You might also like
- CSSD SupervisorDocument6 pagesCSSD SupervisorNuman KhanNo ratings yet
- CSSD CPT ManualDocument3 pagesCSSD CPT Manualthirsal2003No ratings yet
- Central Sterile Supply Department: Mallikarjuna MHADocument25 pagesCentral Sterile Supply Department: Mallikarjuna MHAsandhyakrishnanNo ratings yet
- Chemicals Used For Cleaning & Manual Cleaning Processes - FINAL 2Document45 pagesChemicals Used For Cleaning & Manual Cleaning Processes - FINAL 2jerimiah_manzonNo ratings yet
- Disinfection vs Sterilization: A Comparison of Key AspectsDocument33 pagesDisinfection vs Sterilization: A Comparison of Key AspectsFitri AnggraeniNo ratings yet
- CSSDDocument32 pagesCSSDRAHUL100% (1)
- Alcohol Hand Disinfectant is the Best Way to Prevent Healthcare Associated InfectionsDocument64 pagesAlcohol Hand Disinfectant is the Best Way to Prevent Healthcare Associated Infectionsdanang setiawanNo ratings yet
- Central Sterile Supply Services Policy KKM PDFDocument53 pagesCentral Sterile Supply Services Policy KKM PDFGerald TalledoNo ratings yet
- Medical Waste ManagementDocument50 pagesMedical Waste ManagementNisa ShiningNo ratings yet
- Theatre Infection Control Policy 2005Document15 pagesTheatre Infection Control Policy 2005parthotissNo ratings yet
- Troubleshooting Instrument StainsDocument4 pagesTroubleshooting Instrument Stainsjerimiah_manzonNo ratings yet
- Aseptic TechniqueDocument9 pagesAseptic Techniquebethh_6No ratings yet
- Supplies & Consumables in CSSDDocument119 pagesSupplies & Consumables in CSSDjerimiah_manzonNo ratings yet
- Surabaya - PPI RSDS - Infection Control in CSSDDocument55 pagesSurabaya - PPI RSDS - Infection Control in CSSDboerhan2504No ratings yet
- Deconex PROZYME ALKA EN PDFDocument4 pagesDeconex PROZYME ALKA EN PDFMauli DjistarNo ratings yet
- Hospital HygieneDocument29 pagesHospital HygieneManoj Sankaranarayana0% (1)
- Cis Self-Study Lesson Plan: Vascular and Cardiovascular Surgical InstrumentsDocument4 pagesCis Self-Study Lesson Plan: Vascular and Cardiovascular Surgical Instrumentsjerimiah_manzonNo ratings yet
- CSSD - Sep 1st 2016 Final 3 in 1-1Document16 pagesCSSD - Sep 1st 2016 Final 3 in 1-1SundaraBharathiNo ratings yet
- EtO-MD Sterilization and Autoclave Sterilization Complement Each OtherDocument3 pagesEtO-MD Sterilization and Autoclave Sterilization Complement Each OtherVer BautistaNo ratings yet
- ASEPSISDocument28 pagesASEPSISDeborah AmpongNo ratings yet
- Hemodialysis Central Venous Catheter STH ProtocolDocument2 pagesHemodialysis Central Venous Catheter STH ProtocolNor HilaliahNo ratings yet
- JNJ - SSI - Instrument Reprocessing, 2019 PDFDocument76 pagesJNJ - SSI - Instrument Reprocessing, 2019 PDFDEBBYNo ratings yet
- Presentation 1 Environmental CleaningDocument33 pagesPresentation 1 Environmental CleaningAfeefa Amin AliNo ratings yet
- Ot PDFDocument27 pagesOt PDFZain ShariffNo ratings yet
- Sterilization of Operation Theatres - Time To Stop FumigationDocument2 pagesSterilization of Operation Theatres - Time To Stop Fumigationtummalapalli venkateswara rao100% (1)
- 2020 4 - Principles-of-Sterilization-and-DisinfectionDocument41 pages2020 4 - Principles-of-Sterilization-and-DisinfectionMely Kartikasari100% (1)
- Central Sterile Supply DepartmentDocument25 pagesCentral Sterile Supply DepartmentRevati shindeNo ratings yet
- SE - Sterilization of Medical Devices - 1Document77 pagesSE - Sterilization of Medical Devices - 1Jothi Vel Murugan100% (1)
- Operation Theater ManagementDocument8 pagesOperation Theater ManagementAshish SinghNo ratings yet
- Process Failures HO RoseDocument14 pagesProcess Failures HO RoseHilario AlinabonNo ratings yet
- Decontamination and sterilization methodsDocument36 pagesDecontamination and sterilization methodsHarshinie AudimulamNo ratings yet
- Biomedical Waste Management - A Review: P. V. Deshmukh R. H. RathodDocument5 pagesBiomedical Waste Management - A Review: P. V. Deshmukh R. H. RathodEditor IJRITCCNo ratings yet
- Operating Theater ManagementDocument5 pagesOperating Theater Managementtummalapalli venkateswara raoNo ratings yet
- CRCST Self-Study Lesson PlanDocument4 pagesCRCST Self-Study Lesson Planjerimiah_manzonNo ratings yet
- Definition of CSSD - Central Sterile Supply DepartmentDocument3 pagesDefinition of CSSD - Central Sterile Supply DepartmentRevati shindeNo ratings yet
- Final HICC Manual AIIMSDocument35 pagesFinal HICC Manual AIIMSNaMakNo ratings yet
- Cleaning, Sterilization and Disinfection PrinciplesDocument99 pagesCleaning, Sterilization and Disinfection PrinciplesJyotiNo ratings yet
- 2013 - BestPractices For HLDDocument53 pages2013 - BestPractices For HLDDaniela Cirnatu100% (1)
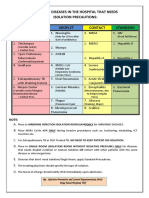
- Common Hospital Diseases Requiring Isolation PrecautionsDocument1 pageCommon Hospital Diseases Requiring Isolation Precautionsjerimiah_manzonNo ratings yet
- CSSDDocument18 pagesCSSDMehak KapoorNo ratings yet
- Medinews 4 For PrintDocument35 pagesMedinews 4 For PrintDr Subhashish DasNo ratings yet
- 10562997Document81 pages10562997Ppa Gpat AmitNo ratings yet
- Legal Aspects in HospitalDocument32 pagesLegal Aspects in HospitalDr. Rakshit Solanki0% (1)
- Steam SterilizationDocument2 pagesSteam SterilizationHumayun KhanNo ratings yet
- Universal Precaution by FithriDocument62 pagesUniversal Precaution by FithriFithriKurniatiNo ratings yet
- Clinical Microbiology Laboratory Test RequisitionDocument1 pageClinical Microbiology Laboratory Test RequisitionRhodjane Dela Cruz0% (1)
- c40402 Sterile ContainerAESCULAPDocument108 pagesc40402 Sterile ContainerAESCULAPIfan RizkyNo ratings yet
- General Chapters - 1035 - Biological Indicators For SterilizationDocument6 pagesGeneral Chapters - 1035 - Biological Indicators For SterilizationKoeys KuswandaNo ratings yet
- AORN's Guide to Cleaning Surgical Instruments and EquipmentDocument46 pagesAORN's Guide to Cleaning Surgical Instruments and EquipmentRex Lagunzad FloresNo ratings yet
- Cis Self-Study Lesson Plan: Care and Handling of Sharp InstrumentsDocument4 pagesCis Self-Study Lesson Plan: Care and Handling of Sharp Instrumentsjerimiah_manzonNo ratings yet
- CSSDDocument35 pagesCSSDAzmi Tok-tokNo ratings yet
- 3 Bio-Medical Waste ManagementDocument69 pages3 Bio-Medical Waste ManagementHarshaWakodkarNo ratings yet
- Sterilization & Disinfection: Allison Mcgeer, MSC, MD, FRCPCDocument53 pagesSterilization & Disinfection: Allison Mcgeer, MSC, MD, FRCPCFrancescca Cynthya A. Vargas RosasNo ratings yet
- Open Gloving: Dahlia A. Bisnar RN, MN, RMDocument20 pagesOpen Gloving: Dahlia A. Bisnar RN, MN, RMClarabal, Sharly Quin A.No ratings yet
- CSSDDocument25 pagesCSSDbalachanderNo ratings yet
- Sterilization TechniquesDocument4 pagesSterilization TechniquesA.JeevarathinamNo ratings yet
- Cystoscope cleaning stepsDocument5 pagesCystoscope cleaning stepsjerimiah_manzonNo ratings yet
- Handbook for Cssd Technicians: Understanding the Basics - Second EditionFrom EverandHandbook for Cssd Technicians: Understanding the Basics - Second EditionNo ratings yet
- 9 Disinfectant, Antiseptic & SterilizationDocument21 pages9 Disinfectant, Antiseptic & SterilizationShatha Al-RamahiNo ratings yet
- Blood Transfusion Guidelines PDFDocument21 pagesBlood Transfusion Guidelines PDFEmhemed Amer Tabib100% (2)
- Skema Sains k1&k2 SPM TRG 2017Document9 pagesSkema Sains k1&k2 SPM TRG 2017zahisma89No ratings yet
- EMTS Book PDFDocument146 pagesEMTS Book PDFWan Nurul Amiera100% (1)
- Guidelines on Aesthetic Medical PracticeDocument47 pagesGuidelines on Aesthetic Medical Practicezahisma890% (1)
- Anesthesia GuideDocument84 pagesAnesthesia Guidezahisma89No ratings yet
- Aseptic Wound Dressing Edited 3 Dec 2008Document11 pagesAseptic Wound Dressing Edited 3 Dec 2008zahisma89No ratings yet
- Polystyrene Fact SheetsDocument4 pagesPolystyrene Fact Sheetszahisma89No ratings yet
- STPPT1 Life Processes Interactions and AdaptationsDocument24 pagesSTPPT1 Life Processes Interactions and AdaptationsIVAN GLENN NAGALNo ratings yet
- Robein E. Velocities, Time-Imaging and Depth-Imaging Principles and Methods (60 PDFDocument462 pagesRobein E. Velocities, Time-Imaging and Depth-Imaging Principles and Methods (60 PDFleonardoNo ratings yet
- Director PR Public Affairs in Chicago IL Resume Gloria PopeDocument2 pagesDirector PR Public Affairs in Chicago IL Resume Gloria PopeGloriaPopeNo ratings yet
- Machine Learning Assignment Differences Between Linear And Logistic RegressionDocument4 pagesMachine Learning Assignment Differences Between Linear And Logistic Regressionbharti goyalNo ratings yet
- Test Study On The Fatigue Performance of HSS For Steel WheelsDocument4 pagesTest Study On The Fatigue Performance of HSS For Steel WheelsdamlaNo ratings yet
- 100 Song ChallengeDocument3 pages100 Song ChallengeChristina KnightsNo ratings yet
- Producer and Actor Mutual AgreementDocument3 pagesProducer and Actor Mutual AgreementKrishNo ratings yet
- Manok Mabuhay (FINAL PAIR CASE)Document12 pagesManok Mabuhay (FINAL PAIR CASE)Eldon CalambaNo ratings yet
- Part Test - 3 (Senior) Question Paper 2011-P1 8-6-2020-FDocument15 pagesPart Test - 3 (Senior) Question Paper 2011-P1 8-6-2020-FJainNo ratings yet
- Palladam Hi-Tech Weaving Park Gateway Global MarketDocument26 pagesPalladam Hi-Tech Weaving Park Gateway Global MarketKrishna PrasadNo ratings yet
- Product Data 38au-02pd Condensadora 6 - 30 TonsDocument52 pagesProduct Data 38au-02pd Condensadora 6 - 30 TonsPatricio LescanoNo ratings yet
- The Kurt Rosenwinkel Forum (Chords)Document7 pagesThe Kurt Rosenwinkel Forum (Chords)thrashtilldeath100% (1)
- HarnWorld d20 - Harn GuideDocument44 pagesHarnWorld d20 - Harn GuideJamesBirmingham100% (1)
- Audio Lingual MethodDocument12 pagesAudio Lingual MethodKeviin Mariño VivasNo ratings yet
- MVix ManualDocument102 pagesMVix Manualspyros_peiraiasNo ratings yet
- Derivatives Commodity Derivatives FGLD EnglishDocument13 pagesDerivatives Commodity Derivatives FGLD EnglishrexNo ratings yet
- Math 121 Fall 17 Final TopicsDocument2 pagesMath 121 Fall 17 Final TopicsJillNo ratings yet
- CV For UnescoDocument6 pagesCV For UnescoArpan BhujuNo ratings yet
- Verbal and Non-VerbalDocument26 pagesVerbal and Non-VerbalDanica ValentinoNo ratings yet
- Mary Slessor of Calabar: Pioneer Missionary by Livingstone, W. P.Document231 pagesMary Slessor of Calabar: Pioneer Missionary by Livingstone, W. P.Gutenberg.orgNo ratings yet
- Diya CopDocument26 pagesDiya CopDebojit Koley DCE 8852No ratings yet
- 2nd Quarter 2nd Summative Oral CommunicationDocument2 pages2nd Quarter 2nd Summative Oral CommunicationArthur TalomaNo ratings yet
- Factors Affecting Chemical Reaction RatesDocument2 pagesFactors Affecting Chemical Reaction RatesLuis WashingtonNo ratings yet
- Plant Disease DetectionDocument3 pagesPlant Disease Detectionabdul kareemNo ratings yet
- Siddha Medicines For Bronchial AsthmaDocument9 pagesSiddha Medicines For Bronchial AsthmasalemraghuNo ratings yet
- Subject + Was/were/v II + Object/ComplementDocument6 pagesSubject + Was/were/v II + Object/ComplementRini TiaraNo ratings yet
- Ultrasonic CleaningDocument9 pagesUltrasonic Cleaningfgdgrte gdfsgdNo ratings yet
- Great Britain: Numbers Issued 1840 To 1910Document42 pagesGreat Britain: Numbers Issued 1840 To 1910Ahmed Mohamed Badawy50% (2)
- Dilg Memocircular 2023119 - Ca3d912db2Document76 pagesDilg Memocircular 2023119 - Ca3d912db2Korlissemina RascoNo ratings yet
- Greater Doha Bus Services: Al Ghanim Bus StationDocument1 pageGreater Doha Bus Services: Al Ghanim Bus Stationramadan rashadNo ratings yet