You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Trust Deed For Establishment of A TempleDocument2 pagesTrust Deed For Establishment of A TemplePoorna Nanda88% (17)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
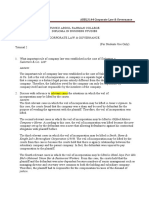
- Tutorial 2Document3 pagesTutorial 2猪mongNo ratings yet
- PNB Liable for Damages Due to Disapproval of Sugar Quota LeaseDocument1 pagePNB Liable for Damages Due to Disapproval of Sugar Quota LeaseErnie GultianoNo ratings yet
- Trabajo Final Académico-Ingles-Ramirez Lopez Camila PDFDocument110 pagesTrabajo Final Académico-Ingles-Ramirez Lopez Camila PDFcamilaNo ratings yet
- Service Returned ServedDocument2 pagesService Returned ServedLeTaia DuncanNo ratings yet
- Kosha Investments LTD Vs Securities & Exchange BD of India & ... On 18 September, 2015Document5 pagesKosha Investments LTD Vs Securities & Exchange BD of India & ... On 18 September, 2015sreevarshaNo ratings yet
- Charlotte Keeley Misconduct Sacramento Superior Court: Unlawful Proof of Service - Sacramento County Judge Robert Hight - Judge James Mize - US District Court Eastern District of California - 3rd District Court of Appeal Judge Vance Raye - California Supreme Court Tani Cantil SakauyeDocument10 pagesCharlotte Keeley Misconduct Sacramento Superior Court: Unlawful Proof of Service - Sacramento County Judge Robert Hight - Judge James Mize - US District Court Eastern District of California - 3rd District Court of Appeal Judge Vance Raye - California Supreme Court Tani Cantil SakauyeCalifornia Judicial Branch News Service - Investigative Reporting Source Material & Story Ideas100% (1)
- GNLU Course Outline for Law of TortsDocument24 pagesGNLU Course Outline for Law of TortsMayank AameriaNo ratings yet
- Law of Contract: ConsiderationDocument19 pagesLaw of Contract: ConsiderationJacob Black100% (1)
- United States v. Joell Joyce, 4th Cir. (2012)Document4 pagesUnited States v. Joell Joyce, 4th Cir. (2012)Scribd Government DocsNo ratings yet
- Eduardo F Hernandez Et Al Vs National Power CorporationDocument12 pagesEduardo F Hernandez Et Al Vs National Power CorporationMariel D. PortilloNo ratings yet
- 881 Legal Studies - Isc SpecimenDocument17 pages881 Legal Studies - Isc SpecimenLion HogwartsNo ratings yet
- Jurisdiction of The RTCDocument26 pagesJurisdiction of The RTCMacNo ratings yet
- DynCorps' Answer To Original ComplaintDocument12 pagesDynCorps' Answer To Original ComplaintDallasObserverNo ratings yet
- PCL Shipping Phils Vs NLRC, 511 SCRA 44Document9 pagesPCL Shipping Phils Vs NLRC, 511 SCRA 44Ric SaysonNo ratings yet
- Ochoa Vs G.S. TransportDocument5 pagesOchoa Vs G.S. Transportkatherine magbanuaNo ratings yet
- Regional Trial Court: ORTIZ Sa Iya Opisina Nga Nahamtang Sa 2Document5 pagesRegional Trial Court: ORTIZ Sa Iya Opisina Nga Nahamtang Sa 2April Laurence Ortiz100% (1)
- PEOPLE'S TRANS-EAST ASIA INSURANCE CORPORATION, A.K.A. PEOPLE'S GENERAL INSURANCE CORPORATION v. DOCTORS OF NEW MILLENNIUM HOLDINGS, INCDocument11 pagesPEOPLE'S TRANS-EAST ASIA INSURANCE CORPORATION, A.K.A. PEOPLE'S GENERAL INSURANCE CORPORATION v. DOCTORS OF NEW MILLENNIUM HOLDINGS, INCRA BautistaNo ratings yet
- Land Trespass LawDocument5 pagesLand Trespass LawKartik BhargavaNo ratings yet
- Janux Transcript 10cDocument2 pagesJanux Transcript 10cWright SomesNo ratings yet
- Battle Sports Science v. Shock Doctor - ComplaintDocument53 pagesBattle Sports Science v. Shock Doctor - ComplaintSarah BursteinNo ratings yet
- Supreme Court petition reconsiderationDocument3 pagesSupreme Court petition reconsiderationHans ChavezNo ratings yet
- Proxy FormDocument3 pagesProxy FormAbegail Protacio GuardianNo ratings yet
- Mutual Termination and Release AgreementDocument5 pagesMutual Termination and Release AgreementMohamed El AbanyNo ratings yet
- Supreme Court dismisses petitions challenging declaration of state of rebellionDocument3 pagesSupreme Court dismisses petitions challenging declaration of state of rebellionFused ConsNo ratings yet
- CJS On SignaturesDocument47 pagesCJS On Signaturesgoldilucks100% (2)
- United States v. Roland Lee Stout, 434 F.2d 1264, 10th Cir. (1970)Document5 pagesUnited States v. Roland Lee Stout, 434 F.2d 1264, 10th Cir. (1970)Scribd Government DocsNo ratings yet
- IRS Frivolous Filing Penalty DismissalDocument7 pagesIRS Frivolous Filing Penalty DismissalvladaputoNo ratings yet
- Rosete vs. LimDocument4 pagesRosete vs. LimLoren MandaNo ratings yet
- Kusum Sharma Versus Mahinder Kumar SharmaDocument62 pagesKusum Sharma Versus Mahinder Kumar SharmaLive Law100% (2)