62mm COLD-WORKED STEEL CARTRIDGE CASEDocument93 pages7. 62mm COLD-WORKED STEEL CARTRIDGE CASEAddison TuNo ratings yet
- Status Quo Rockin All Over The World 1976 PDFDocument4 pagesStatus Quo Rockin All Over The World 1976 PDFAnya McRaeNo ratings yet
- rICF SystemsDocument21 pagesrICF SystemsMidz SalipNo ratings yet
- Robert Muczynski Duos For Flute and ClarinetDocument12 pagesRobert Muczynski Duos For Flute and ClarinetteodoraNo ratings yet
- Mechanical Practical FileDocument49 pagesMechanical Practical FileFaijan MohammadNo ratings yet
- Our Town July 13, 1944Document4 pagesOur Town July 13, 1944narberthcivicNo ratings yet
- Adobe Scan 06 Sep 2023Document3 pagesAdobe Scan 06 Sep 2023nokubongamagagula99No ratings yet
- City Called Heaven Poelinitz PDFDocument6 pagesCity Called Heaven Poelinitz PDFFelipe Bernardo100% (1)
- Professional Parking Management CorporationDocument1 pageProfessional Parking Management CorporationJe RoNo ratings yet
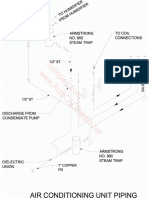
- Steam trap and sewage pump installation detailsDocument28 pagesSteam trap and sewage pump installation detailsMichael Jorge BernalesNo ratings yet
- Bach Quia RespexitDocument3 pagesBach Quia RespexitemilyNo ratings yet
- Drum SizingDocument48 pagesDrum SizingVikram Sharma100% (1)
- Manual Jeep 1977Document2 pagesManual Jeep 1977Calcomanias IndustrialesNo ratings yet
- Typical Details of Skew 11158: Run-InDocument1 pageTypical Details of Skew 11158: Run-InTsang P.K.No ratings yet
- Strike The ViolDocument6 pagesStrike The ViolAnnelies BoonsNo ratings yet
- Noise in Orifice PlateDocument42 pagesNoise in Orifice PlateWesolowskiNo ratings yet
- (J) Jtij: Muhlenberg College EmsDocument3 pages(J) Jtij: Muhlenberg College Emsdandude505No ratings yet
- SATB Junior High Nest EggDocument4 pagesSATB Junior High Nest EggGrace PalmoreNo ratings yet
- KOUSSEVITZKY - Chanson Triste - Pno & Cbajo PDFDocument4 pagesKOUSSEVITZKY - Chanson Triste - Pno & Cbajo PDFNolyNo ratings yet
- You Dont Fool MeDocument11 pagesYou Dont Fool MelukloloNo ratings yet
- Sharpening (Nick Engler) (Z-Library)Document134 pagesSharpening (Nick Engler) (Z-Library)apmcintyre69100% (2)
- Dtic Ada057283Document73 pagesDtic Ada057283docjorseNo ratings yet
- State Bank of India cheque detailsDocument1 pageState Bank of India cheque detailsPramod RawatNo ratings yet
- LACHNER - Op.57 - Prelude - and - Toccata PDFDocument12 pagesLACHNER - Op.57 - Prelude - and - Toccata PDFMichael DelfonteNo ratings yet
- Bax-A Celtic Song CycleDocument14 pagesBax-A Celtic Song CycleteddersrayNo ratings yet
- GhiDocument1 pageGhiQussai BitarNo ratings yet
- Pierre Sancan - Sonatina For Flute and PianoDocument25 pagesPierre Sancan - Sonatina For Flute and Pianosthevan100% (4)
- J.S. Bach - All Jazzed Up! - 12 Favorites Reimagined With A Jazz Flair 49pgDocument49 pagesJ.S. Bach - All Jazzed Up! - 12 Favorites Reimagined With A Jazz Flair 49pgmagali.bachellerie100% (1)
- Nunsense - SynthesizerDocument104 pagesNunsense - SynthesizerLaszlo Molnar100% (1)
- TentDocument24 pagesTenthanyassawy50% (2)
- PDFDocument187 pagesPDFKrishnendu RarhiNo ratings yet
- Tamilnadu Pattadar Pass Book Act 1983Document12 pagesTamilnadu Pattadar Pass Book Act 1983rkjayakumar7639No ratings yet
- Quality assurance plan for Royalton at Capitol CommonsDocument3 pagesQuality assurance plan for Royalton at Capitol CommonsRodelNo ratings yet
- Burton Sonatina PianoDocument23 pagesBurton Sonatina Pianodaitouryou0000No ratings yet
- Parnall Aircraft Since 1914Document121 pagesParnall Aircraft Since 1914Arlene Schwartz100% (2)
- Hertl - ConcertoDocument10 pagesHertl - ConcertoCallum YoungNo ratings yet
- Nancarrow Study No. 15Document8 pagesNancarrow Study No. 15Nick Blue100% (1)
- Ghosts Violin IDocument4 pagesGhosts Violin Ilotoazul2000100% (2)
- Strema PDFDocument43 pagesStrema PDFAthena MontefalcoNo ratings yet
- 1957 4 EngDocument17 pages1957 4 EngTateNo ratings yet
- 35 KLD STP Plant Layout Flow DiagramDocument1 page35 KLD STP Plant Layout Flow DiagramSiva Subramanian C SNo ratings yet
- Artistry Jumps Trompeta 1Document3 pagesArtistry Jumps Trompeta 1Pablo Mazuecos Nievas100% (1)
- Fibich Tři Listy Do PamátníkuDocument2 pagesFibich Tři Listy Do PamátníkuMarkus FlodinNo ratings yet
- Jakub Šimon Jan Ryba - Horn Concerto in Dis Major - Part II, Rondo - Piano PartDocument8 pagesJakub Šimon Jan Ryba - Horn Concerto in Dis Major - Part II, Rondo - Piano PartMcJayJazz100% (1)
- Ashok PatelDocument2 pagesAshok Patelaakash jangalwalaNo ratings yet
- Pages From Dorman Longs - Handbook For Constructional Engineers - 1895-41Document1 pagePages From Dorman Longs - Handbook For Constructional Engineers - 1895-41Fornvald TamasNo ratings yet
- Jordan PDFDocument6 pagesJordan PDFMikey StanleyNo ratings yet
- Mandatory ReportingDocument1 pageMandatory Reportingdandude505No ratings yet
- 95 EVOC Instructor GuideDocument637 pages95 EVOC Instructor Guidedandude505100% (1)
- Legal Aspects of EMSDocument2 pagesLegal Aspects of EMSdandude505No ratings yet
- Home Region 1 Committees Education Resources DP1Document1 pageHome Region 1 Committees Education Resources DP1dandude505No ratings yet
- At The Legal Limit - NYTime..Document6 pagesAt The Legal Limit - NYTime..dandude505No ratings yet
- AD DeathDocument25 pagesAD Deathdandude505No ratings yet
- Advice For New EMT's - Pink..Document12 pagesAdvice For New EMT's - Pink..dandude505No ratings yet
- 1994 Curriculum EmtDocument4 pages1994 Curriculum Emtdandude505No ratings yet
- Boston PCRDocument1 pageBoston PCRdandude505No ratings yet
- EMS On-Call Pay and The FLSADocument3 pagesEMS On-Call Pay and The FLSAdandude505No ratings yet
- New York State FR PCRDocument2 pagesNew York State FR PCRdandude505No ratings yet
- Va Tech Standby ReportDocument1 pageVa Tech Standby Reportdandude505No ratings yet
- Umass Lowell PCRDocument1 pageUmass Lowell PCRdandude505No ratings yet
- Johns Hopkins PCRDocument1 pageJohns Hopkins PCRdandude505No ratings yet
- Va Tech Standby ReleaseDocument2 pagesVa Tech Standby Releasedandude505No ratings yet
- Wustl PCRDocument2 pagesWustl PCRdandude505No ratings yet
- New Hampshire PCRDocument2 pagesNew Hampshire PCRdandude505No ratings yet
- (J) Jtij: Muhlenberg College EmsDocument3 pages(J) Jtij: Muhlenberg College Emsdandude505No ratings yet
- Mount Holyoke PCRDocument1 pageMount Holyoke PCRdandude505No ratings yet
- Mass Event Zone PlanningDocument9 pagesMass Event Zone Planningdandude505No ratings yet
- Rice University's Public Access Defib ProposalDocument13 pagesRice University's Public Access Defib Proposaldandude505No ratings yet
- Laws of The House of GodDocument2 pagesLaws of The House of Goddandude505No ratings yet
- GSA Federal Specification for Star-of-Life Ambulance KKK-A-1822EDocument110 pagesGSA Federal Specification for Star-of-Life Ambulance KKK-A-1822EphilcogabiNo ratings yet
- Treatment Protocols 704.JUNE.08Document161 pagesTreatment Protocols 704.JUNE.08dandude505100% (3)
- Sick Ems HumorDocument13 pagesSick Ems Humordandude505100% (1)
- EmtbnscDocument681 pagesEmtbnscGel OmugtongNo ratings yet
- Continuing Education ManualDocument33 pagesContinuing Education Manualdandude505No ratings yet
- Paramedic Assist Course OutlineDocument6 pagesParamedic Assist Course Outlinedandude505No ratings yet
- 11.1 Antibody Production and VaccinationDocument28 pages11.1 Antibody Production and VaccinationFRENCHONLYNo ratings yet
- Metabolic Reprogramming Due To Hypoxia in Pancreatic Can - 2021 - BiomedicineDocument14 pagesMetabolic Reprogramming Due To Hypoxia in Pancreatic Can - 2021 - BiomedicineAkhmad BajuriNo ratings yet
- Biogenesis and Cell TheoryDocument6 pagesBiogenesis and Cell TheoryScarlet OrigenesNo ratings yet
- The Female Reproductive System: Paul F. Terranova, PH.DDocument17 pagesThe Female Reproductive System: Paul F. Terranova, PH.DMekuriya BeregaNo ratings yet
- ResearchDocument3 pagesResearchapi-380517264No ratings yet
- Basirika Mary Carolyne Latest (Autorecovered)Document5 pagesBasirika Mary Carolyne Latest (Autorecovered)Carol BasirikaNo ratings yet
- PancretitisDocument44 pagesPancretitisMohammad Husni BanisalmanNo ratings yet
- Sleeping Habits by AgeDocument16 pagesSleeping Habits by Ageanon_38352456386% (7)
- Grade 6 - SSES - Science - Q2 - Wk3 - GLAKDocument16 pagesGrade 6 - SSES - Science - Q2 - Wk3 - GLAKMelanie TrinidadNo ratings yet
- Stewart Bitkoff - StarchildDocument9 pagesStewart Bitkoff - StarchildSat FeedNo ratings yet
- Reflex ExercisesDocument43 pagesReflex ExercisesFlori100% (4)
- Group 2. Ectopic PregnancyDocument61 pagesGroup 2. Ectopic PregnancyIvan Laurentine Aceret100% (1)
- Curriculum Vitae: Penata Muda Tk-1 / III BDocument6 pagesCurriculum Vitae: Penata Muda Tk-1 / III BLuciano NawaNo ratings yet
- Organs in The Body Quadrants and RegionsDocument3 pagesOrgans in The Body Quadrants and RegionsDavid HosamNo ratings yet
- Factors Affecting Wound Healing PDFDocument2 pagesFactors Affecting Wound Healing PDFAmandaNo ratings yet
- MODULE 1 & 2 - General Biology 2Document12 pagesMODULE 1 & 2 - General Biology 2John Michael LopezNo ratings yet
- MATERNALDocument32 pagesMATERNALsean blaze100% (1)
- Bci - 3303 - User ManualDocument52 pagesBci - 3303 - User ManualNuno Freitas BastosNo ratings yet
- QuestionDocument16 pagesQuestionellis garciaNo ratings yet
- Hubungan Lama Penggunaan Obat Arv Terhadap Kadar Hemoglobin Pada Penderita Hiv/Aids Di Poli VCT Rsud Prof. Dr. Soekandar Kabupaten MojokertoDocument4 pagesHubungan Lama Penggunaan Obat Arv Terhadap Kadar Hemoglobin Pada Penderita Hiv/Aids Di Poli VCT Rsud Prof. Dr. Soekandar Kabupaten Mojokertofani kurniaNo ratings yet
- Diagnose Cure and Empower Yourself by Currents of Breath - Authored by Acharya Shriram SharmaDocument78 pagesDiagnose Cure and Empower Yourself by Currents of Breath - Authored by Acharya Shriram SharmaGuiding Thoughts- Books by Pandit Shriram Sharma Acharya100% (19)
- e92d86bd42bf566dca92a3495e816e4fDocument8 pagese92d86bd42bf566dca92a3495e816e4fmenchie aquinoNo ratings yet
- NPO GuidelinesDocument2 pagesNPO GuidelinesDan HoNo ratings yet
- Muscle and Nerve McqsDocument6 pagesMuscle and Nerve McqsShan ShaniNo ratings yet
- Self Study Intraoral Anatomy RadiologyDocument80 pagesSelf Study Intraoral Anatomy RadiologydeenmNo ratings yet
- Dipiro 9 (012-047) PDFDocument36 pagesDipiro 9 (012-047) PDFNingrumSindayaniNo ratings yet
- Life Sustaining Processes & Phenomena - Cell MembraneDocument4 pagesLife Sustaining Processes & Phenomena - Cell MembraneS.K.Bhatnagar100% (1)
- Age Drug StudyDocument20 pagesAge Drug StudyLadybelle GototosNo ratings yet
- Weekly Home Learning Plan: Department of EducationDocument19 pagesWeekly Home Learning Plan: Department of EducationMaya CondeNo ratings yet
- Paradox of Self-Conciousness, The - BermúdezDocument17 pagesParadox of Self-Conciousness, The - Bermúdezgheorghe3No ratings yet