Professional Documents
Culture Documents
Alentorn-Geli Et Al 2009. Prevention of Non-Contact Anterior Cruciate Ligament Injuries in Soccer Players. Part 1
Uploaded by
Craig Stewart0 ratings0% found this document useful (0 votes)
223 views25 pagesACL paper
Original Title
Alentorn-Geli Et Al 2009. Prevention of Non-contact Anterior Cruciate Ligament Injuries in Soccer Players. Part 1
Copyright
© © All Rights Reserved
Available Formats
PDF, TXT or read online from Scribd
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentACL paper
Copyright:
© All Rights Reserved
Available Formats
Download as PDF, TXT or read online from Scribd
0 ratings0% found this document useful (0 votes)
223 views25 pagesAlentorn-Geli Et Al 2009. Prevention of Non-Contact Anterior Cruciate Ligament Injuries in Soccer Players. Part 1
Uploaded by
Craig StewartACL paper
Copyright:
© All Rights Reserved
Available Formats
Download as PDF, TXT or read online from Scribd
You are on page 1of 25
KNEE
Prevention of non-contact anterior cruciate ligament injuries
in soccer players. Part 1: Mechanisms of injury
and underlying risk factors
Eduard Alentorn-Geli Gregory D. Myer
Holly J. Silvers Gonzalo Samitier Daniel Romero
Cristina Lazaro-Haro Ramon Cugat
Received: 5 October 2008 / Accepted: 18 April 2009 / Published online: 19 May 2009
Springer-Verlag 2009
Abstract Soccer is the most commonly played sport in
the world, with an estimated 265 million active soccer
players by 2006. Inherent to this sport is the higher risk of
injury to the anterior cruciate ligament (ACL) relative to
other sports. ACL injury causes the most time lost from
competition in soccer which has inuenced a strong
research focus to determine the risk factors for injury. This
research emphasis has afforded a rapid inux of literature
dening potential modiable and non-modiable risk fac-
tors that increase the risk of injury. The purpose of the
current review is to sequence the most recent literature that
reports potential mechanisms and risk factors for non-
contact ACL injury in soccer players. Most ACL tears in
soccer players are non-contact in nature. Common playing
situations precluding a non-contact ACL injury include:
change of direction or cutting maneuvers combined with
deceleration, landing from a jump in or near full extension,
and pivoting with knee near full extension and a planted
foot. The most common non-contact ACL injury mecha-
nism include a deceleration task with high knee internal
extension torque (with or without perturbation) combined
with dynamic valgus rotation with the body weight shifted
over the injured leg and the plantar surface of the foot xed
at on the playing surface. Potential extrinsic non-contact
ACL injury risk factors include: dry weather and surface,
and articial surface instead of natural grass. Commonly
purported intrinsic risk factors include: generalized and
specic knee joint laxity, small and narrow intercondylar
notch width (ratio of notch width to the diameter and cross
sectional area of the ACL), pre-ovulatory phase of men-
strual cycle in females not using oral contraceptives,
decreased relative (to quadriceps) hamstring strength and
recruitment, muscular fatigue by altering neuromuscular
control, decreased core strength and proprioception, low
trunk, hip, and knee exion angles, and high dorsiexion
of the ankle when performing sport tasks, lateral trunk
displacement and hip adduction combined with increased
knee abduction moments (dynamic knee valgus), and
increased hip internal rotation and tibial external rotation
with or without foot pronation. The identied mechanisms
and risk factors for non-contact ACL injuries have been
mainly studied in female soccer players; thus, further
research in male players is warranted. Non-contact ACL
injuries in soccer players likely has a multi-factorial eti-
ology. The identication of those athletes at increased risk
may be a salient rst step before designing and imple-
menting specic pre-season and in-season training pro-
grams aimed to modify the identied risk factors and to
decrease ACL injury rates. Current evidence indicates that
E. Alentorn-Geli G. Samitier C. Lazaro-Haro R. Cugat
Artroscopia G.C., Hospital Quiron, Barcelona, Spain
G. D. Myer
Sports Medicine Biodynamics Center and Human Performance
Laboratory, Cincinnati Childrens Hospital Medical Center,
Cincinnati, OH, USA
G. D. Myer
Rocky Mountain University of Health Professions,
Provo, UT, USA
H. J. Silvers
Santa Monica Orthopaedic Sports Medicine/Research
Foundation, Santa Monica, CA, USA
D. Romero
Physical Therapy School, Blanquerna University,
Barcelona, Spain
E. Alentorn-Geli (&)
Dr. Ramon Cugats Ofce, Hospital Quiron,
Plaza Alfonso Com n 5-7, 08023 Barcelona, Spain
e-mail: ealentorngeli@gmail.com
1 3
Knee Surg Sports Traumatol Arthrosc (2009) 17:705729
DOI 10.1007/s00167-009-0813-1
this crucial step to prevent ACL injury is the only option to
effectively prevent the sequelae of osteoarthritis associated
with this traumatic injury.
Keywords Prevention Non-contact ACL injury
Soccer
Introduction
Soccer is the most commonly played sport in the world
[36], with an estimated 265 million active soccer players
participating in the sport as of 2006 [47]. The international
popularity continues to rise as indicated by the 23 million
increase in active soccer players compared to 8 years ago.
Despite the predominance of male players (90%), the
current trends suggest that the continued rise in participa-
tion is mainly from the increases in females, who choose to
participate in soccer [47]. Despite the suggestion that it is
considered a relatively safe sport for males, female soccer
players are at up to six times greater risk for sustaining an
anterior cruciate ligament (ACL) tear than their male
counterparts [3]. The increased participation and increased
risk of knee injury especially among females, has led to a
substantial increase in number of reported ACL injuries in
the sport. The reported incidence of ACL injury ranges
from 0.06 to 3.7 per 1,000 h of active soccer playing (game
and training) [15, 45], accounting for thousands of ACL
tears each year. It is also estimated that the occurrence of
ACL injuries on a soccer team expressed as a percentage of
all injuries on that team is 1.3% for males, and 3.7% for
females [156].
While there has been recent scientic efforts focused on
ACL injury treatment strategies, it is well established that
surgical reconstruction does not reduce the increased risk
for developing knee osteoarthritis after a traumatic knee
injury is sustained [42, 106, 120, 134]. In addition, ACL
injury is often concomitant with a meniscus tear, and
several authors found that this type of meniscus injury is
also an indicated risk factor for tibiofemoral osteoarthritis
[120, 136]. Beyond the short- and long-term physical
impairments, ACL injury also causes personal and pro-
fessional impairment for athletes, with a high economic
cost for both athletes and institutions [56, 57, 194].
Therefore, the prevention of non-contact ACL injuries is of
major relevance in sports traumatology.
The identied gender bias for non-contact ACL injuries
and associated detrimental effects in female soccer players
have served as the impetus for research efforts to dene the
mechanisms of ACL injury and to delineate the most
relevant underlying risk factors that contribute to these
mechanisms. It is suggested that once these gender-related
mechanisms and associated risk factors are dened more
efcient neuromuscular training protocols can be instituted
to high-risk populations [130]. The purpose of this article is
twofold: rst, to provide a current review of the literature
to dene the most probable mechanisms of non-contact
ACL injuries and second, to delineate the role that envi-
ronmental, anatomical, hormonal, neuromuscular, and
biomechanical risk factors may contribute to the portrayed
mechanisms.
We employed Medline database for literature search
purposes. All articles under the topics ACL prevention,
ACL injury risk factors, non-contact ACL injuries,
mechanisms of ACL injuries, ACL injuries in soccer
players, and injuries in soccer from 1985 to 2008 were
considered of potential interest for this review. Articles
which included an intervention were excluded from this
review. In addition, each reference list from the identied
articles was cross-checked to verify that relevant articles
were not missed for the current review.
Mechanisms of non-contact ACL injuries in soccer
players
The study of mechanisms of non-contact ACL injuries in
soccer players is based on several methodological
approaches: interviews with injured players, video analysis,
clinical studies (where the clinical joint damage is studied
to understand the mechanism of the injury), in vivo studies
(measuring ligament strain or forces to understand liga-
ment loading patterns), cadaver studies, mathematical
modeling and simulation of injury situations, or measure-
ments/estimation from close to injury situations [93,
156].
We considered non-contact ACL tears to those injuries
with no physical contact with other players at the time of
injury. The rate for non-contact ACL injuries ranges from
70 to 84% of all ACL tears in both female and male ath-
letes [17, 45, 117, 137, 138]. Most ACL tears in soccer
occur in the absence of player-to-player (body-to-body)
contact [45]. Despite Arendt and Dick [3] found an equal
rate of contact versus non-contact mechanisms on ACL
injuries among male soccer players, it is overall accepted
that the vast majority of ACL tears occur through a non-
contact mechanism in both male and female athletes.
The most common playing scenarios precluding a non-
contact ACL injury include: change of direction or cutting
maneuvers combined with deceleration, landing from a
jump in or near full extension, pivoting with knee near full
extension and a planted foot [17, 45, 46]. Other described
mechanisms of ACL tears included knee hyperextension
and hyperexion [53, 63, 176]. These playing situations
involve knee valgus, varus, internal rotation, and external
rotation moments, and anterior translation force [17, 110,
706 Knee Surg Sports Traumatol Arthrosc (2009) 17:705729
1 3
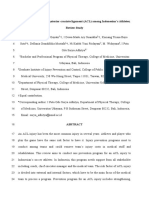
111, 141, 182, 194]. The anterior translation force, spe-
cically at exion angles around 2030, may be the most
detrimental isolated force associated with ACL injury, and
is often identied as a contributing factor to ACL injury
mechanisms [10, 17, 110, 117, 194]. However, cadaveric
studies indicate that a combination of forces produces a
higher strain on the ACL than isolated motions and torques.
Thus, pure knee internal rotation, external rotation, valgus,
and varus moments do not strain ACL [10] to the magni-
tude of combined rotations such as an anteriorly directed
force added to valgus or internal rotation (Fig. 1) [10, 110].
Boden et al. utilized retrospective video analysis in
attempt to dene the most common kinematic positions
related to ACL injury during competitive play. They
reported a lower extremity alignment associated with non-
contact ACL injury in which the tibia was externally
rotated, the knee was close to full extension, the foot was
planted during deceleration with valgus collapse at the
knee [17]. More recent reports have also indicated this
common mechanism of valgus collapse at the knee in
female athletes [94, 141]. Teitz reported very similar
deceleration positions in the majority of the ACL injuries
she examined; however, she also indicated that most often
the center of mass of the body was behind and away from
the base of support (area of foot to ground contact) [177].
Thus, there is mounting evidence that the most common
non-contact injury mechanism of injury in female athletes
occurs during a deceleration task with high knee internal
extension torque (with or without a visual perturbation)
combined with dynamic valgus rotation with the body
weight shifted over to the injured leg and the plantar sur-
face of the foot xed at on the playing surface [17, 94,
141, 177]. Interestingly, both male and female athletes may
demonstrate similar body alignment during competitive
play without succumbing to an ACL injury. Thus, it is
crucial to determine the underlying risk factors that con-
tribute to an increased propensity for this high-risk posi-
tion. Ultimately, it is the goal of clinicians and researchers
to determine the risk factors that preclude the actual ACL
injury.
Risk factors
Risk factors have been divided into extrinsic (those outside
the body) and intrinsic factors (those within the body)
[128]. However, other classication schemes do exist when
considering non-contact ACL injuries. In this article, risk
factors will be divided into environmental, anatomical,
hormonal, neuromuscular, and biomechanical, relative to
the guidelines established by the Hunt Valley meeting [62].
Environmental risk factors
Overview
Environmental factors include those aspects extrinsic to the
athlete such as sport, playing surface, weather character-
istics, the type of footwear, the shoe to surface interaction
(friction coefcient). There is a clear lack of randomized
controlled studies regarding environmental factors in soc-
cer players. The existing evidence on environmental factors
related to ACL injuries is mainly based on American
Football, Australian Football, or indoor sports like handball
[20, 21, 96, 143, 144, 162]. American Football, Australian
Football, and soccer are contact sports sharing some
common features regarding ground characteristics, shoe
choice, and many playing situations like cutting, landing,
or a change of direction with high acceleration and/or
deceleration components.
Weather
A relationship between meteorological conditions and the
incidence of ACL injuries was noted in Australian Football
by Scranton et al. [162]. The authors found a higher ACL
injury rate on natural grass during dry compared to wet
conditions. However, the report did not control for weather
conditions where injuries did not occur. Subsequently,
Orchard et al. [144] found that high water evaporation in the
month before the match and low rainfall in the year before
Fig. 1 ACL injury through a combination of knee valgus and anterior tibial translation force during a side-cut maneuver in soccer players
Knee Surg Sports Traumatol Arthrosc (2009) 17:705729 707
1 3
the match in Australian Football were signicantly associ-
ated with a higher incidence of ACL injuries. It has been
postulated that the high rate of ACL tears during dry con-
ditions on natural grass could be explained by an increased
friction and torsional resistance from the shoe-surface
interface compared to wet conditions [21, 66]. Similarly,
Orchard et al. [145] found that cold weather was associated
with lower knee and ankle injury risk, including ACL tears,
in outdoor sports completed on both natural grass and arti-
cial turf. Correspondingly, Torg et al. [179] demonstrated
that an increase in turf temperature, in combination with
cleat characteristics, affects shoesurface interface friction
and potentially places the athletes knee and ankle at risk of
injury. Studies regarding weather conditions may be limited
without their control for other potential confounding factors
like intrinsic biomechanical factors, neuromuscular condi-
tioning, or hydration status of athletes, among others.
Shoesurface interaction
Surface characteristics themselves, irrespective of whether
they are inuenced by weather conditions, have an impact on
ACL injury rates. Orchard et al. found in Australian Football
that games and practices played on rye grass appeared to
have a lower incidence of ACL tears compared to Bermuda
grass. It was hypothesized that Bermuda grass, with a thicker
thatch layer, would increase shoe-surface traction secondary
to the fact that boot cleats would be better gripped by the
surface [143]. Also, grass cover and root density has been
associated with a greater shoesurface traction. Articial
surface is generally associated with higher shoesurface
traction than natural grass [142], and thus with a higher risk
for ACL tears. In general, articial turf has a higher peak
deceleration for high-energy impacts [101], and the greater
the surface hardness the greater the ground reaction force.
Bowers and Martin [20] demonstrated that the impact
absorption of articial turf decreases as the age of the surface
increases. Additionally, Arnason et al. [6] found a higher
injury rate for soccer played on articial turf compared to
natural grass and gravel, and a higher injury rate on natural
grass compared to gravel. Moreover, Hoff and Martin [77]
found a sixfold increase in the injuries reported in indoor
soccer compared to outdoor. Both articial turf and indoor
ooring may have an increased coefcient of friction. An
increased shoesurface coefcient of friction or traction may
potentially improve performance, but may also increase the
risk for ACL injuries. Ford et al. [50] demonstrated that the
playing surface (grass vs. turf) signicantly alters plantar
loading during cutting in male football players. In addition,
Burkhart et al. [25] reported in a prospective research study
that an athlete, who landed with an increased heel to at-foot
loading mechanism was more likely to sustain to a non-
contact ACL injury during competitive play. In summary,
factors inuencing shoesurface traction include: ground
hardness, ground coefcient of friction, ground dryness,
grass cover and root density, length of cleats on player boots
and relative speed of the game. These factors may contribute
to the inciting mechanism of ACL injury [142]. Unfortu-
nately, no denitive conclusions can be drawn regarding the
safest type of playing surface in soccer players. Recent
studies found no differences in the incidence, severity, nature
or cause of injuries in male and female soccer players
when comparing articial turf versus natural grass [40, 54,
55, 173].
Footwear
Footwear is considered a potential risk factor for ACL tears,
since it modulates foot xation during the game. It has been
shown that the number, length and cleat placement was
associated with the chance of ACL injuries [158]. Lambson
et al. prospectively evaluated ACL injury incidence in
American Football depending on the shoe design. The
authors found a higher risk of ACL tears for the edge
cleat design (longer irregular cleats placed at the peripheral
margin of the lateral sole with a number of smaller pointed
cleats positioned medially). This cleat placement may have
provided signicantly higher torsional resistance compared
to other types of cleats [96]. However, Mitchell et al. [123]
reported that the foot mechanics and possibly the footshoe
interaction were not related to the propensity to demonstrate
high knee load kinematics that are related to increased risk
of ACL injury. While there is no current consensus relating
the environmental and shoesurface interaction to risk
factors that contribute to ACL injury, the initial evidence
reported above suggest that these factors may contribute to
the described mechanisms of ACL injury. However,
potential confounding factors (i.e., biomechanical, neuro-
muscular, hydration status, among others) need to be better
controlled in environmental risk factors studies. Also, some
conclusions are not completely generalizable to soccer
players as they were made for Australian Football (i.e., the
increased risk for wet conditions and for Bermuda grass
compared to rye grass).
Anatomical risk factors
Overview
There is no denitive evidence that any anatomical risk
factors are directly correlated with an increased rate of non-
contact ACL injury with respect to age and gender [62].
Moreover, the preventive potential of anatomical factors
is relatively small, since anatomy is difcult to modify
(Table 1). However, there are anatomical considerations
708 Knee Surg Sports Traumatol Arthrosc (2009) 17:705729
1 3
that should be considered in order to ascertain an adequate
understanding of the implicated pathomechanics, which
may lead to an ACL tear. Body mass index, generalized
and specic knee joint laxity, and Q-angle anatomical
factors were investigated involving soccer players. In
contrast, evidence on intercondylar notch width, ACL size
and strength, pelvis and trunk anatomy, posterior tibial
slope, and foot pronation is not based on soccer players.
Relative mass
Some authors have observed increased body mass index as
a risk factor for ACL injuries, especially among female
adolescent soccer players [24, 71], college recreational
athletes [22, 62], and female army recruits [180]. It was
postulated that an increased body mass index would result
in a more extended lower extremity position with
decreased knee exion upon landing [22, 62]. Unfortu-
nately, conicting results do exist when completing a fur-
ther review of the literature, and other authors found no
impact of body mass index on ACL injuries in female
athletes, including soccer players [54, 55, 91, 95, 146].
Joint laxity
Generalized joint laxity is purported as a risk factor that
could potentially place the athlete at an increased risk of
ACLinjury. Soderman et al. [170] investigated the risk of leg
Table 1 Summary of modiable and non-modiable intrinsic risk factors related to increased risk of ACL injury
Modiable risk factors Non-modiable risk factors Potential control or treatment technique
Anatomical BMI Monitor and control relative body mass
Femoral notch index (ACL size) N-M training targeted to decrease other risk factors
Knee recurvatum N-M training targeted to improve dynamic knee
exion
General joint laxity N-M training targeted to improve joint stiffness
Family history (genetic predisposition) N-M training targeted to decrease other risk factors
Prior injury history Full physical rehabilitation following injury
Developmental and
hormonal
Sex, female N-M training prior to onset of risk factors
Pubertal and post-pubertal maturation
status
N-M training prior during pre-puberty
Preovulatory menstrual status Oral contraceptives in females
a
ACL tensile strength N-M training targeted to decrease other risk factors
Neuromuscular shunt N-M training targeted to improve neuromuscular
control
Biomechanical Knee abduction N-M training targeted to improve coronal plane
loads
Anterior tibial shear N-M training targeted to improve dynamic knee
exion
Lateral trunk motion N-M training targeted to improve trunk strength and
control
Tibial rotation N-M training targeted to control transverse motions
and inuence sagittal plane deceleration
mechanics
Dynamic foot
pronation
Foot orthoses
Fatigue resistance Strength and conditioning training
Ground reaction forces N-M training targeted to improve force absorption
strategies
Neuromuscular Relative hamstring
recruitment
N-M training targeted to improve hamstring strength
and recruitment
Hip abduction strength N-M training targeted to improve hip strength and
recruitment
Trunk proprioception N-M training targeted to improve trunk strength and
control
N-M neuromuscular training
a
Pilot evidence indicates it might be a potential control strategy
Knee Surg Sports Traumatol Arthrosc (2009) 17:705729 709
1 3
injuries among female soccer players presenting with gen-
eral joint laxity and knee hyperextension (among other risk
factors). The investigators demonstrated a signicantly
increased risk of leg injuries (but not specic ACL injuries)
among athletes with generalized joint laxity and knee
hyperextension. Uhorchak [180] specically reported a 2.8
times greater risk of non-contact ACL injury in the United
States Military Academy cadets with generalized joint laxity
compared to normal joint laxity subjects in a prospective 4-
year evaluation. There was also a greater risk of non-contact
ACLinjury for females with a higher anteriorposterior knee
joint laxity but not for males. The authors also found a sig-
nicantly higher generalized joint laxity and anteriorpos-
terior knee joint laxity in females compared to males. It was
also retrospectively observed that ACL-injured subjects had
a signicantly greater generalized joint laxity in comparison
to healthy age-matched controls [154]. The same authors
report a 78.7% proportion of genu recurvatum among ACL-
injured subjects versus the 37%in the control group. Specic
knee joint laxity has been related to increased valgusvarus
and internalexternal rotation knee laxity with an increased
functional valgus collapse [51, 72, 167] observed in young
female soccer and basketball players in comparison to their
male counterparts. Specic knee joint laxity is greater in
healthy females compared to males [149, 180], and knee
joint laxity measured as hyperextension and anteriorpos-
terior tibiofemoral translation has been recently related to a
higher risk of ACL injuries among female soccer and bas-
ketball players [133]. Therefore, it seems that knee joint
laxity could alter dynamic lower extremity motions and
loads a multiplanar fashion, which may place ligaments to a
higher risk of rupture. Ergun et al. compared 44 healthy male
soccer players (from local leagues) with 44 healthy controls
(age- and sex-matched sedentary medical students and hos-
pital staff with no history of regular sports activity) in the
sagittal plane for knee laxity and isokinetic muscle strength.
Soccer players demonstrated signicantly less anterior
and anteriorposterior knee laxity and higher isokinetic
strength of the knee exors and extensors compared to sed-
entary controls. Isokinetic strength difference was found to
be higher for the exor muscle group of the knee [43]. More
studies are needed to elucidate the real role of generalized
joint laxity and specic knee joint laxity in the risk of ACL
tears, specically controlling for neuromuscular factors.
Pelvis and trunk
The female athletes biomechanical prole is a complex
system, and the knee joint should not be considered as an
isolated component to evaluate risk factors for ACL injury.
As a consequence, the trunk, the pelvis, the hip, and the
ankle should be considered in their relationship to resultant
knee joint mechanics. Anterior pelvic tilt places the hip into
an internally rotated, anteverted, and exed position, which
lengthens and weakens the hamstrings and changes moment
arms of the gluteal muscles [37]. Hamstring muscles are
important to prevent static and dynamic genu recurvatum
and to prevent anterior tibial displacement. Gluteal muscles
are important to assist hip exion (gluteus maximus) and to
prevent a dynamic valgus collapse (gluteus medius).
Anterior pelvic tilt also increases genu valgus and subtalar
pronation [167]. Genu recurvatum, excessive navicular
drop, and excessive subtalar pronation are more commonly
found in ACL-injured subjects compared to non-ACL-
injured subjects, all factors that have also been related to
ACL preloading [107]. Nevertheless, the exact degree of
anterior pelvic tilt that directly correlates to ACL injury
remains controversial. It is debated whether the risk is
caused by the altered pelvic position itself, or by the func-
tional malalignment it creates [167]. In any case, clinicians
should be mindful that pelvic stability is a key factor for
lower extremity kinematics and kinetics [199, 200].
Torsional anatomic abnormalities are also related to
altered lower extremity biomechanics. Femoral torsion is
dened as the angle between the axis of the femoral neck
and a transverse line through the posterior aspect of fem-
oral condyles [122]. Femoral anteversion, an increase in
the mentioned angle, may cause an inefciency of the
gluteus medius through a decrease in the internal moment
arm [167]. A weak gluteus medius may inuence dynamic
valgus collapse because of the muscles inability to keep
the hip abducted, especially during weight-bearing activi-
ties such as landing, cutting, or changing direction. The
toe-in gait demonstrates the femoral torsion position and is
often associated with increased external tibial torsion [121,
122], which has been related to the functional valgus col-
lapse at the knee joint [141].
The inuence of pelvis and trunk mechanics on non-
contact ACL injuries in soccer players needs to be better
characterized. Thus, studies examining the specic role of
the pelvis and trunk in the non-contact ACL injuries in
soccer players are warranted.
Q-angle
Another suggested anatomical factor that has been related
to an increased risk of ACL injury is the quadriceps angle
(Q-angle). The Q-angle is the angle formed by a line
directed from the anterior-superior iliac spine to central
patella and a second line directed from the central patella to
tibial tubercle. A high Q-angle may alter the lower limb
biomechanics [65, 124] and place the knee at a higher risk
to static and dynamic valgus stresses [23]. It was observed
that female basketball players with knee injuries had a
mean Q-angle greater than non-injured players [164].
However, other authors found that static Q-angle measures
710 Knee Surg Sports Traumatol Arthrosc (2009) 17:705729
1 3
do not appear to be predictive of either knee valgus angles,
neuromuscular patterns or ACL injury risk during dynamic
movement [41, 60, 131]. Likewise, Pantano et al. [148]
demonstrated that peak knee valgus during a single leg
squat, and static knee valgus were not signicantly greater
in young college athletes with higher Q-angle compared to
those with lower Q-angle. Subjects with a larger Q-angle,
however, had a signicantly greater pelvic width to femoral
length ratios compared to subjects with a small Q-angle.
Pelvic width to femoral length ratios was related to both
static and dynamic knee valgus, but static knee valgus was
not related to dynamic knee valgus [148]. The authors
suggested that pelvic width to femoral length ratios, rather
than Q-angle was a better structural predictor of knee
valgus during dynamic movement.
Soderman et al. [170] specically studied the inuence
of the Q-angle in female soccer players of second and third
Swedish divisions. This study was not specically assess-
ing ACL injuries, but the Q-angle was not associated with
an increased risk of leg injuries. Therefore, the exact role of
the Q-angle in the pathomechanics of ACL injuries needs
further investigation. At this point, there is not enough
evidence to suggest an increased Q-angle as a risk factor
for non-contact ACL injuries in soccer players.
Notch width, ACL size and strength
Gender differences have been associated with ACL struc-
tural properties. Chandrashekar et al. [26] found that ACLs
in women were smaller in length, cross-sectional area,
volume, and mass when compared with that of men. The
authors also demonstrated a lower bril concentration and
lower percent area occupied by collagen brils in females
compared to males. In females, ACL stiffness and modulus
of elasticity were highly correlated to bril concentration,
whereas in males ACL failure load and strength were
highly correlated to percent area occupied by collagen [64].
Interestingly, ultra structure of ACL has been related to its
mechanical properties. Women may have lower tensile
linear stiffness with less elongation at failure, and lower
energy absorption and load at failure than men [27, 156].
Unfortunately, cadaveric studies may not be generalizable
due to the high risk of potential bias. The behavior of in
vivo body system is more complex than a cadaveric knee.
These studies may be helpful to elucidate future hypothesis
on this issue, but caution must be taken with the current
conclusions.
A smaller intercondylar notch has been positively corre-
lated to injury risk [165, 180]. Controversy exists when
considering femoral intercondylar notch width as a risk
factor for ACL injury. It has been shown that a smaller notch
size is related to a higher risk of ACL rupture in studies with
high number of participants [99, 172]. In less powerful
investigations, femoral intercondylar notch width was not
related to ACL tears [160, 178]. Despite the lack of rela-
tionship between notch width and ACLsize [127], a recent in
vivo study reported a signicant correlation of the ACL
cross-sectional area to the notch surface area [39]. The
smaller the intercondylar notch the smaller the cross-sec-
tional area of the midsubstance ACL. The explanation for the
increased risk of ACL tear in small notch width subjects is
not fully understood, but it has been suggested that an
impingement of the ACL at the anterior and posterior roof of
the notch may occur during tibial external rotation and
abduction [39, 149]. In addition, sex differences in the
mechanical properties of ACLreported by Hashemi et al. and
Chandrashekar et al. adds more evidence to the small notch-
small ACL-increased risk of ACL rupture relationship.
Posterior tibial slope
Posterior tibial slope is not a clear anatomical risk factor
for ACL injuries. It was rst shown that no relationship
was present between non-contact ACL injuries and the
caudal (posterior) slope of the tibia [118]. However, in a
recent publication, Stijak et al. [174] found that ACL-
injured patients had a signicantly greater tibial slope of
the lateral tibial plateau and a non-signicant lower tibial
slope of the medial tibial plateau compared to the control
group. Both studies were not conducted with soccer players
but with patients. Therefore, further research is needed to
determine whether the posterior tibial slope is a risk factor
for non-contact ACL injuries in soccer players. Studies
assessing posterior tibial slope must control for contralat-
eral tibial slope, intercondylar notch width, knee joint
laxity, lower extremity alignment, neuromuscular, and
biomechanical characteristics.
Foot pronation
Foot pronation and navicular drop have been considered a
risk factor for ACL injuries. Beckett et al. established a
direct relationship between subtalar joint hyperpronation
and ACL tears [8]. The authors compared 50 patients with
past medical history of ACL injury and 50 uninjured sub-
jects. The ACL-injured subjects had greater navicular drop
test scores than uninjured subjects. Later, Woodford-Rogers
et al. compared gymnasts, American Football, and basket-
ball players with history of ACL injury to matched uninjured
athletes. They observed a greater subtalar pronation in the
ACL-injured group [192] results that were also found by
other authors [2]. Also, Loudon et al. compared 20 ACL-
injured females and 20 age-matched controls in a retro-
spective study design. Seven variables were measured:
standing pelvic position, hip position, standing sagittal knee
position, standing frontal knee position, hamstring length,
Knee Surg Sports Traumatol Arthrosc (2009) 17:705729 711
1 3
prone subtalar joint position, and navicular drop test. As
earlier reviewed, knee recurvatum, excessive navicular
drop, and excessive subtalar joint pronation were found to
be signicant discriminators between the ACL-injured and
uninjured groups [107]. Unfortunately, foot pronation and
navicular drop are not free of controversy, since other
authors observed contradictory ndings [86, 169]. In a
recent study conducted by Jenkins et al. [86], 105 soccer and
basketball players (53 women and 52 men) were recruited
and divided into an ACL-normal group and an ACL-injured
group. Two measures of foot structure (subtalar joint neutral
position and navicular drop test values) were recorded for
each subject. No statistically signicant differences were
found in the foot structure measures between women and
men. The authors concluded that values derived from sub-
talar joint neutral position measurement and the navicular
drop test were not associated with ACL injury in collegiate
female and male soccer and basketball players. Addition-
ally, Mitchell et al. [73, 123] recently reported that dynamic
medial foot loading was not related to increased propensity
to demonstrate high ACL-injury risk biomechanics. Subta-
lar joint pronation creates a compensatory increase in the
internal tibial rotation, which has been found to be coupled
with internal tibial rotation at the knee during extension [9,
33]. Normally, subtalar joint pronation and tibial internal
rotation occur only during the contact phase of gait. If
pronation occurs beyond the contact phase, the tibia remains
internally rotated, impeding the occurrence of subtalar joint
supination and tibial external rotation, which normally
occurs as the limb moves through the midstance phase of
gait. This excessive internal tibial rotation transmits
abnormal forces upward in the kinetic chain [8]. Given a
forced movement with planted foot and internal rotation, the
preloaded ACL may be placed to a greater stress that may
evoke to a rupture. Subtalar joint pronation and internal
tibial rotation at the knee may produce an increased internal
femoral rotation and valgus angulation at the knee [153],
enhancing the risk of ACL injury.
Similar to those concerns indicated above related to
posterior tibial slope as a risk factor, studies assessing the
role of foot pronation specically for soccer players are
needed before clear conclusions can be drawn in this
population.
Hormonal risk factors
Overview
While there has been a signicant research focus on sex
hormone relationships to ACL injury, the literature provides
conicting evidence, which has prevented a strong consen-
sus to be reached on whether ACL injury risk is associated
with specic sex hormone uctuations. Almost all studies
assessing the hormonal risk factor for non-contact ACL
injuries involve athletes, although not all of them engaged
soccer players. The study of Martineau et al. [112] found that
oral contraceptive use decreased the ligamentous laxity in
female soccer players. However, there is not enough evi-
dence at this point to widely recommend oral contraceptive
use to prevent non-contact ACL injuries in soccer players.
Pilot evidence indicates that it might be a potential control
strategy in the future if strongest evidence is provided
(Table 1).
Sex hormones
It was shown that human ACL cells had both estrogen and
progesterone receptor sites [105]. Furthermore, it was sug-
gested that gender differences for ACL tears may be, in part,
explained by sex hormones. Specically, hormonal risk
factors are believed to play an important role for non-contact
ACL injuries among female athletes. There are three phases
of the menstrual cycle: follicular (day 09), ovulatory (day
1014) and luteal (day 1528). Disparity of results exists
concerning the time of the menstrual cycle at which the
greatest number of injuries occur: follicular phase [4, 5, 135,
157, 168], around ovulation [1, 14, 187, 188], or the luteal
phase [125]. In a recent systematic review, seven studies
were pooled in an attempt to determine a potential relation-
ship of the menstrual cycle to ACL injury [75]. The seven
reviewed studies favored an effect of the rst half, or pre-
ovulatory phase, of the menstrual cycle for increased ACL
injuries. The six studies that stratied the non-oral contra-
ceptive and oral contraceptive data also favored an effect of
the rst half of the menstrual cycle for increased ACL inju-
ries. The authors concluded that the clinical relevance of this
nding is that female athletes may be more predisposed to
ACLinjuries during the pre-ovulatory phase of the menstrual
cycle, which is consistent with the estrogen surge seen during
this phase of the cycle [75]. Not all hormonal studies com-
pared to a control group nor stratied for oral versus non-oral
contraceptive use. Both aspects are crucial to test the
hypothesis that sex hormones are a potential risk factor for
non-contact ACL injuries.
Effects on laxity
Sex hormones have also been related to an increased
anterior knee laxity. Zazulak et al. [201] conducted a sys-
tematic review on the effects of menstrual cycle on anterior
knee laxity. The authors included nine studies, and they
observed that six of them reported no signicant effect of
the menstrual cycle on anterior knee laxity in women.
However, three studies observed signicant associations
between the menstrual cycle and anterior knee laxity.
712 Knee Surg Sports Traumatol Arthrosc (2009) 17:705729
1 3
These studies all reported an increased knee laxity during
the ovulatory or post-ovulatory phases of the cycle. A
meta-analysis, which included data from the nine reviewed
studies, corroborated the signicant effect of cycle phase
on knee laxity. In the analyses, the knee laxity data mea-
sured at 1014 days was greater than at 1528 days, which
was greater than at 19 days. Hicks-Little et al. [76] also
found that the ovulation and luteal phases of the menstrual
cycle signicantly increased anterior displacement about
the knee. Oral contraceptive use was found to decrease the
ligamentous laxity in female soccer players [112] and to
lower the traumatic injury rate [3, 125, 187]. In another
study, female athletes on oral contraceptives demonstrated
decreased impact forces and reduced medial and lateral
torques at the knee, increased hamstrings to quadriceps
strength ratios, increased stability on one leg and decreased
knee laxity relative to non-users [70]. For this sample, the
use of oral contraceptives appeared to increase the dynamic
stability of the knee joint. These results suggest that
hormonal stabilization increases dynamic stability of the
female athletes knee, and may reduce the risk of serious
knee injury in this high-risk athlete [70]. In contrast, others
have demonstrated a tendency to increase anterior tibial
displacement in oral contraceptive users compared to those
not using hormonal replacement therapy [76].
Effects on ACL tensile strength
Estrogen and progesterone have been found to affect the
collagen metabolism in both animal models and humans.
Essentially, estrogen (i.e., estradiol) decreased broblast
proliferation and type I pro-collagen synthesis whereas
progesterone levels attenuated estrogen inhibitory effect on
collagen metabolism of female ACLs, both in a dose- and
time-dependent manner [197, 198]. Controversy also exists
due to a disparity of results among animal models. Further
research is needed to better elucidate the concentration and
time dependency effects of estrogen exposure, as well as of
other sex hormones, with respect to the ACL tissue [166].
Sex hormones have also been reported to affect tensile
properties of ligaments [18, 92, 193], but other authors
found no signicant differences in maximum force, stiff-
ness, energy to failure, or failure site of ACLs in sheep
[175]. Inuence of sex hormones on mechanical properties
of ligaments has been only studied in animal models.
Further research is also needed to better establish the
inuence of estrogen and other hormones on biomechani-
cal properties of ligaments.
Effects on neuromuscular function
Neuromuscular function seems to also be affected by sex
hormones. During the ovulatory phase, there was an
increase in quadriceps strength, a decrease in muscle
relaxation time, and an increase in muscle fatigability in
young healthy relatively sedentary females [159]. Sex
hormones also decrease motor coordination [152] and have
effects on isokinetic strength, anaerobic and aerobic
capacity, and high-intensity endurance in female athletes
[100]. Interestingly, Chaudhari et al. [31] investigated knee
and hip loading patterns at different phases in the menstrual
cycle. The authors compared performance on horizontal
jump, vertical jump, and drop from a 30-cm box on the left
leg between women (half of them taking oral contracep-
tive) and men. Men were tested once whereas women were
tested twice for each phase of the menstrual cycle (follic-
ular, ovulatory, luteal), and lower limb kinematics (foot
strike knee exion) and peak externally applied moments
were calculated (hip adduction moment, hip internal
rotation moment, knee exion moment, knee abduction
moment). No signicant differences in moments or knee
angle were observed between phases in either female group
or between the two female groups (oral contraceptive users
and non-oral contraceptive users) or between either of
female groups and the male controls. The authors con-
cluded that variations of the menstrual cycle and the use of
an oral contraceptive do not directly effect knee or hip joint
loading during jumping and landing tasks [31]. Because
knee and hip joint loading was unaffected by cyclic vari-
ations in hormone levels, the observed difference in injury
rates was thought to be more likely attributable to persis-
tent differences in strength, neuromuscular coordination,
or ligament properties. As stated, sex hormones as a risk
factor for ACL injury is an attractive and promising area of
research. Nevertheless, there is still equivocal evidence on
many topics, and future research is again needed in this
area to better prevent, at least in part, many ACL injuries.
Neuromuscular risk factors
Overview
Neuromuscular control refers to unconscious activation
of the dynamic restraints surrounding a joint in response
to sensory stimuli [61]. The neuromuscular system gener-
ates movement and determines biomechanics of playing
actions. Unconscious muscle activation is crucial during
many actions in sport, and differences in neuromuscular
control may explain, in part, the increased ACL injury risk
exhibited by a certain cohort of soccer players [141]. Olsen
et al. [141] reported that team handball players were often
judged by the coaches to be out of balance, and in the
majority of cases, some form of perturbation (often contact
with another player) appeared to have altered the players
coordination or intended movement at the time of injury.
Knee Surg Sports Traumatol Arthrosc (2009) 17:705729 713
1 3
Landing, cutting, and pivoting maneuvers in some females
have been shown to differ from males [51, 52, 115].
Essentially, female soccer players perform playing actions
with increased adduction and internal rotation of the femur,
reduced hip and knee exion angles, increased dynamic
knee valgus, increased quadriceps activity (with a con-
comitant decrease in hamstring activity), and decreased
muscle stiffness around the knee joint [69].
Relative strength and recruitment
Dynamic stabilization via the neuromuscular control sys-
tem helps to protect the knee joint during dynamic sport-
related tasks [13, 104, 183185]. However, muscle actions
must be coordinated and co-activated in order to protect the
knee joint [185]. Hence, antagonistagonist relationships
are crucial for joint stability. For the knee joint, co-acti-
vation of hamstrings and quadriceps may be critical to
prevent or to reduce knee motion and loads that increase
the risk of ACL injury. Hamstring recruitment reduces
ACL loads from quadriceps [155, 185], and may help to
provide dynamic knee stability by resisting anterior and
lateral tibial translation and transverse tibial rotations
[104].
In vivo studies where a strain gauge was placed into
an intact ACL at the time of surgery demonstrated that
rehabilitation exercises that produced an isolated con-
traction of the quadriceps muscle near extension strained
the ACL more than exercises with co-contraction of both
quadriceps and hamstrings [48]. Specically, the quad-
riceps muscle cause peak strain to the ACL around 30
of knee exion [10]. Women may have an imbalance
between muscular strength, exibility, and coordination
within their lower extremities [90, 132]. Decits in rel-
ative hamstring strength may contribute to increased risk
of ACL injury in soccer players. Colby et al. [32]
investigated quadriceps and hamstring muscles activation
patterns and determined the knee exion angle during
the eccentric motion of sidestep cutting, cross-cutting,
stopping, and landing in healthy collegiate and recrea-
tional male and female athletes. The results indicated
that there is high-level quadriceps muscle activation
beginning just before foot strike and peaking in
mid-eccentric motion. Hamstring muscle activation was
submaximal at and after initial contact. The maximum
quadriceps muscle activation for all maneuvers was
161% of the maximum voluntary contraction, while
minimum hamstring muscle activity was 14%. Foot
strike occurred at an average of 22 of knee exion
for all maneuvers. This low level of hamstring muscle
activity and low angle of knee exion at foot strike
during eccentric contraction, coupled with relatively
unopposed forces generated by the quadriceps muscles at
the knee, could produce signicant anterior displacement
of the tibia, which may play a role in ACL injury [32].
Chappell et al. [28] found that female soccer, basketball,
and volleyball players prepared for landing with
increased quadriceps activation and decreased hamstring
activation, which may result in increased ACL loading
during the landing of the stop-jump task and the risk for
non-contact ACL injury. Also, Padua et al. [147] found
an increased quadriceps and soleus activation during
hopping as well as a decreased hamstrings to quadriceps
activation ratio in women compared to men (both were
active subjects with previous recreational experience in
soccer, basketball, and volleyball). Hewett et al. dem-
onstrated that a plyometric training reduced the peak
landing forces and increased hamstring torques at landing
in female volleyball players [74]. The decrease in land-
ing forces implies that less force is transmitted to the
knee articulations and passive structures; therefore, more
energy is being absorbed by active muscular restraints.
In contrast, weak hamstrings contribute to a greater
ground reaction forces that place the ACL at a higher
risk of rupture [71]. In addition, adduction and abduction
moments at the knee signicantly decreased after plyo-
metric training and were the sole signicant predictors of
peak landing force. A decreased adduction and abduction
moment would decrease the risk of femoral condylar lift-
off from the tibial plateau [74]. On the other hand, peak
landing exion (reecting net quadriceps muscle activity)
and extension moments (reecting net hamstrings muscle
activity) at the knee did not change after training and
were not signicant predictors of peak landing force.
The plyometric training also increased the hamstring-to-
quadriceps muscle ratio by increasing the hamstring
muscle peak torque. As reviewed, soccer players dem-
onstrated signicantly less anterior and anteriorposterior
knee laxity and higher isokinetic strength of the knee
exors and extensors compared to sedentary controls
[43], what adds more evidence on the dynamic stabilizer
function of muscles. Moreover, Myer et al. [129]
recently found that female soccer and basketball players
sustaining ACL injuries had a combination of similar
quadriceps strength with decreased hamstring strength
compared to males. In direct contrast, female athletes
who did not go on to ACL injury had decreased quad-
riceps strength and similar hamstring strength compared
to matched male athletes. Female soccer and basketball
players who demonstrate increased relative quadriceps
strength and decreased relative hamstring strength may
be at increased risk for ACL injury. Hence, preseason
and continued in-season conditioning focused on ham-
string strengthening may be indicated for female soccer
players, who fall into this high risk unbalanced prole
[129].
714 Knee Surg Sports Traumatol Arthrosc (2009) 17:705729
1 3
Relative joint stiffness and stability
Hamstring muscles are important to decrease anterior shear
forces and greatly reduce load on the primary restraint to
anterior tibial motion, the ACL [7, 126]. It was found that
increasing hamstring muscle force during the knee exion
phase of a simulated jump landing signicantly reduced the
peak relative strain in the ACL in vitro [185]. Through
knee joint compression, hamstrings limit anterior tibial
translation by allowing the concave medial tibial plateau to
limit anterior drawer [82] and by allowing more of the
valgus load to be carried by articular contact forces, pro-
tecting the ligaments [71]. Moreover, hamstring compres-
sion could protect against torsional loading, which has been
found to be greater for females compared to males [104,
189]. In fact, a vigorous quadriceps contraction has been
shown to induce ACL rupture in cadavers [38]. Women
demonstrate decreased hamstrings-to-quadriceps peak tor-
que ratios and increased knee abduction (valgus) moments
compared to males [71]. Hamstring muscles are activated
by ACL receptors when the ligament is placed under stress,
what adds more evidence to the hamstrings provide
agonistic support to the ACL. It was also suggested that
hamstrings are activated by an alternative reex arc
unrelated to ACL receptors [171]. This ACL receptor-
dependent muscle activation suggests that decreased pro-
prioception could have an impact on knee stability. The
hamstring activation depending on the ability of the ACL
to sense a torque and elongation may justify the inclusion
of proprioception training in preventive and rehabilitation
programs [171].
Muscles crossing a joint provide stability to that joint. In
other words, muscle stiffness, or the resistance to dynamic
stretch may protect ligaments from rupture when a load is
applied. As reviewed, quadriceps and hamstring muscles
provide anteriorposterior joint stiffness. Others suggest
that sagittal plane knee joint stiffness is also relevant for
ACL injury prevention. Studies demonstrate that female
athletes show less muscular stiffness than their male
counterparts [58, 59, 67, 79, 88, 161, 186, 189]. Males
activate their lower extremity muscles signicantly earlier
[67], and have longer activation duration in muscles that
initiated and maintained knee (gastrocnemius) and lower
extremity stiffness (gluteus) than women [88]. Decreased
muscular stiffness in females was shown for both anterior
tibial translation [58, 59, 81, 88, 186] and rotational forces
[58, 59, 161, 189]. In a recent study, Schmitz et al. [161]
investigated the varus/valgus and internal/external tor-
sional knee joint stiffness in both males and females. Knee
kinematics of 20 university students were measured while
applying 010 Nm of varus and valgus torques with the
subject non-weight-bearing, and 05 Nm of internal and
external torques in both non-weight-bearing and weight-
bearing conditions, with the use of a custom joint testing
device. When low magnitudes of torque were applied to the
knee, women had signicantly lower stiffness values than
did men. With the exception of applied external torque
with the joint weight-bearing and varus torque with the
joint non-weight-bearing, women demonstrated an increase
in joint stiffness as the magnitude of torque increased from
lower to higher magnitudes. In contrast, for the men, joint
stiffness values remained unchanged as the magnitude of
applied torque increased. The authors concluded that
women exhibited lower knee stiffness in response to low
magnitudes of applied torque compared to men and dem-
onstrated an increase of joint stiffness as the magnitude of
applied torque increased [161].
Muscular fatigue
Since muscles contribute to joint stability, muscular fatigue
might be a risk factor for ligament injuries. Fatigued
muscles are able to absorb less energy before reaching the
degree of stretch that causes injuries [108]. Better condi-
tioned soccer players may have improved neuromuscular
control later in games relative to de-conditioned athletes.
This improved neuromuscular control may help athlete to
better absorb energy, leaving less energy to be absorbed by
other structures such as ligaments [158]. Under fatigued
conditions, it was shown that males and females decrease
knee exion angle and increase proximal tibial anterior
shear force and knee varus moments when performing
stop-jump tasks [29]. Nyland et al. [140] investigated the
effect of quadriceps and hamstrings fatigue from eccentric
work on the activation onset of vastus medialis, rectus
femoris, vastus lateralis, the medial hamstrings, biceps
femoris, and gastrocnemius muscles in healthy female
athletes compared with controls directly after performing
crossover cut training. The authors demonstrated that
quadriceps fatigue from eccentric work produced earlier
gastrocnemius and delayed quadriceps femoris activation
during crossover cutting in female athlete compared to
controls, but activation onset did not differ compared to
hamstring fatigue. Neither hamstring nor quadriceps
femoris fatigue produced differences in medial hamstring
or biceps femoris activation onset compared to controls.
The authors concluded that the gastrocnemius muscles act
as a synergistic and compensatory dynamic knee stabilizer
in a closed kinetic chain situations as the quadriceps
femoris muscles fatigue [140]. Conversely, Fleming et al.
[49] demonstrated that the gastrocnemius muscle is an
antagonist of the ACL. Six subjects with normal ACLs
participated in the study. Subjects underwent spinal anes-
thesia to ensure that their leg musculature was relaxed.
Transcutaneous electrical muscle stimulation was used to
induce contractions of the gastrocnemius, quadriceps and
Knee Surg Sports Traumatol Arthrosc (2009) 17:705729 715
1 3
hamstrings muscles, while the strains in the anteromedial
bundle of the ACL were measured using a differential
variable reluctance transducer. The ACL strain values
produced by contraction of the gastrocnemius muscle were
dependent on the magnitude of the ankle torque and knee
exion angle. Co-contraction of the gastrocnemius and
quadriceps muscles produced ACL strain values that were
greater than those produced by isolated activation of either
muscle group when the knee was at 15 and 30. Co-con-
traction of the gastrocnemius and hamstrings muscles
produced strains that were higher than those produced by
the isolated contraction of the hamstrings muscles. At 15
and 30 of knee exion, the co-contraction strain values
were less than those produced by stimulation of the gas-
trocnemius muscle alone [49]. Landry et al. [97, 98]
demonstrated that elite female soccer players exhibit an
increased gastrocnemius activity during unanticipated run,
side-cut, and cross-cut maneuvers. Female soccer players
demonstrated a higher gastrocnemius activity and a medi-
olateral gastrocnemius activation imbalance during early
stance to midstance of the side-cut and during both run and
cross-cut maneuvers that was not present in the male
players. Additionally, for unanticipated side-cut maneu-
vers, female athletes demonstrated greater rectus femoris
muscle activity throughout stance, and the only hamstring
difference identied was a mediolateral activation imbal-
ance in male athletes only [98]. Moreover, for unantici-
pated run and cross-cut maneuvers, rectus femoris activity
and vastus medialis and lateralis activity for the straight run
only were also greater in female than in male athletes [97].
Other notable difference captured for both maneuvers
included female players having reduced hamstring activity
compared to male players. Padua et al. [147] also observed
greater soleus activation during hopping in healthy women
compared to men.
Nyland et al. [139] further investigated the effects of
hamstring fatigue on transverse plane knee control during
a running crossover cut directional change (functional
pivot shift). The authors found that an eccentric work-
induced hamstring fatigue created decreased dynamic
transverse plane knee control as evidenced by increased
knee internal rotation during impact-force absorption, an
earlier peak ankle plantar-exor moment onset, and a
decreased knee internal rotation with propulsion during
hamstring fatigue. It was suggested that this pattern may
represent compensatory attempts at dynamic knee stabil-
ization from the posterior lower leg musculature during
the reportedly ligamentous stressful functional pivot shift
phase of the crossover cut [139]. In turn, other authors
found an increased anterior tibial translation with mus-
cular fatigue in healthy knees [119, 190]. However,
Wojtys et al. [190] found that the recruitment order of the
lower extremity muscles in response to anterior tibial
translation did not change with fatigue. Melnyk and
Gollhofer [119] assessed reex latencies and neuromus-
cular hamstring activity using surface electromyography.
Muscle fatigue produced a signicant longer latency for
the monosynaptic reex latencies, whereas no differences
in the latencies of the medium latency component were
found. Fatigue signicantly reduced EMG amplitudes of
the short and medium latency components. The authors
suggested that a reduced motor activity rather than the
extended latency of the rst hamstring response is the
reason for possible failure. McLean et al. [113] also
investigated the impact of fatigue on ACL injury risk. Ten
males and ten females were compared performing a land
from a jump. Females landed with more initial ankle
plantar exion and peak-stance ankle supination, knee
abduction, and knee internal rotation compared with men.
They also had larger knee adduction, abduction, and
internal rotation, and smaller ankle dorsiexion moments.
Fatigue increased initial and peak knee abduction and
internal rotation motions and peak knee internal rotation,
adduction, and abduction moments, with the latter being
more pronounced in females. Therefore, McLean et al.
concluded that fatigue-induced modications in lower-
limb control may increase the risk of non-contact ACL
injury during landings. Gender dimorphic abduction
loading in the presence of fatigue also may explain the
increased injury risk in women [113].
Decision-making (i.e., anticipated and unanticipated
actions), in addition to fatigue, has been shown in isola-
tion to directly impact ACL injury risk [11, 78, 151]. For
example, Besier et al. [11] examined a sidestep cut at two
different angles under both anticipated and unanticipated
conditions and found increased varusvalgus and internal
external knee moments during unanticipated movements.
The authors suggested that the increased coronal plane
torques increased the potential for ACL injuries during
unanticipated movements. Lower extremity muscle acti-
vation during cutting is signicantly different between
anticipated and unanticipated conditions [11]. Recently,
the effects of a combination of fatigue and decision-
making on landing postures were investigated. Borotikar
et al. [19] studied the combined effects of fatigue and
decision-making on lower limb kinematics during sports
relevant landings. Fatigue caused signicant increases in
initial contact hip extension and internal rotation, and in
peak stance knee abduction and internal rotation and
ankle supination angles. Fatigue-induced increases in
initial contact hip rotations and in peak knee abduction
angle were also signicantly more pronounced during
unanticipated compared to anticipated landings. It was
suggested that the integrative effects of fatigue and
decision-making may represent a worst case scenario in
terms of ACL injury risk during dynamic single leg
716 Knee Surg Sports Traumatol Arthrosc (2009) 17:705729
1 3
landings, by perpetuating substantial degradation and
overload of central control mechanisms [19]. Addition-
ally, Olsen et al. [141] reported that ACL injuries
occurred when team handball players were out of balance,
or some form of perturbation (often contact with another
player) altered the players coordination. Laboratory
studies do not correlate with eld studies at all. Fauno
and Wulff Jakobsen [45] reported that ACL injuries in
second half is not statistically different from rst half, so
fatigue was not seen as a risk factor by the authors. Thus,
it appears that fatigue may contribute to other risk factors,
but may not in itself be an isolated risk factor for ACL
injury.
Biomechanical risk factors
Overview
Biomechanics of playing actions are necessary to under-
stand the pathomechanics of ACL injuries and to offer
effective prevention programs. It was postulated that hip
low forward exion, hip adduction, hip internal rotation,
knee valgus, knee extension, and knee external rotation
may place the ACL to a high risk of rupture. It was called
the position of no return [84]. Biomechanical studies
have been conducted in cadavers, in vivo through strain
gauges placed at the time of surgery, and from analytical
modeling. Biomechanical risk factors for ACL injuries
have been described in all three planes. Abundant data
exists considering biomechanical risk factors in athletes.
Specic biomechanical studies involving soccer players do
also exist, especially in females.
Sagittal plane
Sagittal plane biomechanics have yielded many studies on
trunk, hip, knee, and ankle exion angles when performing
sport tasks. The more joints are exed during landing, the
more the energy is absorbed and the less the impact is
transferred to the knee. Also, the ACL and hamstring
anatomy explain why knee exion is protective of ACL
damage. Every movement with inuences over knee ex-
ion can contribute to ACL injury. From proximal to distal,
Blackburn and Padua [16] demonstrated that increased
trunk exion during landing also increased hip and knee
exion angles. The authors found that trunk exion altered
neither transverse nor frontal plane kinematics during the
landing task. A less erected posture during landing has
been associated with a reduced ACL injury risk [61, 68,
89].
Hewett et al. [73] reported a signicant increased peak
external hip exion moment in ACL injured compared to
uninjured females soccer, basketball, and volleyball play-
ers, but was not observed to be a signicant predictor of
ACL injury. These data suggest ACL-injured athletes had
an increased internal hip extensor moment due to an
increased gluteus maximus activity. Conversely, Decker
et al. [35] suggested that a decreased hip musculature
activity may produce a higher ground reaction force,
because muscles would be used to absorb energy from a
certain task. Landry et al. [97, 98] studies showed that elite
female soccer players exhibited a reduced external hip
exion moment and hip exion angle during unanticipated
side-cut, run, and cross-cut maneuvers. Similarly, Zazulak
et al. [202] found a decreased gluteus maximus activity in
females during single-legged landings.
Female soccer players demonstrate decreased hip and
knee exion angles at landing compared to male soccer
players after the age of 13-year-old [196]. Young female
soccer, basketball, and volleyball players also showed
decreased hip and knee exion angles compared to males
during the landing preparation of a vertical stop-jump task
[28]. Resultant initial contact lower extremity motion pat-
terns during landing of the stop-jump task may be pre-
programed just prior to landing. Therefore, female subjects
prepared for landing with a decreased hip and knee exion
angle which may result in increased ACL loading during
the landing of the stop-jump task and the risk for non-
contact ACL injury [28]. It was postulated that a decreased
hip and knee exion angles at landing places the ACL at a
greater risk of injury, because a greater peak landing force
is transmitted to the knee [74]. Yu et al. [195] showed that
hip and knee exionextension angular velocity, rather
than angle or joint position, was correlated to the peak
posterior and vertical ground reaction forces at landing
from a stop-jump task. On average, females landed with
greater impact forces and had smaller hip and knee exion
angles at the initial foot contact with the ground and
maximum knee exion angle at the end of the landing. The
greater the hip and knee exion angular velocity at the
initial foot contact during the landing of a stop-jump task,
the lesser the posterior and vertical ground reaction forces.
Also, the greater the peak proximal tibia anterior shear
force and peak knee extension moment during landing, the
greater the posterior and vertical ground reaction force.
Therefore, decreased hip and knee exion angles at landing
as a risk factor for ACL injury may not be resultant from
increased ground reaction force [195]. Instead, the
increased risk of ACL injury from decreased knee exion
angle could be explained by differences in ACL elevation
angle, the angle of insertion of the hamstrings, and by
differences in patellar tendontibial shaft angle. Near knee
extension, the ACL has a greater elevation angles, so the
ligament is more perpendicular to a tibial plateau line,
whereas the ACL is essentially parallel to the tibial plateau
Knee Surg Sports Traumatol Arthrosc (2009) 17:705729 717
1 3
with knee exion past 90 [103]. This change in orientation
inuences the load placed on the ACL and its ability to
sustain elastic deformation without injury [16]. The struc-
tural properties of the ACL are maximized under tensile
(longitudinal) loading conditions and minimized under
non-axial (shear) loading conditions [191]. As the knee
progresses into extension, the ACL elevation angle is
maximized. Under this conguration, the anterior tibial
shear force generated by the quadriceps/patellar tendon and
imparted to ACL is increasingly shear in nature. Con-
versely, as the ACL elevation angle decreases with knee
exion, the shear component of the resultant ACL force
decreases while the tensile component increases recipro-
cally [16]. Additionally, as the knee progresses into exion,
the angle of insertion of the hamstrings with respect to the
tibial longitudinal axis increases such that at knee exion
angles greater than 100, the resultant hamstring force is
directed parallel to the tibial plateau [16, 204]. On the other
hand, at lower degrees of knee exion, the angle of
insertion of the hamstrings with respect to the tibial lon-
gitudinal axis decreases such that the resultant hamstring
force is directed parallel to the ACL, which is placed
perpendicular to the tibial plateau, thus limiting the ham-
strings potential to counteract anterior tibial strain to the
ACL. Also, an extended lower limb at landing may strain
the ACL due to a greater patellar tendontibial shaft angle
that increases the anteriorly directed component of the
force produced by the quadriceps muscle [194]. As the
knee progresses into exion, the patellar tendon insertion
angle with respect to the tibial longitudinal axis decreases
[204]. This change in patellar tendon orientation has a
profound inuence on tibial shear force, as the anteriorly
directed component of the quadricepspatellar tendon force
is derived as a multiple of the sine of the insertion angle
[16]. Hence, at lower knee exion angles, the quadriceps
exerts a higher anteriorly directed force that is poorly
counteracted by both the ACL and the hamstrings. Addi-
tionally, the maximum quadriceps force is estimated to be
produced around 60 of knee exion [203]. Therefore, it
might be argued that an extended position around 20 of
knee exion may produce less impact absorption through
the musculotendinous system increasing the force trans-
mitted to the passive structures of the knee. A large hip and
knee exion angles at the initial foot contact with the
ground do not necessarily reduce the impact force during
landing, but active hip and knee exion motions do [195].
It was also demonstrated that females had increased
quadriceps activation before landing from the same task
compared with male subjects [195]. Yu et al. also found
that female athletes exhibited an increased hamstring
activation before landing but a trend of decreased ham-
string activation after landing compared with male sub-
jects, whereas Krosshaug et al. [94] showed an increased
knee exion angle both at initial contact and 50 ms after
initial ground contact in female basketball players com-
pared to males. Landing preparation with increased quad-
riceps activation may increase ACL loading during
landing, since muscle activation is a major determinant of
muscle contraction force [87]. A greater quadriceps acti-
vation [109] and increased knee extension moment [30]
during landing of a variety of athletic tasks in female
athletes compared to their male counterparts was also
observed by other authors. Hewett et al. [73] found similar
knee exion angles at initial contact between ACL injured
and uninjured female athletes in a prospective study. The
peak knee exion moment was also similar; however,
maximum knee exion angle was lower in the ACL-injured
group compared to uninjured controls. Several authors
report that isolated sagittal plane forces are not high
enough to tear the ACL during sports [114, 150]. In
addition, there is no consensus on whether females land or
cut with less [80, 109], same [52, 114, 116], or greater [44,
94] knee exion angles compared to males.
Ankle joint is a key component in any movement in
closed kinetic chain. Therefore, ankle sagittal plane
movements have also an involvement in the knee joint. Self
and Paine [163] showed that landing technique with the
largest ankle plantar-exion position at ground contact
demonstrated the most shock absorption and reduction of
the peak vertical ground reaction force. It was recently
demonstrated that landing with the rear foot (dorsiexed
ankle) was associated with less hip and knee exion at peak
vertical ground reaction force than forefoot landing (plan-
tarexed ankle) [34]. Also, the maximum knee exion
angle with forefoot landing technique was signicantly
higher than the rear foot technique. In contrast, hip and
knee exion angles at initial foot contact were signicantly
lower with the forefoot than rear foot technique. Given that
the maximum force transferred to the knee would be at the
peak vertical ground reaction force, a forefoot landing
might be preferred over rear foot technique. No signicant
differences for foot-landing technique were observed
between males and females [34]. However, Burkhart et al.
[25] reported in a prospective research study that an athlete
who landed with an increased heel to at-foot loading
mechanism was more likely to sustain to a non-contact
ACL injury during competitive play.
Coronal plane
Coronal plane biomechanics are also involved in the gen-
esis of non-contact ACL injuries. Houck et al. [78] inves-
tigated coronal plane trunk/hip kinematics and hip and
knee moments (measures of neuromuscular control) during
unanticipated compared to anticipated straight and side
step cut tasks. Hip angles, but not lateral trunk exion,
718 Knee Surg Sports Traumatol Arthrosc (2009) 17:705729
1 3
were altered during unanticipated conditions. Lateral trunk
exion remained near 810 for both anticipated and
unanticipated tasks, what was explained by a compensatory
decrease in the left lateral tilt orientation of the pelvis
(taken at the same instant in stance as lateral trunk orien-
tation) during the sidestep unanticipated task by 23
compared to both the anticipated and unanticipated straight
step task, and anticipated sidestep task. Lateral trunk ori-
entation was not a result of lateral trunk exion, suggesting
even during unanticipated tasks the pelvis and thorax
rotated as a single segment. The authors interpreted that hip
abduction angles and foot placement, not lateral trunk
exion inuence trunk orientation [78]. Zazulak et al. [199]
investigated the effects of isolated trunk displacement after
a perturbation in a laboratory study as a predictor of knee
ligament injury. Twenty-ve athletes (11 female and 14
male) sustained knee injuries over a 3-year period. Trunk
displacement in any plane was greater in athletes with
knee, ligament, and ACL injuries than in uninjured ath-
letes. Lateral displacement was the strongest predictor of
ligament injury. Trunk displacements, proprioception, and
history of low back pain predicted knee ligament injury
with 91% sensitivity and 68% specicity. This model
predicted knee, ligament, and ACL injury risk in female
athletes with 84, 89, and 91% accuracy, but only history of
low back pain was a signicant predictor of knee ligament
injury risk in male athletes [199]. Therefore, core stability
may be an important component of ACL injury prevention
programs.
Hip angles during landing can be important determi-
nants of impact force at the knee [71]. Female soccer,
basketball, and volleyball players may have an increased
external adduction moment about the hip at landing.
Increased adduction moment about the hip may place an
increased valgus stress over the knee [51, 73], but the hip
adduction itself was not demonstrated to be a risk factor
for ACL injury [73]. Hip abduction angles and knee
moments were signicantly affected by the type of task
and anticipation. Hip abduction angles decreased by 4.0
7.68, when comparing the unanticipated sidestep task to
the anticipated straight step, unanticipated straight step,
and anticipated sidestep tasks [78]. The hip abduction
angles were associated with foot placement and lateral
trunk orientation. The unanticipated sidestep task reduced
the distance between contact point and the trunk center of
mass, probably to perform faster, inuencing the whole
kinetic chain proximally. During landing preparation of a
stop-jump task, young female soccer, basketball, and
volleyball players demonstrated a decreased hip abduction
compared to their male counterparts [28]. Jacobs et al.
[85] observed that healthy women had lower hip abductor
peak torque than healthy men. Hip abduction peak torque
correlated moderately with hip exion peak joint
displacement in women, and most importantly hip exion
and adduction peak joint displacement increased after a
30-s bout of isometric hip abduction exercise. It was also
observed that squat strength positively correlated with hip
abduction strength in female soccer players but not for
men [181]. The authors suggested hip abduction strength
assessment as a potential method to identify those sub-
jects at risk of ACL injury at landing. Imwalle et al. [83]
evaluated lower extremity motions in females performing
unanticipated cutting task that directed their running
angles to 45 and 90. They reported that hip internal
rotation and knee internal rotation were increased during
the 90 cut compared to the 45 unanticipated cut
angle. Mean hip exion was also greater in the 90 cut.
However, the only signicant predictor of knee abduction
during both tasks was hip adduction. The authors
suggested that ndings indicate that the mechanisms
underlying increased knee abduction measures in female
athletes during cutting tasks were primarily coronal plane
motions at the hip [83].
Coronal plane knee biomechanics are also related to
ACL injury. Hewett et al. [73] conducted a prospective
study where 205 female athletes participating in the high-
risk sports of soccer, basketball, and volleyball were
measured for neuromuscular control using three-dimen-
sional kinematics (joint angles) and joint loads using
kinetics (joint moments) during a jump-landing task. Nine
athletes had a conrmed ACL injury. Knee abduction
angle at landing was 8 signicantly greater in ACL-
injured athletes compared to uninjured athletes. In addi-
tion, ACL-injured subjects had 2.5 times greater knee
abduction moment and 20% higher ground reaction force
compared to uninjured subjects. Also, women have
exhibited greater valgus moments than men during the
landing phase of each stop-jump task [30]. Additionally,
increased motion, force, and moments occurred more
quickly in the injured compared to uninjured athletes [73].
For cutting maneuvers, Ford et al. [52] demonstrated that
females exhibited greater knee abduction (valgus) angles
compared with males.
There is a scarcity of studies on coronal plane ankle
biomechanics, but the very few studies demonstrate similar
results. Ford et al. [52] demonstrated that female basketball
players had greater maximum ankle eversion than did male
athletes during the stance phase of cutting. Similarly,
Landry et al. [97] found an increased ankle eversion angle
throughout stance in elite female soccer players compared
with male players for unanticipated run and cross-cut
maneuvers. It was already reviewed that ankle kinematics
inuence knee joint. Excessive ankle eversion may
increase internal tibial rotation, knee valgus stress, anterior
tibial translation, and loading on the ACL during extension
[9, 33, 71, 153].
Knee Surg Sports Traumatol Arthrosc (2009) 17:705729 719
1 3
Transverse plan
Transverse plane biomechanics have been focused on hip
and knee joints. Hip biomechanical ndings mainly refer to
a greater hip internal rotation maximum angular displace-
ment [102] and a lower gluteal EMG activity [202] at
landing in female soccer, basketball, and volleyball players
compared to males. When performing unanticipated side-
cut maneuvers, female soccer players exhibited more hip
external rotation compared with the male athletes [98].
When performing unanticipated cutting tasks at 90 unan-
ticipated cut angles, females increased hip internal rotation
and knee internal rotation relative to the 45 unanticipated
cut angle. However, the changes in transverse planes
motion were not related to concomitant coronal plane
motions at the knee [83].
Transverse plane knee biomechanics depend on the type
of task and decision-making. Besier et al. [12] showed
that varus/valgus and internal/external rotation moments
applied to the knee during sidestepping and crossover
cutting were considerably larger than those measured
during normal running. The same group found that cutting
maneuvers performed without adequate planning may
increase the risk of non-contact knee ligament injury due to
an increased internalexternal rotation moments applied to
the knee [11]. The authors attributed these results to the
small amount of time to make appropriate postural
adjustments before performance of the task such as the
position of the foot on the ground relative to the body
center of mass [11]. Landing preparation from a stop-jump
task demonstrated that young female soccer, basketball,
and volleyball players had a decreased hip external rotation
and increased knee internal rotation compared with male
athletes [28]. It has been also shown that healthy women
had higher knee laxity, lower stiffness, and higher energy
loss in passive external tibial rotation than did healthy men
[149].
Discussion
The present literature review elicited several conclusions.
First, common playing situations precluding a non-contact
ACL injury include change of direction or cutting
maneuvers combined with deceleration, landing from a
jump in or near full extension, and pivoting with knee near
full extension and a planted foot. Second, the most
common non-contact ACL injury mechanism includes a
deceleration task with high knee internal extension torque
(with or without perturbation) combined with dynamic
valgus rotation with the body weight shifted over the
injured leg and the plantar surface of the foot xed at on
the playing surface. Third, potential extrinsic non-contact
ACL injury risk factors include: dry weather and surface
and articial surface instead of natural grass. Finally,
commonly purported intrinsic risk factors include: gen-
eralized and specic knee joint laxity, small and narrow
intercondylar notch width (ratio of notch width to the
diameter and cross sectional area of the ACL), pre-ovula-
tory phase of menstrual cycle in females not using oral
contraceptive, decreased relative (to quadriceps) hamstring
strength and recruitment, muscular fatigue by altering
neuromuscular control, decreased core strength and
proprioception, low trunk, hip, and knee exion angles, and
high dorsiexion of the ankle when performing sport tasks,
lateral trunk displacement and hip adduction combined
with increased knee abduction moments (dynamic knee
valgus), and increased hip internal rotation and tibial
external rotation with or without foot pronation. Non-
contact ACL injury in female athletes likely has a multi-
factorial etiology. Prior epidemiological data demonstrate
that neuromuscular and biomechanical risk factors may
contribute in isolation or combination with other factors,
such as anatomical, hormonal and potentially psychologi-
cal parameters, to increase relative non-contact ACL injury
rates in female athletes.
In general, more research is needed to better elucidate
the exact role of all reviewed risk factors in both female
and male soccer players. Upon an extensive literature
review, nearly every risk factor has contradictory data
reported at some point, although there is a preponderance
of supportive evidence that acquiesces many of them. The
reason why some authors found conicting results may be
explained by the lack of adequate control on multiple
confounding factors, especially when the research study
may have been insufciently powered. Whenever possible,
studies with an emphasis on designing and reporting Level
I research for prospective randomized controlled trials are
needed. There is an existing need for further research
investigating the role of non-contact ACL injury in male
soccer players. The fact that females are at greater risk for
an ACL tear should not imply that no research should be
conducted on male soccer players. The economic conse-
quences of ACL injuries in semi-professional and pro-
fessional male soccer players are enormous, and the
psychological impairment to the injured player is difcult
to quantify but easily understood. Elite soccer studies are
limited and it is important to explore this eld, since pro-
fessional soccer players are a relatively homogeneous
sample that may differ in some characteristics from rec-
reational players.
Mechanisms of ACL injury have been mostly described
in cadaveric studies. Video tape analysis has been used to
report mechanisms of injury, but the accuracy and preci-
sion is questionable, especially when dealing with rota-
tional and coronal plane moments. In contrast, video
720 Knee Surg Sports Traumatol Arthrosc (2009) 17:705729
1 3
analysis allows a forum to obtain on the eld data collec-
tion. Continuous efforts should be made to improve the
accuracy of on-eld analysis. Soccer regulations tend to
impede the investigation of game injuries, but practice or
training sessions can be easily assessed for epidemiological
data. ACL tears could be better understood if adequate
technology is provided and available on the eld.
Environmental risk factors need to be specically
assessed in soccer, since most studies deal with American
or Australian Football. A comprehensive prospective epi-
demiological study on non-contact ACL injury incidence
incurred during the sport of soccer with respect to playing
surface (gravel, articial turf, and natural grass), soccer
division, and intensity of play at the time of injury (practice
versus games) controlling for level of conditioning,
weather conditions, or soccer boots would be desirable.
Well-designed laboratory and eld-based studies are nee-
ded in order to adequately assess cleat selection in soccer
players. From a theoretical point of view, orthotics may be
potentially useful to increase impact absorption or to cor-
rect malalignments. However, more research should be
conducted in this eld. It is important to point out that
research on shoes and shoesurface interaction may pro-
vide elucidating results, and provides a means of relative
ease with regard to an intervention. Studies regarding
weather conditions need to control for many other potential
confounding factors like intrinsic biomechanical factors,
neuromuscular conditioning, or hydration status of soccer
players, among others. The effects of prophylactic knee
braces use on neuromuscular control, knee and whole-body
kinematics, and knee kinetics of soccer players need to be
better characterized. It is not only important to observe the
general inuence of knee braces at ACL injury reduction,
but also to clarify the mechanisms by which they affect
injury rates. Knee braces studies should be placebo-con-
trolled to limit the inuence of psychological factors. Knee
brace interventions need to control for many parameters
(position of the player, level of conditioning, skills, expe-
rience of the player, soccer division, etc) and also need to
include highly homogeneous and a large human sample.
Prevention of non-contact ACL injuries through modi-
cation of anatomical risk factors may seem to have
limited potential for intervention. However, more investi-
gation in this area will provide us with a better under-
standing of this injury, and may provide insights on
techniques to at least control for these risk factors to help
diminish their potential to increase risk of injury (Table 1).
Generalized joint laxity or specic knee joint laxity studies
need to control for neuromuscular factors. Moreover, spe-
cic investigations on mechanical properties of the ACL in
loose jointed individuals compared to stiff subjects are
desirable. It is necessary to clarify biomechanical conse-
quences of anterior pelvic tilt in lower extremity
biomechanics, especially in relation to those modications
that may place the ACL at a greater risk of rupture. Sim-
ilarly, the increased Q-angle as a risk factor for non-contact
ACL tears, considered both statically and dynamically,
need clarication, since its role in ACL injuries seems
more theoretical than practical. Also, it is required that
studies on intercondylar notch width are controlled for
ACL size. It might be argued that a narrower intercondylar
notch size allows less growth to the ACL during human
development. Theoretically, a smaller ACL may be at
greater risk of rupture, but studies on notch width need to
be also controlled by anthropometric characteristics,
because a small ACL may not be at greater risk of rupture
if the subject is short and thin. The relationship of notch
width, ACL size, and anthropometrics of soccer players
need to be collectively studied. Other bone morphology
characteristics such as posterior tibial slope also require to
control for other anatomical, hormonal, neuromuscular,
and biomechanical risk factors.
It was postulated that a familial tendency to non-contact
ACL injuries may exist, but the existing literature is sparse.
Well-controlled large-sampled studies are needed to
observe the incidence of non-contact ACL injuries within
immediate family members of players who sustained uni-
lateral or bilateral non-contact ACL injuries compared to
their uninjured team mates. In the same way, genetic
investigations may bring us to a new dimension for the
understanding of non-contact ACL injuries. For example,
broblast gene expression at the ACL may differ among
injured versus uninjured subjects. These differences may
alter ultra structural characteristics of ligaments and place
them at a greater risk of rupture. Could eco-guided ne-
needle aspiration biopsy of the ACL provide information
on specic genes? Could gene studies predict soccer
players at greater risk of suffering non-contact ACL inju-
ries? Further ultra structural composition of the ACL
comparisons between female and male soccer players are
needed, and between ACL injured and uninjured males as
well.
Hormonal risk factors are a promising area of research
given the enormous amount of unanswered questions at this
point in time. More research is needed to better establish
the effects of sex hormones on structure, metabolism, and
mechanical properties of tendons and ligaments. The
required minimum hormonal concentrations to evoke these
tendinous and ligamentous effects should be better dened.
Also, the interaction between different hormones would be
a more realistic approach to this issue (i.e., estrogen, pro-
gesterone, testosterone, relaxin, and inhibin). It is crucial to
characterize the phase of the menstrual cycle where female
soccer players are at increased risk of non-contact ACL
injuries, if one does indeed exist. In the eld hormonal
studies should consider the interaction of the level of
Knee Surg Sports Traumatol Arthrosc (2009) 17:705729 721
1 3
training, level of competition, stress factors, nutritional
status, sex hormones, and phase of menstrual cycle in
female soccer players.
Neuromuscular and biomechanical risk factors are in
direct relation to anatomical structure and development. In
fact, it would be interesting to assess if pre-pubertal or
pubertal soccer players could benet from the great
potential at modifying neuromuscular risk factors during
these developmental stages. Landing neuromuscular and
biomechanical studies should aim to investigate authentic
game and practice situations such as landing after heading
the ball rather than landing from a box. Foot-landing
techniques should also be assessed under real jump-landing
tasks. Also, neuromuscular and biomechanical studies of
unanticipated tasks should be conducted under opposing
playing situations rather than using cones and verbal
orders. In general, neuromuscular and biomechanical
studies require large samples, especially if conducted
prospectively, given that a low number of ACL injuries
may underpower the study. A new window to future
research was opened by Hewett et al. [73] when they
prospectively demonstrated that knee motion and knee
loading during a landing task were predictors of ACL
injury risk in female soccer, basketball, and volleyball
players. Hence, neuromuscular and biomechanical assess-
ments should be studied as potential screening tools. It is
also essential to further study the relationship between
external knee joint loads and the whole-body kinematics.
As reviewed, each segment in the body is related to each
other. Thus, a holistic view would consider that the load
experienced at the knee joint may be related to the position
of the foot on the ground with respect to the bodys center
of gravity or the angle of the lower limb with respect to the
ground [12]. Neuromuscular and biomechanical studies
should take into account postural adjustments in all parts of
the body, not only in hip, knee, and ankle joints but also in
pelvis and trunk. Likewise, ankle transverse, sagittal, and
coronal plane biomechanics in relation to ACL injury risk
are a wide and relatively unexplored area to investigate.
Another area to further investigate would be to better
characterize the relationship between peak ground reaction
force and the ACL loading. It is also important to further
investigate the role of the iliopsoas muscle in different
soccer tasks (since it is directly related to both trunk and
hip biomechanics), the role of hip abductors on the landing
biomechanics in relation to ACL risk of injury, the role of
rectus femoris and his relationship to the location of the
center of gravity (especially when the center of gravity falls
behind the knee at landing and the rectus femoris has to act
as a trunk exor, requiring a high force that would be
potentially transmitted to the knee), and the role of the
gastrocnemius muscles during dynamic soccer tasks.
Muscular imbalance, especially between hamstrings and
quadriceps, should be further investigated to better know
how they inuence on non-contact ACL injuries. The exact
role of neuromuscular fatigue remains controversial. Many
laboratory studies show that fatigue may alter neuromus-
cular control and may place the athlete at a greater risk of
ACL injury, but there is no clear increase in non-contact
ACL tears at the end of the game or season.
Conclusions
Non-contact ACL injury in athletes likely has a multi-
factorial etiology, with several potential elements which
determine injury mechanism. There does not appear to be
an isolated risk factor presenting in all cases of non-contact
ACL injuries. Instead, a combination of risk factors may
better predict those soccer players at increased risk of
injury. When comparing the data extracted from the
reviewed studies, one might generate a few conclusions
regarding ACL injury mechanisms and the associated risk
factors in soccer players.
Conclusions on non-contact ACL injury mechanisms in
soccer players:
Most ACL injuries in soccer players are non-contact in
nature (Fig. 1).
Change of direction or cutting maneuvers combined
with deceleration, landing from a jump in or near full
extension and pivoting with knee near full extension
and a planted foot are among the most common playing
situations precluding an ACL injury. These playing
situations involve knee valgus, varus, internal rotation,
and external rotation moments, and anterior translation
force.
An anterior translation force may be the most detri-
mental direct isolated force associated with non-contact
ACL injuries. However, a combination (sagittal, coro-
nal, and transverse plane knee loads) of forces produce
even a greater strain on the ACL than an isolated
anterior translation force.
The most common non-contact ACL injury mechanism
is a deceleration task with high knee internal extension
torque (with or without perturbation) combined with
dynamic valgus rotation with the body weight shifted
over the injured leg and the plantar surface of the foot
xed at on the playing surface.
Conclusions on non-contact ACL injury risk factors in
soccer players:
Dry weather conditions may increase non-contact ACL
injury risk, but evidence is mainly based on Australian
Football, which limits its potential to be generalized to
soccer players (Fig. 2; Table 1).
722 Knee Surg Sports Traumatol Arthrosc (2009) 17:705729
1 3
Articial Turf may place the soccer player to a higher
risk of non-contact ACL injury.
It is not clear whether an increased BMI places the
soccer players at a greater risk of non-contact ACL
rupture, and studies are mainly based on female
athletes.
Generalized joint laxity (which was found to be higher
for female athletes) and anteriorposterior knee joint
laxity have been associated with an increased risk of
non-contact ACL injury for both males and females.
The exact role of pelvis and trunk needs to be further
studied in soccer players.
There is not enough evidence to support than an
increased Q-angle is a risk factor for non-contact ACL
injuries in soccer player
Small and narrow intercondylar notch width (ratio of
notch width to the diameter and cross sectional area of
the ACL) were found to be risk factors for ACL
injuries.
Differences in ACL size and strength between males
and females have been identied. Small and weak
ACLs contribute to an increased risk of ACL rupture.
Pre-ovulatory phase of menstrual cycle in females not
using oral contraceptive were reported to be risk factors
for non-contact ACL injuries.
Despite the increased knee laxity around the ovulation
may decrease with the use of oral contraceptives in
female soccer players; further evidence is needed
before this medication can be systematically prescribed
in order to decrease the non-contact ACL injuries.
Sex hormones may decrease motor coordination in
female athletes and may play a role in non-contact ACL
injuries.
Decreased relative (to quadriceps) hamstring strength
and recruitment place the soccer player to an increased
risk of non-contact ACL injury.
Muscular fatigue may increase the risk of non-contact
ACL injury by altering the neuromuscular control.
Decreased Core strength and proprioception may
place the soccer players to a higher risk of non-contact
ACL injury.
Low trunk, hip, and knee exion angles, and high
dorsiexion of the ankle when performing sport tasks
increase the risk of non-contact ACL injuries.
Lateral trunk displacement and hip adduction combined
with increased knee abduction moments (dynamic knee
valgus) increase the risk of non-contact ACL injuries.
Increased hip internal rotation and tibial external
rotation with or without foot pronation are risk factors
for non-contact ACL injuries.
Mechanisms and risk factors for non-contact ACL
injuries have been mainly studied in female soccer players;
thus, further research in male players is warranted.
Fig. 2 Risk factors for ACL injury: a causation model (reproduced from Bahr R, Krosshaug T (2005) Understanding injury mechanisms: a key
component of preventing injuries in sport. BJSM 39:324329 with permission from the publisher)
Knee Surg Sports Traumatol Arthrosc (2009) 17:705729 723
1 3
Continued efforts to identify the most modiable risk
factors to ACL injury in soccer players is currently the only
option to prevent the high risk of osteoarthritis following
this traumatic injury. Pre-season screening programs that
monitor important risk factors (especially those that are
modiable) to identify soccer players with potential decits
are warranted to help target high risk athletes with the
most effective neuromuscular training interventions.
Acknowledgments The authors would like to thank Professor
Rodrigo C Miralles, from Universitat Rovira i Virgili and Hospital de
Sant Joan, Reus, for his excellent contributions, helpful comments
and interesting suggestions. We would also like to thank Dr. Gerard
Moras for his advices and critical reading of the manuscript. One
author (GDM) would like to acknowledge funding support from
National Institutes of Health Grants R01-AR049735 and R01-
AR055563.
Conict of interest statement No conict of interest is declared.
References
1. Adachi N, Nawata K, Maeta M, Kurozawa Y (2008) Relation-
ship of the menstrual cycle phase to anterior cruciate ligament
injuries in teenaged female athletes. Arch Orthop Trauma Surg
128:473478
2. Allen MK, Glasoe WM (2000) Metrecom measurement of
navicular drop in subjects with anterior cruciate ligament injury.
J Athl Train 35:403406
3. Arendt E, Dick R (1995) Knee injury patterns among men and
women in collegiate basketball and soccer. NCAA data and
review of literature. Am J Sports Med 23:694701
4. Arendt EA, Agel J, Dick R (1999) Anterior cruciate ligament
injury patterns among collegiate men and women. J Athl Train
34:8692
5. Arendt EA, Bershadsky B, Agel J (2002) Periodicity of non-
contact anterior cruciate ligament injuries during the menstrual
cycle. J Gend Specif Med 5:1926
6. Arnason A, Gudmundsson A, Dahl HA, Johannsson E (1996)
Soccer injuries in Iceland. Scand J Med Sci Sports 6:4045
7. Baratta R, Solomonow M, Zhou BH, Letson D, Chuinard R,
DAmbrosia R (1988) Muscular coactivation. The role of the
antagonist musculature in maintaining knee stability. Am J
Sports Med 16:113122
8. Beckett ME, Massie DL, Bowers KD, Stoll DA (1992) Inci-
dence of hyperpronation in the ACL injured knee: a clinical
perspective. J Athl Train 27:5862
9. Bellchamber TL, Van den Bogert AJ (2000) Contributions of
proximal and distal moments to axial tibial rotation during
walking and running. J Biomech 33:13971403
10. Berns GS, Hull ML, Patterson HA (1992) Strain in the anteri-
ormedial bundle of the anterior cruciate ligament under com-
bined loading. J Orthop Res 10:167176
11. Besier TF, Lloyd DG, Ackland T, Cochrane JL (2001) Antici-
patory effects on knee joint loading during running and cutting
maneuvers. Med Sci Sports Exerc 33:11761181
12. Besier TF, Lloyd DG, Cochrane JL, Ackland T (2001) External
loading of the knee joint during running and cutting maneuvers.
Med Sci Sports Exerc 33:11681175
13. Beynnon BD, Fleming BC (1998) Anterior cruciate ligament
strain in-vivo: a review of previous work. J Biomech 31:519525
14. Beynnon BD, Johnson RJ, Braun S, Sargent M, Bernstein IM,
Skelly JM, Vacek PM (2006) The relationship between men-
strual cycle phase and anterior cruciate ligament injury: a case-
control study of recreational alpine skiers. Am J Sports Med
34:757764
15. Bjordal JM, Arnoy F, Hannestad B, Strand T (1997) Epidemi-
ology of anterior cruciate ligament injuries in soccer. Am J
Sports Med 25:341345
16. Blackburn JT, Padua DA (2008) Inuence of trunk exion on
hip and knee joint kinematics during a controlled drop landing.
Clin Biomech (Bristol, Avon) 23:313319
17. Boden BP, Dean GS, Feagin JA, Garrett WE (2000) Mecha-
nisms of anterior cruciate ligament injury. Orthopedics 23:573
578
18. Booth FW, Tipton CM (1970) Ligamentous strength measure-
ments in pre-pubescent and pubescent rats. Growth 34:177185
19. Borotikar BS, Newcomer R, Koppes R, McLean SG (2008)
Combined effects of fatigue and decision making on female
lower limb landing postures: central and peripheral contribu-
tions to ACL injury risk. Clin Biomech (Bristol, Avon)
23:8192
20. Bowers KD, Martin RB (1974) Impact absorption, new and old
astroturf at West Virginia University. Med Sci Sports 6:217221
21. Bowers KD, Martin RB (1975) Cleat-surface friction on new
and old Astroturf. Med Science Sport 7:123135
22. Brown CN, Yu B, Kirkendall DT, Garrett WE (2005) Effects of
increased body mass index on lower extremity motion patterns
in a stop-jump task. J Athl Train 42:S26
23. Buchanan PA (2003) Developmental perspectives on basketball
players strength, knee position in landing, and ACLinjury gender
differences. Dissertation, Indiana University, Bloomington
24. Buehler-Yund C (1999) A longitudinal study of injury rates and
risk factors in 5 to 12 year old soccer players. In: Environmental
health. University of Cincinnati, Cincinnati, p 161
25. Burkhart BG, Ford KR, Myer GD, Heidt RS, Hewett TE (2008)
Anterior cruciate ligament tear in an athlete: does increased heel
loading increase ACL injury risk? N Am J Sports Phys Ther 3(3)
26. Chandrashekar N, Slauterbeck J, Hashemi J (2005) Sex-based
differences in the anthropometric characteristics of the anterior
cruciate ligament and its relation to intercondylar notch geom-
etry. Am J Sports Med 33:14921498
27. Chandrashekar NJ, Mansour M, Slauterbeck J, Hashemi J (2006)
Sex-based differences in the tensile properties of the human
anterior cruciate ligament. J Biomech 39:29432950
28. Chappell JD, Creighton RA, Giuliani C, Yu B, Garrett WE
(2007) Kinematics and electromyography of landing preparation
in vertical stop-jump: risks for noncontact anterior cruciate
ligament injury. Am J Sports Med 35:235241
29. Chappell JD, Herman DC, Knight BS, Kirkendall DT, Garrett
WE, Yu B (2005) Effect of fatigue on knee kinetics and kine-
matics in stop-jump tasks. Am J Sports Med 33:10221029
30. Chappell JD, Yu B, Kirkendall DT, Garrett WE (2002) A
comparison of knee kinetics between male and female recrea-
tional athletes in stop-jump tasks. Am J Sports Med 30:261267
31. Chaudhari AM, Lindenfeld TN, Andriacchi TP, Hewett TE,
Riccobene J, Myer GD, Noyes FR (2007) Knee and hip loading
patterns at different phases in the menstrual cycle: implications
for the gender difference in anterior cruciate ligament injury
rates. Am J Sports Med 35:793800
32. Colby S, Francisco A, Yu B, Kirkendall D, Finch M, Garrett WE
(2000) Electromyographic and kinematic analysis of cutting
maneuvers: implications for anterior cruciate ligament injury.
Am J Sports Med 28:234240
33. Coplan JA (1989) Rotational motion of the knee. A comparison
of normal and pronating subjects. J Orthop Sports Phys Ther
10:366369
724 Knee Surg Sports Traumatol Arthrosc (2009) 17:705729
1 3
34. Cortes N, Onate J, Abrantes J, Gagen L, Dowling E, Van Lunen
B (2007) Effects of gender and foot-landing techniques on lower
extremity kinematics during drop-jump landings. J Appl Bio-
mech 23:289299
35. Decker MJ, Torry MR, Wyland DJ, Sterett WI, Richard Stead-
man J (2003) Gender differences in lower extremity kinematics,
kinetics and energy absorption during landing. Clin Biomech
(Bristol, Avon) 18:662669
36. Delco AJ, Garrett WE (1998) Mechanisms of injury of the
ACL in soccer players. Clin Sport Med 17:779785
37. Delp SL, Hess WE, Hungerford DS, Jones LC(1999) Variation of
rotation moment arms with hip exion. J Biomech 32:493501
38. DeMorat G, Weinhold P, Blackburn T, Chudik S, Garrett WE
(2004) Aggressive quadriceps loading can induce noncontact
anterior cruciate ligament injury. Am J Sports Med 32:477
483
39. Dienst M, Schneider G, Altmeyer K, Voelkering K, Georg T,
Kramann B, Kohn D (2007) Correlation of intercondylar notch
cross sections to the ACL size: a high resolution MRtomographic
in vivo analysis. Arch Orthop Trauma Surg 127:253260
40. Ekstrand J, Timpka T, Hagglund M (2006) Risk of injury in elite
football played on articial turf versus natural grass: a pro-
spective two-cohort study. Br J Sports Med 40:975980
41. Endsley ML, Ford KR, Myer GD, Slauterbeck JR, Hewett TE
(2003) The effects of gender on dynamic knee stability and
Q-angle in young athletes. In: Ohio Physical Therapy Association
fall conference. Cleveland State University, Cleveland
42. Engstrom B, Forssblad M, Johansson C, Tornkvist H (1990)
Does a major knee injury denitely sideline an elite soccer
player? Am J Sports Med 18:101105
43. Ergun M, Islegen C, Taskiran E (2004) A cross-sectional anal-
ysis of sagittal knee laxity and isokinetic muscle strength in
soccer players. Int J Sports Med 25:594598
44. Fagenbaum R, Darling WG (2003) Jump landing strategies in
male and female college athletes and the implications of such
strategies for anterior cruciate ligament injury. Am J Sports Med
31:233240
45. Fauno P, Wulff Jakobsen B (2006) Mechanism of ACL injuries
in soccer. Int J Sports Med 27:7579
46. Feagin JA, Lambert KL (1985) Mechanism of injury and
pathology of anterior cruciate ligament injuries. Orthop Clin
North Am 16:4145
47. Federation Internationale de Football Association (FIFA)
(2008) Web page: http://www.fa.com/mm/document/fafacts/
bcoffsurv/bigcount.statspackage_7024.pdf
48. Fleming BC, Ohlen G, Renstrom PA, Peura GD, Beynnon BD,
Badger GJ (2003) The effects of compressive load and knee
joint torque on peak anterior cruciate ligament strains. Am J
Sports Med 31:701707
49. Fleming BC, Renstrom PA, Ohlen G, Johnson RJ, Peura GD,
Beynnon BD, Badger GJ (2001) The gastrocnemius muscle is an
antagonist of the anterior cruciate ligament. J Orthop Res
19:11781184
50. Ford KR, Manson NA, Evans BJ, Myer GD, Gwin RC, Heidt
RS, Hewett TE (2006) Comparison of in-shoe foot loading
patterns on natural grass and synthetic turf. J Sci Med Sport
9:433440
51. Ford KR, Myer GD, Hewett TE (2003) Valgus knee motion
during landing in high school female and male basketball
players. Med Sci Sports Exerc 35:17451750
52. Ford KR, Myer GD, Toms HE, Hewett TE (2005) Gender dif-
ferences in the kinematics of unanticipated cutting in young
athletes. Med Sci Sports Exerc 37:124129
53. Fornalski S, McGarry MH, Csintalan RP, Fithian DC, Lee TQ
(2008) Biomechanical and anatomical assessment after knee
hyperextension injury. Am J Sport Med 36:8084
54. Fuller CW, Dick RW, Corlette J, Schmalz R (2007) Com-
parison of the incidence, nature and cause of injuries sus-
tained on grass and new generation articial turf by male and
female football players. Part 2: training injuries. Br J Sports
Med 41(Suppl 1):i27i32
55. Fuller CW, Dick RW, Corlette J, Schmalz R(2007) Comparison of
the incidence, nature and cause of injuries sustained on grass and
new generation articial turf by male and female football players.
Part 1: match injuries. Br J Sports Med 41(Suppl 1):i20i26
56. Gottlob CA, Baker CL (2000) Anterior cruciate ligament
reconstruction: socioeconomic issues and cost effectiveness. Am
J Orthop 29:472476
57. Gottlob CA, Baker CL, Pellissier JM, Colvin L (1999) Cost
effectiveness of anterior cruciate ligament reconstruction in
young adults. Clin Orthop Relat Res 367:272282
58. Granata KP, Padua DA, Wilson SE (2002) Gender differences in
active musculoskeletal stiffness, part II: quantication of leg
stiffness during functional hopping tasks. J Electromyogr
Kinesiol 12:127135
59. Granata KP, Wilson SE, Padua DA (2002) Gender differences in
active musculoskeletal stiffness, part I: quantication in con-
trolled measurements of knee joint dynamics. J Electromyogr
Kinesiol 12:119126
60. Gray J, Taunton JE, McKenzie DC, Clement DB, McConkey JP,
Davidson RG (1985) A survey of injuries to the anterior cruciate
ligament of the knee in female basketball players. Int J Sports
Med 6:314316
61. Grifn LY, Agel J, Albohm MJ, Arendt EA, Dick RW, Garrett
WE, Garrick JG, Hewett TE, Huston LJ, Ireland ML, Johnson
RJ, Kibler WB (2000) Noncontact anterior cruciate ligament
injuries: risk factors and prevention strategies. J Am Acad
Orthop Surg 8:141150
62. Grifn LY, Albohm MJ, Arendt EA, Bahr R, Beynnon BD,
DeMaio M, Dick RW, Engebretsen L, Garrett WE, Hannan JA,
Hewett TE, Huston LJ (2006) Understanding and preventing
noncontact anterior cruciate ligament injuries. A review of the
Hunt Valley II Meeting, January 2005. Am J Sports Med
34:15121532
63. Hame SL, Oakes DA, Markolf KL (2002) Injury to the anterior
cruciate ligament during alpine skiing: a biomechanical analysis
of tibial torque and knee exion angle. Am J Sports Med
30:537540
64. Hashemi J, Chandrashekar N, Mansouri H, Slauterbeck JR,
Hardy DM (2008) The human anterior cruciate ligament: sex
differences in ultrastructural and correlation with biomechanical
properties. J Orthop Res 26:945950
65. Heiderscheit BC, Hamill J, Caldwell GE (2000) Inuence of
Q-angle on lower-extremity running kinematics. J Orthop Sports
Phys Ther 30:271278
66. Heidt RS, Dormer SG, Cawley PW, Scranton PE, Losse G,
Howard M (1996) Differences in friction and torsional resis-
tance in athletic shoe-turf surface interfaces. Am J Sports Med
24:834842
67. Heise GD, Bohne M, Bressel E (2001) Muscle preactivation and
leg stiffness in men and women during hopping. In: American
Society of Biomechanics annual meeting, San Diego, CA
68. Hewett TE (2000) Neuromuscular and hormonal factors asso-
ciated with knee injuries in female athletes. Strategies for
intervention. Sports Med 29:313327
69. Hewett TE (2007) Biomechanical and neuromuscular mecha-
nisms of ACL injuries. In: Hewett TE, Shultz SJ, Grifn LY
(eds) Understanding and preventing non-contact ACL injuries,
1st edn. Human Kinetics, Champaign, pp 129130
70. Hewett TE, Myer GD (2000) The effects of oral contraceptives
on knee stability and neuromuscular performance in female
athletes. Med Sci Sports Exerc 32:S207
Knee Surg Sports Traumatol Arthrosc (2009) 17:705729 725
1 3
71. Hewett TE, Myer GD, Ford KR (2006) Anterior cruciate liga-
ment injuries in female athletes, part 1: mechanisms and risk
factors. Am J Sports Med 34:299311
72. Hewett TE, Myer GD, Ford KR (2004) Decrease in neuromus-
cular control about the knee with maturation in female athletes.
J Bone Joint Surg Am 86:16011608
73. Hewett TE, Myer GD, Ford KR, Heidt RS, Colosimo AJ,
McLean SG, Van den Bogert AJ, Paterno MV, Succop P (2005)
Biomechanical measures of neuromuscular control and valgus
loading of the knee predict anterior cruciate ligament injury risk
in female athletes: a prospective study. Am J Sports Med 33:
492501
74. Hewett TE, Stroupe AL, Nance TA, Noyes FR (1996) Plyo-
metric training in female athletes. Decreased impact forces and
increased hamstring torques. Am J Sports Med 24:765773
75. Hewett TE, Zazulak BT, Myer GD (2007) Effects of the men-
strual cycle on anterior cruciate ligament injury risk: a system-
atic review. Am J Sports Med 35:659668
76. Hicks-Little CA, Thatcher JR, Hauth JM, Goldfuss AJ, Cordova
ML (2007) Menstrual cycle stage and oral contraceptive effects
on anterior tibial displacement in collegiate female athletes.
J Sports Med Phys Fitness 47:255260
77. Hoff GL, Martin TA (1986) Outdoor and indoor soccer injuries.
Am J Sports Med 14:231233
78. Houck JR, Duncan A, De Haven KE (2006) Comparison of
frontal plane trunk kinematics and hip and knee moments during
anticipated and unanticipated walking and side step cutting
tasks. Gait Posture 24:314322
79. Huston LJ (2007) Clinical biomechanical studies on ACL injury
risk factors. In: Hewett TE, Shultz SJ, Grifn LY (eds) Under-
standing and preventing non-contact ACL injuries, 1st edn.
Human Kinetics, Champaign, pp 141154
80. Huston LJ, Vibert B, Ashton-Miller JA, Wojtys EM (2001)
Gender differences in knee angle when landing from a drop-
jump. Am J Knee Surg 14:215219
81. Huston LJ, Wojtys EM (1996) Neuromuscular performance
characteristics in elite female athletes. Am J Sports Med
24:427436
82. Imran A, OConnor JJ (1997) Theoretical estimates of cruciate
ligament forces: effects of tibial surface geometry and ligament
orientations. Proc Inst Mech Eng 211:425439
83. Imwalle LE, Myer GD, Ford KR, Hewett TE (2008) The rela-
tionship between hip and knee kinematics in female athletes
during cutting maneuvers: a possible link to non-contact ACL
injury and prevention. J Strength Cond Res (in press)
84. Ireland ML (1999) Anterior cruciate ligament injury in female
athletes: epidemiology. J Athl Train 34:150154
85. Jacobs CA, Uhl TL, Mattacola CG, Shapiro R, Rayens WS
(2007) Hip abductor function and lower extremity landing
kinematics: sex differences. J Athl Train 42:7683
86. Jenkins WL, Killian CB, Williams DS, Loudon J, Raedeke SG
(2007) Anterior cruciate ligament injury in female and male
athletes: the relationship between foot structure and injury. J Am
Podiatr Med Assoc 97:371376
87. Kaufman KR, An KN, Litchy WJ, Chao EY (1991) Physiolog-
ical prediction of muscle forces, II: application to isokinetic
exercise. Neuroscience 40:793804
88. Kibler WB, Livingston B (2001) Closed-chain rehabilitation for
upper and lower extremities. J Am Acad Orthop Surg 9:412421
89. Kirkendall DT, Garrett WE (2000) The anterior cruciate liga-
ment enigma. Injury mechanisms and prevention. Clin Orthop
Relat Res 372:6468
90. Knapik JJ, Bauman CL, Jones BH, Harris JM, Vaughan L
(1991) Preseason strength and exibility imbalances associated
with athletic injuries in female collegiate athletes. Am J Sports
Med 19:7681
91. Knapik JJ, Sharp MA, Canham-Chervak M, Hauret K, Patton JF,
Jones BH (2001) Risk factors for training-related injuries among
men and women in basic combat training. Med Sci Sports Exerc
33:946954
92. Komatsuda T, Sugita T, Sano H, Kusakabe T, Watanuki M,
Yoshizumi Y, Murakami T, Hashimoto M, Kokubun S (2006)
Does estrogen alter the mechanical properties of the anterior
cruciate ligament? An experimental study in rabbits. Acta Ort-
hop 77:973980
93. Krosshaug T, Krosshaug T, Andersen TE, Olsen OE, Myklebust
G, Bahr R (2005) Research approaches to describe the mecha-
nisms of injuries in sport: limitations and possibilities. Br J
Sports Med 39:330339
94. Krosshaug T, Nakamae A, Boden BP, Engebretsen L, Smith G,
Slauterbeck JR, Hewett TE, Bahr R (2007) Mechanisms of
anterior cruciate ligament injury in basketball: video analysis of
39 cases. Am J Sports Med 35:359367
95. Kucera KL, Marshall SW, Kirkendall DT, Marchak PM, Garrett
WE (2005) Injury history as a risk factor for incident injury in
youth soccer. Br J Sports Med 39:462
96. Lambson RB, Barnhill BS, Higgins RW (1996) Football cleat
design and its effect on ACL injuries. A three-year prospective
study. Am J Sports Med 24:155159
97. Landry SC, McKean KA, Hubley-Kozey CL, Stanish WD,
Deluzio KJ (2007) Neuromuscular and lower limb biomechan-
ical differences exist between male and female elite adolescent
soccer players during an unanticipated run and crosscut
maneuver. Am J Sports Med 35:19011911
98. Landry SC, McKean KA, Hubley-Kozey CL, Stanish WD,
Deluzio KJ (2007) Neuromuscular and lower limb biomechan-
ical differences exist between male and female elite adolescent
soccer players during an unanticipated side-cut maneuver. Am J
Sports Med 35:18881900
99. LaPrade RF, Burnett QM (1994) Femoral intercondylar notch
stenosis and correlation to anterior cruciate ligament injuries: a
prospective study. Am J Sports Med 22:198203
100. Lebrun CM (1994) The effect of the phase of the menstrual
cycle and the birth control pill in athletic performance. Clin
Sports Med 13:419441
101. Lees A, Nolan L (1998) The biomechanics of soccer: a review.
J Sports Sci 16:211234
102. Lephart SM, Ferris CM, Riemann BL, Myers JB, Fu FH (2002)
Gender differences in strength and lower extremity kinematics
during landing. Clin Orthop Relat Res 401:162169
103. Li G, Papannagari R, DeFrate LE, Yoo JD, Park SE, Gill TJ
(2006) Comparison of the ACL and ACL graft forces before and
after ACL reconstruction: an in-vitro robotic investigation. Acta
Orthop 77:267274
104. Li G, Rudy TW, Sakane M, Kanamori A, Ma CB, Woo SL
(1999) The importance of quadriceps and hamstring muscle
loading on knee kinematics and in-situ forces in the ACL.
J Biomech 32:395400
105. Liu SH, Al-Shaikh R, Panossian V, Yang RS, Nelson SD,
Soleiman N, Finerman GA, Lane JM (1996) Primary immuno-
localization of estrogen and progesterone target cells in the
human anterior cruciate ligament. J Orthop Res 14:526533
106. Lohmander LS, Englund PM, Dahl LL, Roos EM (2007) The
long-term consequence of anterior cruciate ligament and
meniscus injuries: osteoarthritis. Am J Sports Med 35:1756
1769
107. Loudon JK, Jenkins W, Loudon KL (1996) The relationship
between static posture and ACL injury in female athletes.
J Orthop Sports Phys Ther 24:9197
108. Mair S, Seaber A, Glisson R, Garrett WE (1996) The role of
fatigue in susceptibility to acute muscle strain injury. Am
J Sports Med 24:137143
726 Knee Surg Sports Traumatol Arthrosc (2009) 17:705729
1 3
109. Malinzak RA, Colby SM, Kirkendall DT, Yu B, Garrett WE
(2001) A comparison of knee joint motion patterns between men
and women in selected athletic tasks. Clin Biomech (Bristol,
Avon) 16:438445
110. Markolf KL, Burcheld DM, Shapiro MM, Shepard MF, Fin-
erman GA, Slauterbeck JL (1995) Combined knee loading states
that generate high anterior cruciate ligament forces. J Orthop
Res 13:930935
111. Markolf KL, Gorek JF, Kabo JM, Shapiro MS (1990) Direct
measurement of resultant forces in the anterior cruciate liga-
ment. An in vitro study performed with a new experimental
technique. J Bone Joint Surg Am 72:557567
112. Martineau PA, Al-Jassir F, Lenczner E, Burman ML (2004)
Effect of the oral contraceptive pill on ligamentous laxity. Clin J
Sport Med 14:281286
113. McLean SG, Fellin RE, Suedekum N, Calabrese G, Passerallo
A, Joy S (2007) Impact of fatigue on gender-based high-risk
landing strategies. Med Sci Sports Exerc 39:502514
114. McLean SG, Huang X, Su A, Van den Bogert AJ (2004) Sagittal
plane biomechanics cannot injure the ACL during sidestep
cutting. Clin Biomech (Bristol, Avon) 19:828838
115. McLean SG, Lipfert SW, Van den Bogert AJ (2004) Effect of
gender and defensive opponent on the biomechanics of sidestep
cutting. Med Sci Sports Exerc 36:10081016
116. McLean SG, Neal RJ, Myers PT, Walters MR (1999) Knee joint
kinematics during the sidestep cutting maneuver: potential for
injury in women. Med Sci Sports Exerc 31:959968
117. McNair P, Marshall R, Matheson J (1990) Important features
associated with acute anterior cruciate ligament injury. N Z Med
J 103:537539
118. Meister K, Talley MC, Horodyski MB, Indelicato PA, Hartzel
JS, Batts J (1998) Caudal slope of the tibia and its relationship to
non-contact injuries to the ACL. Am J Knee Surg 11:217219
119. Melnyk M, Gollhofer A (2007) Submaximal fatigue of the
hamstring impairs specic reex components and knee stability.
Knee Surg Sports Traum Arthrosc 15:525532
120. Meunier A, Odensten M, Good L (2007) Long-term results after
primary repair or non-surgical treatment of anterior cruciate
ligament rupture: a randomized study with a 15-year follow-up.
Scand J Med Sci Sports 17:230237
121. Miralles RC, Miralles I (2007) Biomecanica de las desalineac-
iones. In: Miralles RC, Miralles I (eds) Biomecanica cl nica de
las patolog as del aparato locomotor, 1st edn. Masson, Barce-
lona, pp 7174
122. Miralles RC, Saltor M (1987) Los vicios de torsion de la
extremidad inferior. Rev Ortop Traumatol 33IB:131135
123. Mitchell LC, Ford KR, Minning SJ, Myer GD, Manigne RE,
Hewett TE (2008) Effect of medial foot loading pattern on
ankle and knee landing biomechanics. N Am J Sports Phys
Ther 3(3)
124. Mizuno Y, Kumagai M, Mattessich SM, Elias JJ, Ramrattan N,
Cosgarea AJ, Chao EY (2001) Q-angle inuences tibiofemoral
and patellofemoral kinematics. J Orthop Res 19:834840
125. Moller Nielsen J, Hammar M (1991) Sports injuries and oral
contraceptive use: is there a relationship? Sports Med 12:152
160
126. More RC, Karras BT, Neiman F, Fritschy D, Woo SL, Daniel
DM (1993) Hamstringsan anterior cruciate ligament protag-
onist. An in vivo study. Am J Sports Med 21:231237
127. Muneta T, Takakuda K, Yamamoto H (1997) Intercondylar
notch width and its relation to the conguration and cross-sec-
tional area of the anterior cruciate ligament. A cadaveric knee
study. Am J Sports Med 25:6972
128. Murphy DF, Connolly DA, Beynnon BD (2003) Risk factors for
lower extremity injury: a review of the literature. Br J Sports
Med 37:1329
129. Myer GD, Ford KR, Barber Foss K, Liu C, Nick TG, Hewett TE
(2009) The relationship of hamstrings and quadriceps strength to
anterior cruciate ligament injury in female athletes. Clin J Sport
Med 19:38
130. Myer GD, Ford KR, Brent JL, Hewett TE (2007) Differential
neuromuscular training effects on ACL injury risk factors in
high-risk versus low-risk athletes. BMC Musculoskelet
Disord 8:39
131. Myer GD, Ford KR, Hewett TE (2005) The effects of gender on
quadriceps muscle activation strategies during a maneuver that
mimics a high ACL injury risk position. J Electromyogr Kine-
siol 15:181189
132. Myer GD, Ford KR, Palumbo JP, Hewett TE (2005) Neuro-
muscular training improves performance and lower extremity
biomechanics in female athletes. J Strength Cond Res 19:5160
133. Myer GD, Ford KR, Paterno MV, Nick TG, Hewett TE (2008)
The effects of generalized joint laxity on risk of anterior cruciate
ligament injury in young female athletes. Am J Sports Med
36:10731080
134. Myklebust G, Bahr R (2005) Return to play guidelines after
anterior cruciate ligament surgery. Br J Sports Med 39:127131
135. Myklebust G, Engebretsen L, Braekken IH, Skjolberg A, Olsen
OE, Bahr R (2003) Prevention of anterior cruciate ligament
injuries in female team handball players: a prospective inter-
vention study over three seasons. Clin J Sport Med 13:7178
136. Neuman P, Englund M, Kostogiannis I, Friden T, Roos H,
Dahlberg LE (2008) Prevalence of tibiofemoral osteoarthritis
15 years after nonoperative treatment of anterior cruciate liga-
ment injury: a prospective cohort study. Am J Sports Med
36:17171725
137. Noyes F, Matthews D, Mooar P, Grood ES (1983) The symp-
tomatic ACL-decient knee. Part II: The results of rehabilita-
tion, activity modication, and counseling on functional
disability. J Bone Joint Surg Am 65:163174
138. Noyes F, Mooar P, Matthews D, Butler DL (1983) The symp-
tomatic ACL-decient knee. Part I: The long-term functional
disability in athletically active individuals. J Bone Joint Surg
Am 65:154162
139. Nyland JA, Caborn DN, Shapiro R, Johnson DL (1999) Cross-
over cutting during hamstring fatigue produces transverse plane
knee control decits. J Athl Train 34:137143
140. Nyland JA, Caborn DN, Shapiro R, Johnson DL (1997) Fatigue
after eccentric quadriceps femoris work produces earlier gas-
trocnemius and delayed quadriceps femoris activation during
crossover cutting among normal athletic women. Knee Surg
Sports Traumatol Arthrosc 5:162167
141. Olsen OE, Myklebust G, Engebretsen L, Bahr R (2004) Injury
mechanisms for anterior cruciate ligament injuries in team
handball. Am J Sports Med 32:10021012
142. Orchard J (2002) Is there a relationship between ground and
climatic conditions and injuries in football? Sports Med 32:419
432
143. Orchard J, Chivers I, Aldous D, Bennell K, Seward H (2005)
Rye grass is associated with fewer non-contact anterior cruciate
ligament injuries than bermuda grass. Br J Sports Med 39:704
709
144. Orchard J, Seward H, McGivern J, Hood S (1999) Rainfall,
evaporation and the risk of non-contact anterior cruciate liga-
ment injury in the Australian Football League. Med J Aust
170:304306
145. Orchard JW, Powell JW (2003) Risk of knee and ankle sprains
under various weather conditions in American Football. Med Sci
Sports Exerc 35:11181123
146. Ostenberg A, Roos H (2000) Injury risk factors in female
European football: a prospective study of 123 players during one
season. Scand J Med Sci Sports 10:279285
Knee Surg Sports Traumatol Arthrosc (2009) 17:705729 727
1 3
147. Padua DA, Carcia CR, Arnold BL, Granata KP (2005) Gender
differences in leg stiffness and stiffness recruitment strategy
during two-legged hopping. J Mot Behav 37:111125
148. Pantano KJ, White SC, Gilchrist LA, Leddy J (2005) Differ-
ences in peak knee valgus angles between individuals with high
and low Q-angles during a single limb squat. Clin Biomech
(Bristol, Avon) 20:966972
149. Park HS, Wilson NA, Zhang LQ (2008) Gender differences in
passive knee biomechanical properties in tibial rotation. J Ort-
hop Res 26:937944
150. Pum MA, Shelburne KB, Torry MR, Decker MJ, Pandy MG
(2004) Model prediction of anterior cruciate ligament force
during drop-landings. Med Sci Sports Exerc 36:19491958
151. Pollard CD, Davis IM, Hamill J (2004) Inuence of gender on
hip and knee mechanics during a randomly cued cutting
maneuver. Clin Biomech (Bristol, Avon) 19:10221031
152. Posthuma BW, Bass MJ, Bull SB, Nisker JA (1987) Detecting
changes in functional ability in women with premenstrual syn-
drome. Am J Obstet Gynecol 156:275278
153. Powers CM (2003) The inuence of altered lower-extremity
kinematics on patellofemoral joint dysfunction: a theoretical
perspective. J Orthop Sports Phys Ther 33:639646
154. Ramesh R, Von Arx O, Azzopardi T, Schranz PJ (2005) The risk
of anterior cruciate ligament rupture with generalized joint
laxity. J Bone Joint Surg Br 87:800803
155. Renstrom P, Arms SW, Stanwyck TS, Johnson RJ, Pope MH
(1986) Strain within the anterior cruciate ligament during
hamstring and quadriceps activity. Am J Sports Med 14:8387
156. Renstrom P, Ljungqvist A, Arendt E, Beynnon B, Fukubayashi
T, Garrett W, Georgoulis T, Hewett TE, Johnson R, Krosshaug
T, Mandelbaum B, Micheli L, Myklebust G, Roos E, Roos H,
Schamasch P, Shultz S, Werner S, Wojtys E, Engebretsen L
(2008) Non-contact ACL injuries in female athletes: an Inter-
national Olympic Committee current concepts statement. Br J
Sports Med 42:394412
157. Ruedl G, Ploner P, Linortner I, Schranz A, Fink C, Sommers-
acher R, Pocecco E, Nachbauer W, Burtscher M (2009) Are oral
contraceptive use and menstrual cycle phase related to anterior
cruciate ligament injury risk in female recreational skiers? Knee
Surg Sports Traum Arthrosc Mar 31. [Epub ahead of print]
158. Ryder SH, Johnson RJ, Beynnon BD, Ettlinger CF (1997) Pre-
vention of ACL injuries. J Sport Rehab 6:8096
159. Sarwar R, Niclos BB, Rutherford OM (1996) Changes in muscle
strength, relaxation rate and fatiguability during the human
menstrual cycle. J Physiol 493:267272
160. Schickendantz MS, Weiker GG (1993) The predictive value of
radiographs in the evaluation of unilateral and bilateral anterior
cruciate ligament injuries. Am J Sports Med 21:110113
161. Schmitz RJ, Ficklin TK, Shimokochi Y, Nguyen AD, Beynnon
BD, Perrin DH, Shultz SJ (2008) Varus/valgus and internal/
external torsional knee joint stiffness differs between sexes. Am
J Sports Med 36:13801388
162. Scranton P, Whitesel J, Powell J, Dormer SG, Heidt RS, Losse
G, Cawley PW (1997) A review of selected noncontact anterior
cruciate ligament injuries in the National Football League. Foot
Ankle Int 18:772776
163. Self BP, Paine D (2001) Ankle biomechanics during four
landing techniques. Med Sci Sports Exerc 33:13381344
164. Shambaugh JP, Klein A, Herbert JH (1991) Structural measures
as predictors of injury in basketball players. Med Sci Sports
Exerc 23:522527
165. Shelbourne KD, Kerr B (2001) The relationship of femoral in-
tercondylar notch width to height, and sex in patients with intact
anterior cruciate ligaments. Am J Knee Surg 14:9296
166. Shultz SJ (2007) Hormonal inuences on ligament biology.
In: Hewett TE, Shultz SJ, Grifn LY (eds) Understanding and
preventing non-contact ACL injuries, 1st edn. Human Kinetics,
Champaign, pp 219238
167. Shultz SJ, Nguyen AD, Beynnon BD (2007) Anatomical factors
in ACL injury risk. In: Hewett TE, Shultz SJ, Grifn LY (eds)
Understanding and preventing non-contact ACL injuries, 1st
edn. Human Kinetics, Champaign, pp 239258
168. Slauterbeck JR, Fuzie SF, Smith MP, Clark RJ, Xu K, Starch
DW, Hardy DM (2002) The menstrual cycle, sex hormones, and
anterior cruciate ligament injury. J Athl Train 37:275278
169. Smith J, Szczerba JE, Arnold BL, Martin DE, Perrin DH (1997)
Role of hyperpronation as a possible risk factor for anterior
cruciate ligament injuries. J Athl Train 32:2528
170. Soderman K, Alfredson H, Pietila T, Werner S (2001) Risk
factors for leg injuries in female soccer players: a prospective
investigation during one out-door season. Knee Surg Sports
Traumatol Arthrosc 9:313321
171. Solomonow M, Baratta R, Zhou BH, Shoji H, Bose W, Beck C,
DAmbrosia R (1987) The synergistic action of the anterior
cruciate ligament and thigh muscles in maintaining joint sta-
bility. Am J Sports Med 15:207213
172. Souryal TO, Freeman TR (1993) Intercondylar notch size and
anterior cruciate ligament injuries in athletes: a prospective
study. Am J Sports Med 21:535539
173. Steffen K, Andersen TE, Bahr R (2007) Risk of injury on arti-
cial turf and natural grass in young female football players. Br
J Sports Med 41(Suppl 1):i33i37
174. Stijak L, Herzog RF, Schai P (2008) Is there an inuence of the
tibial slope of the lateral condyle on the ACL lesion? A case-
control study. Knee Surg Sports Traum Arthrosc 16:112117
175. Strickland SM, Belknap TW, Turner SA, Wright TM, Hannan
JA (2003) Lack of hormonal inuences on mechanical proper-
ties of sheep knee ligaments. Am J Sports Med 31:210215
176. Swenson TM, Harner CD (1995) Knee ligament and meniscal
injuries: current concepts. Orthop Clin North Am 26:529546
177. Teitz CC (2001) Video analysis of ACL injuries. In: Grifn LY
(ed) Prevention of Noncontact ACL Injuries, vol 1. American
Academy of Orthopaedic Surgeons, Rosemont, IL, pp 9396
178. Teitz CC, Lind BK, Sacks BM (1997) Symmetry of the femoral
notch width index. Am J Sports Med 25:687690
179. Torg JS, Stilwell G, Rogers K (1996) The effect of ambient
temperature on the shoe-surface interface release coefcient.
Am J Sports Med 24:7982
180. Uhorchak JM, Scoville CR, Williams GN, Arciero RA, St Pierre
P, Taylor DC (2003) Risk factors associated with noncontact
injury of the anteriorcruciate ligament: a prospective four-year
evaluation of 859 West Point cadets. Am J Sports Med 31:831
842
181. Wallace BJ, Kernozek TW, Mikat RP, Wright GA, Simons SZ,
Wallace KL (2008) A comparison between back squat exercise
and vertical jump kinematics: implications for determining
anterior cruciate ligament injury. J Strength Cond Res 22:1249
1258
182. Wascher DC, Markolf KL, Shapiro MS, Finerman GA (1993)
Direct in vitro measurement of force in the cruciate ligaments.
Part I: The effect of multiplane loading in the intact knee. J Bone
Joint Surg Am 75:377386
183. Withrow TJ, Huston LJ, Wojtys EM, Ashton-Miller JA (2006)
The effect of an impulsive knee valgus moment on in vitro
relative ACL strain during a simulated jump landing. Clin
Biomech (Bristol, Avon) 21:977983
184. Withrow TJ, Huston LJ, Wojtys EM, Ashton-Miller JA (2006)
The relationship between quadriceps muscle force, knee exion,
and anterior cruciate ligament strain in an in vitro simulated
jump landing. Am J Sports Med 34:269274
185. Withrow TJ, Huston LJ, Wojtys EM, Ashton-Miller JA (2008)
Effect of varying hamstring tension on anterior cruciate
728 Knee Surg Sports Traumatol Arthrosc (2009) 17:705729
1 3
ligament strain during in vitro impulsive knee exion and
compression loading. J Bone Joint Surg Am 90:815823
186. Wojtys EM, Ashton-Miller JA, Huston LJ (2002) A gender-
related difference in the contribution of the knee musculature to
sagittal-plane shear stiffness in subjects with similar knee laxity.
J Bone Joint Surg Am 84:1016
187. Wojtys EM, Huston LJ, Boynton MD, Spindler KP, Lindenfeld
TN (2002) The effect of the menstrual cycle on anterior cruciate
ligament injuries in women as determined by hormone levels.
Am J Sports Med 30:182188
188. Wojtys EM, Huston LJ, Lindenfeld TN, Hewett TE, Greeneld
ML (1998) Association between the menstrual cycle and ante-
rior cruciate ligament injuries in female athletes. Am J Sport
Med 26:614619
189. Wojtys EM, Huston LJ, Schock HJ, Boylan JP, Ashton-Miller
JA (2003) Gender differences in muscular protection of the knee
in torsion in size-matched athletes. J Bone Joint Surg Am
85:782789
190. Wojtys EM, Whylie BB, Huston LJ (1996) The effects of
muscle fatigue on neuromuscular function and anterior tibial
translation in healthy knees. Am J Sports Med 24:615621
191. Woo SL, Hollis JM, Adams DJ, Lyon RM, Takai S (1991)
Tensile properties of the human femur-anterior cruciate liga-
ment-tibia complex. The effects of specimen age and orienta-
tion. Am J Sports Med 19:217225
192. Woodford-Rogers B, Cyphert L, Denegar CR (1994) Risk fac-
tors for anterior cruciate ligament injury in high school and
college athletes. J Athl Train 29:343346
193. Woodhouse E, Schmale GA, Simonian P, Tencer A, Huber P,
Seidel K (2007) Reproductive hormone effects on strength of the
rat anterior cruciate ligament. Knee Surg Sports Traumatol
Arthrosc 15:453460
194. Yu B, Garrett WE (2007) Mechanisms of non-contact ACL
injuries. Br J Sports Med 41(Suppl 1):i47i51
195. Yu B, Lin CF, Garrett WE (2006) Lower extremity biome-
chanics during the landing of a stop-jump task. Clin Biomech
(Bristol, Avon) 21:297305
196. Yu B, McClure SB, Onate JA, Guskiewicz KM, Kirkendall DT,
Garrett WE (2005) Age and gender effects on lower extremity
kinematics of youth soccer players in a stop-jump task. Am J
Sports Med 33:13561364
197. Yu WD, Liu SH, Hatch JD, Panossian V, Finerman GA (1999)
Effect of estrogen on cellular metabolism of the human anterior
cruciate ligament. Clin Orthop Rel Res 366:229238
198. Yu WD, Panossian V, Hatch JD, Liu SH, Finerman GA (2001)
Combined effects of estrogen and progesterone on the anterior
cruciate ligament. Clin Orthop Rel Res 383:268281
199. Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J
(2007) Decits in neuromuscular control of the trunk predict
knee injury risk: a prospective biomechanical-epidemiologic
study. Am J Sports Med 35:11231130
200. Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J
(2007) The effects of core proprioception on knee injury: a
prospective biomechanical-epidemiological study. Am J Sports
Med 35:368373
201. Zazulak BT, Paterno M, Myer GD, Romani WA, Hewett TE
(2006) The effects of menstrual cycle on anterior knee laxity. A
systematic review. Sports Med 36:847862
202. Zazulak BT, Ponce PL, Straub SJ, Medvecky MJ, Avedisian L,
Hewett TE (2005) Gender comparison of hip muscle activity
during single leg landing. J Orthop Sports Phys Ther 35:292
299
203. Zernicke RF, Garhammer J, Jobe FW (1977) Human patellar-
tendon rupture. J Bone Joint Surg Am 59:179183
204. Zheng N, Fleisig GS, Escamilla RF, Barrentine SW (1998) An
analytical model of the knee for estimation of internal forces
during exercise. J Biomech 31:963967
Knee Surg Sports Traumatol Arthrosc (2009) 17:705729 729
1 3
You might also like
- Anterior Cruciate Ligament InjuryDocument16 pagesAnterior Cruciate Ligament InjuryEolia EffendiNo ratings yet
- Hewett2006 PDFDocument13 pagesHewett2006 PDFhectorNo ratings yet
- Mechanisms, Prediction, and Prevention of ACL Injuries - Cut Risk With Three Sharpened and Validated ToolsDocument13 pagesMechanisms, Prediction, and Prevention of ACL Injuries - Cut Risk With Three Sharpened and Validated ToolsMaKayla Leigh CrosbyNo ratings yet
- Anterior Cruciate Ligament InjuryDocument20 pagesAnterior Cruciate Ligament Injurymnunezh2304No ratings yet
- Anterior Cruciate Ligament Injuries in Soccer Players:: Amit Bandyopadhyay and Shazlin ShaharudinDocument15 pagesAnterior Cruciate Ligament Injuries in Soccer Players:: Amit Bandyopadhyay and Shazlin ShaharudinmanhuiyNo ratings yet
- ACL Injuries in The Female Athlete: Causes, Impacts, and Conditioning Programs Frank R. Noyes Sue Barber-WestinDocument658 pagesACL Injuries in The Female Athlete: Causes, Impacts, and Conditioning Programs Frank R. Noyes Sue Barber-WestinluizamgoNo ratings yet
- Dr. HumaryantoDocument6 pagesDr. HumaryantoLili SuryaniNo ratings yet
- Valgus Knee Motion During Landing in High School Female and Male Basketball PlayersDocument6 pagesValgus Knee Motion During Landing in High School Female and Male Basketball Playersok okNo ratings yet
- Perspectives On Modern OrthopaedicsDocument10 pagesPerspectives On Modern OrthopaedicsIonela ArusteiNo ratings yet
- ACL Case StudyDocument14 pagesACL Case StudyKate Crizia VillafuerteNo ratings yet
- 1 s2.0 S2095254612000452 Main PDFDocument10 pages1 s2.0 S2095254612000452 Main PDFanettepardedeNo ratings yet
- s40279 022 01697 WDocument21 pagess40279 022 01697 WBima GoodsNo ratings yet
- International Journal of Chemtech Research: Nabil .A. Mohamed and Maha. M. MohamedDocument11 pagesInternational Journal of Chemtech Research: Nabil .A. Mohamed and Maha. M. MohamedHari25885No ratings yet
- Epidemiology of Patella Instability Injuries in Collegiate Level Athletes in The United StatesDocument19 pagesEpidemiology of Patella Instability Injuries in Collegiate Level Athletes in The United StatesAthenaeum Scientific PublishersNo ratings yet
- ACL Injury: Everything You Need to Know to Make the Right Treatment Decision: - What the ACL does and why it is so important - Treatment options for partial and complete ACL tears - Surgery: graft options, how it is done, what to expect - How to prepare for surgery - What to dFrom EverandACL Injury: Everything You Need to Know to Make the Right Treatment Decision: - What the ACL does and why it is so important - Treatment options for partial and complete ACL tears - Surgery: graft options, how it is done, what to expect - How to prepare for surgery - What to dNo ratings yet
- The Effect of A Sports Chiropractic ManualDocument11 pagesThe Effect of A Sports Chiropractic ManualAli DptNo ratings yet
- Surgery Literaturr Review Anterior Cruciate Ligament RuptureDocument23 pagesSurgery Literaturr Review Anterior Cruciate Ligament RupturedayitaNo ratings yet
- 3-Women Athletes Knee Injuries - 2005Document9 pages3-Women Athletes Knee Injuries - 2005Fernanda CarvalhoNo ratings yet
- Rotura de Ligamento Cruzado Anterior en La Mujer Deportista PDFDocument5 pagesRotura de Ligamento Cruzado Anterior en La Mujer Deportista PDFCarlos Andres Valencia RenteriaNo ratings yet
- 5854 12393 1 SMDocument6 pages5854 12393 1 SMalaa adienNo ratings yet
- What's New in Sports Medicine (Primary Care) - UpToDateDocument8 pagesWhat's New in Sports Medicine (Primary Care) - UpToDateManuel OpazoNo ratings yet
- Return to Play After Ankle Sprains and SurgeryDocument13 pagesReturn to Play After Ankle Sprains and SurgeryNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- ACL Injuries in Female Athletes PowerpointDocument8 pagesACL Injuries in Female Athletes Powerpointrupinder24No ratings yet
- Ni HmsDocument40 pagesNi HmsDiah PramuditaNo ratings yet
- 10.1007@s00167 010 1170 9Document9 pages10.1007@s00167 010 1170 9Veronica LopezNo ratings yet
- Article p189 With Cover Page v2Document7 pagesArticle p189 With Cover Page v2Băiceanu AlinNo ratings yet
- Evidence Based Concepts For Prevention of Knee and ACL Injuries. 2017 Guidelines of The Ligament Committee of The German Knee Society (DKG)Document11 pagesEvidence Based Concepts For Prevention of Knee and ACL Injuries. 2017 Guidelines of The Ligament Committee of The German Knee Society (DKG)lipemagalhaesNo ratings yet
- Assessing The Effectiveness of Neuromuscular Training Programs in Reducing The Incidence of Anterior Cruciate Ligament Injuries in Female AthletesDocument9 pagesAssessing The Effectiveness of Neuromuscular Training Programs in Reducing The Incidence of Anterior Cruciate Ligament Injuries in Female AthletesCamila GuevaraNo ratings yet
- Acl Injury Research PaperDocument6 pagesAcl Injury Research Paperrvpchmrhf100% (1)
- ACL Injury and RehabilitationDocument7 pagesACL Injury and RehabilitationPaula BautistaNo ratings yet
- Female Athletes Acl InjuryDocument5 pagesFemale Athletes Acl Injuryapi-383362997No ratings yet
- 2021 Perfil de riesgo clínico para una segunda lesión del ligamento cruzado anterior en jugadoras de fútbol después de la reconstrucción del ligamento cruzado anterior.Document31 pages2021 Perfil de riesgo clínico para una segunda lesión del ligamento cruzado anterior en jugadoras de fútbol después de la reconstrucción del ligamento cruzado anterior.contact.movementsiteNo ratings yet
- Women AclDocument8 pagesWomen AclIra AdventiaNo ratings yet
- Basketball Injuries - Definition and AnatomyDocument3 pagesBasketball Injuries - Definition and AnatomysinghmenkaNo ratings yet
- Ijerph 19 13716 v2Document11 pagesIjerph 19 13716 v2allfit.davidNo ratings yet
- Dynamic Taping Improves Landing Biomechanics in YoungDocument12 pagesDynamic Taping Improves Landing Biomechanics in YoungArthur CalegariNo ratings yet
- IOC World Conference On Prevention of Injury & Illness in Sport Grimaldi Forum Monaco, Monte Carlo, Monaco 7-9 April 2011Document4 pagesIOC World Conference On Prevention of Injury & Illness in Sport Grimaldi Forum Monaco, Monte Carlo, Monaco 7-9 April 2011Christian ThamNo ratings yet
- Prevention Program in Anterior Cruciate Ligament (ACL) Among Indonesian's Athletes - Reviewed 202209122Document17 pagesPrevention Program in Anterior Cruciate Ligament (ACL) Among Indonesian's Athletes - Reviewed 202209122dewa aryNo ratings yet
- 2004, Vol.23, Issues 1, Athletic Foot and Ankle InjuriesDocument165 pages2004, Vol.23, Issues 1, Athletic Foot and Ankle InjuriesAndrei Gianina100% (3)
- Handball CMJDocument6 pagesHandball CMJBubela AlexandraNo ratings yet
- Prevention of Lateral Ankle SprainsDocument12 pagesPrevention of Lateral Ankle SprainsMarcus EstradaNo ratings yet
- Isquiotibiales TestDocument6 pagesIsquiotibiales TestHugo TintiNo ratings yet
- Upper Extremity Injuries in The National Football League: Part II: Elbow, Forearm, and Wrist InjuriesDocument8 pagesUpper Extremity Injuries in The National Football League: Part II: Elbow, Forearm, and Wrist InjuriesMaddy WolsmenNo ratings yet
- 1 s2.0 S0960077922012589 MainDocument11 pages1 s2.0 S0960077922012589 MainYẾN TRẦN NGỌCNo ratings yet
- Overview of Running Injuries of The Lower ExtremityDocument47 pagesOverview of Running Injuries of The Lower ExtremityGuardito PequeñoNo ratings yet
- Shoulder InjuriesDocument8 pagesShoulder InjurieswernsickleNo ratings yet
- Maria Luisa Dias EstrigaDocument332 pagesMaria Luisa Dias EstrigaKoordinacijska Lestev Speed LadderNo ratings yet
- Biomechanics and Injury in Volleyball ThesisDocument96 pagesBiomechanics and Injury in Volleyball ThesisDanonino12No ratings yet
- Foot and Ankle Stress Fractures in Athletes: Michael C. GreaserDocument14 pagesFoot and Ankle Stress Fractures in Athletes: Michael C. GreaserJamaluddin HaikhahNo ratings yet
- 2020 Hacer que el fútbol sea más seguro para las mujeres.Document12 pages2020 Hacer que el fútbol sea más seguro para las mujeres.contact.movementsiteNo ratings yet
- 2016 Baseline Time to StabilizationDocument5 pages2016 Baseline Time to Stabilizationktan.lboroNo ratings yet
- Evaluation, Management, Rehabilitation, and Prevention of Anterior Cruciate Ligament Injury: Current ConceptsDocument10 pagesEvaluation, Management, Rehabilitation, and Prevention of Anterior Cruciate Ligament Injury: Current ConceptsMónica Alejandra Grimaldo MuñozNo ratings yet
- Understanding and Preventing Acl Injuries: Current Biomechanical and Epidemiologic Considerations - Update 2010Document18 pagesUnderstanding and Preventing Acl Injuries: Current Biomechanical and Epidemiologic Considerations - Update 2010masonNo ratings yet
- Cartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesFrom EverandCartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesAaron J. KrychNo ratings yet
- Updateonanterior Cruciateligamentrupture AndcareinthefemaleathleteDocument13 pagesUpdateonanterior Cruciateligamentrupture AndcareinthefemaleathleteKata MoraNo ratings yet
- Canadian Academy of Sport and Exercise Medicine.11Document5 pagesCanadian Academy of Sport and Exercise Medicine.11Diego PonceNo ratings yet
- Research Paper On Football InjuriesDocument5 pagesResearch Paper On Football Injuriesafednabte100% (1)
- Relationship of Movement Screens With PastDocument7 pagesRelationship of Movement Screens With PastYoh ChenNo ratings yet
- Foot and Ankle ArthrokinematicsDocument6 pagesFoot and Ankle ArthrokinematicsCraig StewartNo ratings yet
- NSCA - Relationship Between Core Stability Functional Movement and PerformanceDocument10 pagesNSCA - Relationship Between Core Stability Functional Movement and PerformanceCraig StewartNo ratings yet
- Post Game Recovery Strategies PDFDocument4 pagesPost Game Recovery Strategies PDFCraig StewartNo ratings yet
- Effects of Active RecoveryDocument70 pagesEffects of Active RecoveryCraig StewartNo ratings yet
- Effects of Dietry Composition On Insulin Action and Energy MetabolismDocument3 pagesEffects of Dietry Composition On Insulin Action and Energy MetabolismCraig StewartNo ratings yet
- Act 342 Prevention and Control of Infectious Diseases Act 1988Document26 pagesAct 342 Prevention and Control of Infectious Diseases Act 1988Adam Haida & Co100% (1)
- A New Drug-Shelf Arrangement For Reducing MedicatiDocument9 pagesA New Drug-Shelf Arrangement For Reducing MedicatiEmmanuel LawerNo ratings yet
- Mal UnionDocument10 pagesMal UnionYehuda Agus SantosoNo ratings yet
- Biochemistry For Anesthesiologists and IntensivistsDocument11 pagesBiochemistry For Anesthesiologists and IntensivistsAndi tenri sanda datuNo ratings yet
- Drug-Induced Taste Disorders: A Primer for ToxicologistsDocument10 pagesDrug-Induced Taste Disorders: A Primer for ToxicologistsBharat NarumanchiNo ratings yet
- Bagian AwalDocument17 pagesBagian AwalCitra Monalisa LaoliNo ratings yet
- Pancreas: Anatomy, Histology, Physiology and FunctionsDocument85 pagesPancreas: Anatomy, Histology, Physiology and Functionslungu eduardNo ratings yet
- Hipraviar ClonDocument2 pagesHipraviar Clonst_richard04100% (2)
- How I Do CMR Scanning Safely: Elisabeth Burman Research Sister Royal Brompton Hospital, London UKDocument41 pagesHow I Do CMR Scanning Safely: Elisabeth Burman Research Sister Royal Brompton Hospital, London UKYuda FhunkshyangNo ratings yet
- Chapter 6 DiscussionDocument3 pagesChapter 6 DiscussionyughaNo ratings yet
- Nutrients: Obesity and Dyslipidemia in South AsiansDocument26 pagesNutrients: Obesity and Dyslipidemia in South AsiansFitriNo ratings yet
- Tender No 38 S Haad PT 2014Document26 pagesTender No 38 S Haad PT 2014Sundar Ramasamy100% (1)
- Safe AnalgesicsDocument3 pagesSafe AnalgesicsJohn SolisNo ratings yet
- 74 Manila Pest Control Vs WCCDocument4 pages74 Manila Pest Control Vs WCCharryNo ratings yet
- Tilapia 4Document69 pagesTilapia 4Annisa MeilaniNo ratings yet
- AsepsisDocument6 pagesAsepsisMarcus, RN100% (5)
- TH THDocument11 pagesTH THFista Divi AmesiaNo ratings yet
- DR, OR, WardDocument14 pagesDR, OR, WardjanNo ratings yet
- Mar ChecklistDocument18 pagesMar ChecklistMin MawNo ratings yet
- Fundamentals of Tooth Preparation Periodontal AspectsDocument74 pagesFundamentals of Tooth Preparation Periodontal AspectsVica Vitu100% (3)
- Study of Effects of Antibiotics On Micro-OrganismsDocument11 pagesStudy of Effects of Antibiotics On Micro-OrganismsSAGAR DAS79% (14)
- Effects of Pulmonary Rehabilitation On Physiologic and Psychosocial Outcomes in Patients With Chronic Obstructive Pulmonary DiseaseDocument10 pagesEffects of Pulmonary Rehabilitation On Physiologic and Psychosocial Outcomes in Patients With Chronic Obstructive Pulmonary DiseaseElita Urrutia CarrilloNo ratings yet
- Clinical Evoked PotentialsDocument13 pagesClinical Evoked PotentialsHerminaElenaNo ratings yet
- JC Oncology55211005Document32 pagesJC Oncology55211005Neenuch ManeenuchNo ratings yet
- JC 7Document20 pagesJC 7Alexander S. Garcia Jr.No ratings yet
- Canadian Standards For Hospital LibrariesDocument4 pagesCanadian Standards For Hospital LibrariesFernando HernandezNo ratings yet
- Textbook of Clinical Occupational and Environmental MedicineDocument4 pagesTextbook of Clinical Occupational and Environmental MedicineAmos SiraitNo ratings yet
- Presentation - Oral Controlled Release DrugDocument38 pagesPresentation - Oral Controlled Release DrugMrValentynNo ratings yet
- Quick Guide to Bandaging TechniquesDocument4 pagesQuick Guide to Bandaging TechniquesTheodore GonzaloNo ratings yet
- MedAspectsBio PDFDocument633 pagesMedAspectsBio PDFDuy PhúcNo ratings yet