You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- 2012 AICPA Financial QuestionsDocument59 pages2012 AICPA Financial QuestionsJimsy AntuNo ratings yet
- By Emile Alline: Technical Art by Fred WolffDocument4 pagesBy Emile Alline: Technical Art by Fred WolffJim100% (3)
- CD1 ISO/IEC 17000 Conformity Assessment - Vocabulary and General PrinciplesDocument26 pagesCD1 ISO/IEC 17000 Conformity Assessment - Vocabulary and General PrinciplesMAC CONSULTORESNo ratings yet
- Tailwind OperationsDocument3 pagesTailwind Operationsiceman737No ratings yet
- Crafting and Executing StrategyDocument33 pagesCrafting and Executing Strategyamoore2505No ratings yet
- Siart, Et. Al (2018) Digital GeoarchaeologyDocument272 pagesSiart, Et. Al (2018) Digital GeoarchaeologyPepe100% (2)
- Production of Formaldehyde From MethanolDocument200 pagesProduction of Formaldehyde From MethanolSofia Mermingi100% (1)
- Correlation Between Polymerization Stress and Interfacial Integrity of Composites Restorations Assessed by Different in Vitro TestsDocument9 pagesCorrelation Between Polymerization Stress and Interfacial Integrity of Composites Restorations Assessed by Different in Vitro TestsNeelima SonawaneNo ratings yet
- Application Form: Student SSC DetailsDocument3 pagesApplication Form: Student SSC DetailsShrikrishna BirajdarNo ratings yet
- Chocolate IndustryDocument71 pagesChocolate IndustryHem Thapar50% (8)
- Diploma New Admission FormDocument3 pagesDiploma New Admission FormNeelima SonawaneNo ratings yet
- Annual Report 2007 2008Document84 pagesAnnual Report 2007 2008Neelima SonawaneNo ratings yet
- Application DetailsDocument2 pagesApplication DetailsNeelima SonawaneNo ratings yet
- Case Study - Jamie Turner at MLI Inc.Document11 pagesCase Study - Jamie Turner at MLI Inc.Neelima Sonawane50% (2)
- MBA CET 2013-2015 Model Question Paper For Offline ExamDocument6 pagesMBA CET 2013-2015 Model Question Paper For Offline ExamNeelima SonawaneNo ratings yet
- Holacracy FinalDocument24 pagesHolacracy FinalShakil Reddy BhimavarapuNo ratings yet
- ADL MATRIX STRATEGY FOR BPCL'S GROWTHDocument17 pagesADL MATRIX STRATEGY FOR BPCL'S GROWTHSachin Nagar100% (1)
- E 74 - 06 - For Force Measuring InstrumentsDocument12 pagesE 74 - 06 - For Force Measuring InstrumentsSarvesh MishraNo ratings yet
- DrdoDocument2 pagesDrdoAvneet SinghNo ratings yet
- E Requisition SystemDocument8 pagesE Requisition SystemWaNi AbidNo ratings yet
- Critical Thinking Essay-Animal Testing: Rough DraftDocument10 pagesCritical Thinking Essay-Animal Testing: Rough Draftjeremygcap2017No ratings yet
- Quiz 1Document3 pagesQuiz 1JULIANNE BAYHONNo ratings yet
- Philippine Popular Culture in HEIsDocument9 pagesPhilippine Popular Culture in HEIsNokie TunayNo ratings yet
- 21st Century Literature Exam SpecsDocument2 pages21st Century Literature Exam SpecsRachel Anne Valois LptNo ratings yet
- Gentle Classical Nature Sample - Units1 and 2Document129 pagesGentle Classical Nature Sample - Units1 and 2Carita HemsleyNo ratings yet
- J05720020120134026Functions and GraphsDocument14 pagesJ05720020120134026Functions and GraphsmuglersaurusNo ratings yet
- Dewatering Well PointsDocument4 pagesDewatering Well Pointssalloum3No ratings yet
- 1993 - Kelvin-Helmholtz Stability Criteria For Stratfied Flow - Viscous Versus Non-Viscous (Inviscid) Approaches PDFDocument11 pages1993 - Kelvin-Helmholtz Stability Criteria For Stratfied Flow - Viscous Versus Non-Viscous (Inviscid) Approaches PDFBonnie JamesNo ratings yet
- PMMAEE Application FormDocument2 pagesPMMAEE Application Formshiero501100% (15)
- University Reserch Worksheet PDFDocument7 pagesUniversity Reserch Worksheet PDFapi-410567922No ratings yet
- Calculating Molar MassDocument5 pagesCalculating Molar MassTracy LingNo ratings yet
- HRM Assignment Final - Case StudyDocument7 pagesHRM Assignment Final - Case StudyPulkit_Bansal_2818100% (3)
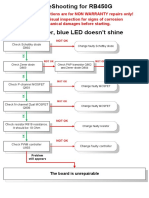
- RB450G Trouble ShootingDocument9 pagesRB450G Trouble Shootingjocimar1000No ratings yet
- GCSE H3 02g4 02 3D TrigonometryDocument2 pagesGCSE H3 02g4 02 3D TrigonometryAndrei StanescuNo ratings yet
- Catalogue: Product Offering 51Document56 pagesCatalogue: Product Offering 51Bruno MartinsNo ratings yet
- Click To Edit Master Title Style: Uggas, Heinz Gerhard A. Sabroso, Dionisio Jr. L. Reyes, Jeboy ODocument21 pagesClick To Edit Master Title Style: Uggas, Heinz Gerhard A. Sabroso, Dionisio Jr. L. Reyes, Jeboy ODionisio SabrosoNo ratings yet
- Use DCP to Predict Soil Bearing CapacityDocument11 pagesUse DCP to Predict Soil Bearing CapacitysarvaiyahimmatNo ratings yet
- Vega Plus 69Document3 pagesVega Plus 69yashNo ratings yet
- The Critical Need For Software Engineering EducationDocument5 pagesThe Critical Need For Software Engineering EducationGaurang TandonNo ratings yet