You might also like
- Case Analysis: Bipolar 1 Diagnosis & Treatment PlanDocument2 pagesCase Analysis: Bipolar 1 Diagnosis & Treatment PlanJoshua Ringor100% (1)
- Combining CBT and Medication: An Evidence-Based ApproachFrom EverandCombining CBT and Medication: An Evidence-Based ApproachRating: 3 out of 5 stars3/5 (1)
- Assessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.ArchanaaDocument62 pagesAssessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.Archanaadrkadiyala2No ratings yet
- Understanding DelusionsDocument17 pagesUnderstanding DelusionsAnonymous 0ZZTYomaq100% (1)
- Psychiatry 2016Document136 pagesPsychiatry 2016Firas KNo ratings yet
- Prodromal SchizophreniaDocument13 pagesProdromal SchizophreniadizhalfaNo ratings yet
- Bipolar Disorder Assessment and Management 35109814379461Document49 pagesBipolar Disorder Assessment and Management 35109814379461Ana Maria Coral LeitonNo ratings yet
- Psychiatry Capstone 43020 Agitation PsychopharmacologyDocument20 pagesPsychiatry Capstone 43020 Agitation Psychopharmacologyapi-552282470No ratings yet
- Malingering NbiDocument5 pagesMalingering NbiPridina SyadirahNo ratings yet
- Schizoaffective Disorder FactsheetDocument6 pagesSchizoaffective Disorder FactsheetYusnida RahmawatiNo ratings yet
- Guidelines For The Recognition and Management of Mixed DepressionDocument17 pagesGuidelines For The Recognition and Management of Mixed DepressionGino Garavito Criollo100% (1)
- PSYCH 003 - Diagnosis and Management of Thought DisordersDocument9 pagesPSYCH 003 - Diagnosis and Management of Thought DisordersKaye NeeNo ratings yet
- Psychosomatic in Psychiatry - UNTAD 2012Document18 pagesPsychosomatic in Psychiatry - UNTAD 2012Fadjarr WahidNo ratings yet
- Diagnosis & Classification in Psychiatry: Organizing Principles and Current Classifications/TITLEDocument22 pagesDiagnosis & Classification in Psychiatry: Organizing Principles and Current Classifications/TITLEKholoud KholoudNo ratings yet
- App2Document3 pagesApp2Johnykutty JosephNo ratings yet
- Depression PsychoticDocument10 pagesDepression Psychoticharumimiaomiao_198930% (1)
- 7 .2 Schizoaffective Disorder: Dialectical Behavior TherapyDocument4 pages7 .2 Schizoaffective Disorder: Dialectical Behavior TherapyRevan ArthaNo ratings yet
- Neuroanatomy For The Psychiatrist: Textbook of PsychiatryDocument37 pagesNeuroanatomy For The Psychiatrist: Textbook of Psychiatrykrysdana22No ratings yet
- (PSYCH) 4.01 Forensic Psychiatry - Dr. Cruz PDFDocument6 pages(PSYCH) 4.01 Forensic Psychiatry - Dr. Cruz PDFMon Kristoper CastilloNo ratings yet
- Ketamine-Assisted Psychotherapy:: A Practical Guide For Medical ProvidersDocument40 pagesKetamine-Assisted Psychotherapy:: A Practical Guide For Medical ProvidersMannu MoguritoNo ratings yet
- History Taking and Mental State Exam for PsychosisDocument10 pagesHistory Taking and Mental State Exam for PsychosisNathan T. CheungNo ratings yet
- Major Depressive Disorder: Assessment, Diagnosis, Planning and InterventionsDocument25 pagesMajor Depressive Disorder: Assessment, Diagnosis, Planning and InterventionsCath CathNo ratings yet
- Notes On PsychiatryDocument10 pagesNotes On PsychiatryMark VillenaNo ratings yet
- General Questions (Mood Disorder)Document5 pagesGeneral Questions (Mood Disorder)Zubair MushtaqNo ratings yet
- Schizoaffective Disorder in The DSM 5 PDFDocument5 pagesSchizoaffective Disorder in The DSM 5 PDFpipiitopandabamboo247No ratings yet
- The Clinical Interview and AssessmentDocument6 pagesThe Clinical Interview and AssessmentIoana Antonesi100% (1)
- Psychiatric InterviewDocument54 pagesPsychiatric InterviewzarrarNo ratings yet
- CEP BPSD Discussion Guide ENG RFCG Updated2019 PDFDocument8 pagesCEP BPSD Discussion Guide ENG RFCG Updated2019 PDFM.DalaniNo ratings yet
- Individual Music Therapy For Depression: Randomised Controlled TrialDocument9 pagesIndividual Music Therapy For Depression: Randomised Controlled TrialSarah HarahapNo ratings yet
- Alcohol Use Disorder MGMT Guideline - Final... EstDocument83 pagesAlcohol Use Disorder MGMT Guideline - Final... EstMuluken TesfayeNo ratings yet
- Psychiatry Notes - Defenses MechanismsDocument2 pagesPsychiatry Notes - Defenses MechanismsLiSenNo ratings yet
- Psychiatry history taking and case formulation templateDocument11 pagesPsychiatry history taking and case formulation templateNicholasNo ratings yet
- Symptom Overreporting and Dissociative Experiences: A Qualitative ReviewDocument13 pagesSymptom Overreporting and Dissociative Experiences: A Qualitative ReviewKamiNo ratings yet
- Disorders RushedDocument40 pagesDisorders Rushedapi-391411195No ratings yet
- Early Onset Psychotic DisordersDocument51 pagesEarly Onset Psychotic Disordersdrkadiyala2100% (1)
- Cha, Danielle S. - Mcintyre, Roger S - Cognitive Impairment in Major Depressive Disorder - Clinical Relevance, Biological Substrates, and Treatment Opportunities-Cambridge University Press (2016)Document384 pagesCha, Danielle S. - Mcintyre, Roger S - Cognitive Impairment in Major Depressive Disorder - Clinical Relevance, Biological Substrates, and Treatment Opportunities-Cambridge University Press (2016)Vissente TapiaNo ratings yet
- PPDGJ 3 PDFDocument279 pagesPPDGJ 3 PDFtri ummiNo ratings yet
- Biological Aspects of OCD SeminarDocument60 pagesBiological Aspects of OCD Seminarneha mattikoppaNo ratings yet
- Intro Child PsychiatryDocument122 pagesIntro Child PsychiatryayunisallehNo ratings yet
- (Sept 14, 12) Schizophrenia and Other Psychotic DisordersDocument56 pages(Sept 14, 12) Schizophrenia and Other Psychotic DisordersuculucullNo ratings yet
- ILOCOS TRAINING AND REGIONAL MEDICAL CENTER PSYCHIATRY ROTATIONDocument21 pagesILOCOS TRAINING AND REGIONAL MEDICAL CENTER PSYCHIATRY ROTATIONKristine BoholstNo ratings yet
- PSYCH 1.2B Criteria Mood DisordersDocument5 pagesPSYCH 1.2B Criteria Mood DisordersZaza100% (1)
- Comprehensive Psychiatric EvaluationDocument5 pagesComprehensive Psychiatric EvaluationfrankieNo ratings yet
- Rating Scales for Assessing Bipolar Disorder SymptomsDocument14 pagesRating Scales for Assessing Bipolar Disorder SymptomsDivia RainaNo ratings yet
- Psychiatry History & Suicide Risk Assessment TemplatesDocument32 pagesPsychiatry History & Suicide Risk Assessment TemplatesDuncan Jackson100% (1)
- Behavioral Management of HipersomniaDocument7 pagesBehavioral Management of HipersomniaHernán MarínNo ratings yet
- Psychiatry: ' ' Psychology 538 ' Pathology 540 ' Pharmacology 556Document24 pagesPsychiatry: ' ' Psychology 538 ' Pathology 540 ' Pharmacology 556Brush LowdryNo ratings yet
- Signs and symptoms of mental illnessDocument3 pagesSigns and symptoms of mental illnessSunny MaeNo ratings yet
- Case Study 5 - 8 - PsychosisDocument17 pagesCase Study 5 - 8 - PsychosisanojanNo ratings yet
- Mood Disorder Management ChartDocument1 pageMood Disorder Management ChartechopennerNo ratings yet
- Treatment Resistant OcdDocument70 pagesTreatment Resistant Ocddrkadiyala2100% (1)
- The Neuroscience of Clinical PsychiatryDocument334 pagesThe Neuroscience of Clinical PsychiatryThaíse MondinNo ratings yet
- Shared Psychotic Disorder - NCBIDocument8 pagesShared Psychotic Disorder - NCBI5KevNo ratings yet
- Clinical Psychological Science 2016 Beck 2167702616628523Document24 pagesClinical Psychological Science 2016 Beck 2167702616628523memo leyNo ratings yet
- Toolkit Risk Assessment Final1Document8 pagesToolkit Risk Assessment Final1MalkOo AnjumNo ratings yet
- Early PsychosisDocument118 pagesEarly Psychosissolomon1234567100% (1)
- Understanding the Person Beyond the IllnessDocument21 pagesUnderstanding the Person Beyond the IllnessMuluken TesfayeNo ratings yet
- APA - DSM 5 Depression Bereavement Exclusion PDFDocument2 pagesAPA - DSM 5 Depression Bereavement Exclusion PDFDaniel NgNo ratings yet
- Depression in Older PeopleDocument4 pagesDepression in Older PeopleAlina AlinaNo ratings yet
- Teenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenFrom EverandTeenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenNo ratings yet
- Factors Affecting Language LearnerDocument13 pagesFactors Affecting Language LearnermisterashNo ratings yet
- Curriculum Information For WebsiteDocument2 pagesCurriculum Information For Websiteapi-263335251No ratings yet
- CHE 320 Homework #1 Ethics GuidelinesDocument3 pagesCHE 320 Homework #1 Ethics Guidelineslulu100% (1)
- Final Project 111Document25 pagesFinal Project 111Maleeha AyubiNo ratings yet
- Spitler Jordan Resume RealDocument2 pagesSpitler Jordan Resume Realapi-284829624No ratings yet
- Kingdom of Saudi Arabia The National Commission for Academic Accreditation & Assessment COURSE REPORTDocument7 pagesKingdom of Saudi Arabia The National Commission for Academic Accreditation & Assessment COURSE REPORTtledraa4477No ratings yet
- Manzoor Solangi Curriculum VitaeDocument8 pagesManzoor Solangi Curriculum VitaeAqil SolangiNo ratings yet
- Student Council 251011Document13 pagesStudent Council 251011eholmes80No ratings yet
- Curriculum-Vitae: Master's of Science (M.SC)Document2 pagesCurriculum-Vitae: Master's of Science (M.SC)Anonymous ByrWdkceKoNo ratings yet
- Guidelines For 2023 DFOTDocument69 pagesGuidelines For 2023 DFOTEizen DivinagraciaNo ratings yet
- TLE9 - Q2 - Mod4 Week 8Document24 pagesTLE9 - Q2 - Mod4 Week 8Ceasar Ryan AsuncionNo ratings yet
- Distance Education in India: Problems or Barriers To LearningDocument9 pagesDistance Education in India: Problems or Barriers To LearningcpmrNo ratings yet
- Updated ResumeDocument1 pageUpdated Resumeapi-354315166No ratings yet
- ICT Officer (Infra) Profile: Various Locations Grade: Junior (P2) and Mid (P3) Level PositionsDocument2 pagesICT Officer (Infra) Profile: Various Locations Grade: Junior (P2) and Mid (P3) Level Positionsسعيد نورحوسين اخمدNo ratings yet
- The Life and Works of Rizal The Life and Works of RizalDocument100 pagesThe Life and Works of Rizal The Life and Works of RizalRodolfo jr B. ValdenarroNo ratings yet
- Wake Forest Faculty Senate Ad Hoc Committee Report On Koch Foundation FundingDocument38 pagesWake Forest Faculty Senate Ad Hoc Committee Report On Koch Foundation FundingThe College FixNo ratings yet
- Utopian Discourse and Practices in Social MovementsDocument2 pagesUtopian Discourse and Practices in Social Movementsviva_bourdieuNo ratings yet
- Human Values and Community Outreach SyllabusDocument5 pagesHuman Values and Community Outreach SyllabusIshika SinghalNo ratings yet
- Infiniband Network ArchitectureDocument0 pagesInfiniband Network ArchitectureGeorgehanyNo ratings yet
- Modernism's Debt to Anthropology and ArchaeologyDocument13 pagesModernism's Debt to Anthropology and ArchaeologymagwanwanNo ratings yet
- Apollo Engineering College DetailsDocument1 pageApollo Engineering College DetailsKARNA JayNo ratings yet
- PMC Module 4Document7 pagesPMC Module 4Manahil Naeem100% (1)
- Undergraduate Prospectus OxfordDocument168 pagesUndergraduate Prospectus OxfordShawn TanNo ratings yet
- Educational PsychologyDocument10 pagesEducational PsychologysimonNo ratings yet
- MATH 6 - (SIM) Comparing FractionsDocument24 pagesMATH 6 - (SIM) Comparing FractionsTricia Nievera Dizon100% (1)
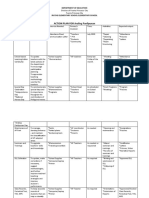
- ACTION PLAN FOR Araling Panlipunan: Department of EducationDocument4 pagesACTION PLAN FOR Araling Panlipunan: Department of EducationJaz ZeleNo ratings yet
- Try To Remember - Psychiatry's Clash Over Meaning, Memory, Mind - P. McHugh (Dana, 2008) BBSDocument293 pagesTry To Remember - Psychiatry's Clash Over Meaning, Memory, Mind - P. McHugh (Dana, 2008) BBSAmelia Negoi100% (1)
- Syllabus Obe - Operations Management-Tqm Revised Flex 823221Document17 pagesSyllabus Obe - Operations Management-Tqm Revised Flex 823221Jayar DimaculanganNo ratings yet
- CV For Dcis Elizeus MushongiDocument4 pagesCV For Dcis Elizeus Mushongijonas msigalaNo ratings yet
- 23 PA Semifinalists-NatlMeritProgramDocument5 pages23 PA Semifinalists-NatlMeritProgramPennLiveNo ratings yet