You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- BDSM Checklist ShevahDocument208 pagesBDSM Checklist Shevahslackjack86% (36)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Creepy Moments For RPGs - Part 1 - Version 1.5 PDFDocument141 pagesCreepy Moments For RPGs - Part 1 - Version 1.5 PDFBraulioCharajaVargas100% (1)
- Green Tea (Camellia Sinensis, L.) Ethanolic Extract As Hair Tonic in Nutraceutical: Physical Stability, Hair Growth Activity On Rats, and Safety TestDocument6 pagesGreen Tea (Camellia Sinensis, L.) Ethanolic Extract As Hair Tonic in Nutraceutical: Physical Stability, Hair Growth Activity On Rats, and Safety TestDyah Putri Ayu DinastyarNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- 16 Stroke SyndromesDocument32 pages16 Stroke SyndromesRos Potter100% (2)
- How To Make Hair ShampoosDocument1 pageHow To Make Hair Shampoospakde jongkoNo ratings yet
- Cambridge Food HygieneDocument22 pagesCambridge Food Hygieneapi-350003268No ratings yet
- Halal Critical Point of Foods and Beverages - REV-1Document44 pagesHalal Critical Point of Foods and Beverages - REV-1Dyah Putri Ayu DinastyarNo ratings yet
- The Treatment of Dandruff of The Scalp: Harmacology CosmetologDocument8 pagesThe Treatment of Dandruff of The Scalp: Harmacology CosmetologDyah Putri Ayu DinastyarNo ratings yet
- Emergency and Disaster NursingDocument13 pagesEmergency and Disaster Nursingkarenkaren09No ratings yet
- Bhalaaji - Art and Science of Orthodontics WordDocument578 pagesBhalaaji - Art and Science of Orthodontics WordBudi AthAnza Suhartono85% (13)
- Dermatitis and HomoeopathyDocument18 pagesDermatitis and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Scaling and Root Planing Presentation - DR - Naaz GillDocument37 pagesScaling and Root Planing Presentation - DR - Naaz GillNaazGill100% (1)
- Assessment of RA 9994 implementation for senior citizensDocument12 pagesAssessment of RA 9994 implementation for senior citizenserroljohnescorial100% (1)
- Bahaya Makanan HaramDocument37 pagesBahaya Makanan HaramDyah Putri Ayu DinastyarNo ratings yet
- ContraceptionDocument42 pagesContraceptionDyah Putri Ayu DinastyarNo ratings yet
- Eng PDFDocument214 pagesEng PDFafriantoNo ratings yet
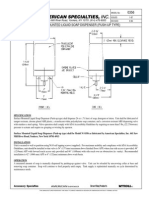
- Surface Mounted Liquid Soap Dispenser (Push-Up Type) : 441 Saw Mill River Road, Yonkers, NY 10701 (914) 476-9000Document1 pageSurface Mounted Liquid Soap Dispenser (Push-Up Type) : 441 Saw Mill River Road, Yonkers, NY 10701 (914) 476-9000Dyah Putri Ayu DinastyarNo ratings yet
- The Malassezia Genus in Skin and Systemic DiseasesDocument36 pagesThe Malassezia Genus in Skin and Systemic DiseasesDyah Putri Ayu DinastyarNo ratings yet
- Archive of SID: Riginal RticleDocument4 pagesArchive of SID: Riginal RticleDyah Putri Ayu DinastyarNo ratings yet
- Preparation of Soap Using Different Types of Oils and Exploring Its Properties PDFDocument42 pagesPreparation of Soap Using Different Types of Oils and Exploring Its Properties PDFm.cj1No ratings yet
- Coagulation DisorderDocument36 pagesCoagulation DisorderDyah Putri Ayu DinastyarNo ratings yet
- Formulation and evaluation of herbal anti-dandruff shampooDocument5 pagesFormulation and evaluation of herbal anti-dandruff shampoofaizawidiNo ratings yet
- 3162 3646 1 SMDocument7 pages3162 3646 1 SMjlekzzzNo ratings yet
- Cocamide DEADocument1 pageCocamide DEADyah Putri Ayu DinastyarNo ratings yet
- 559 PDFDocument4 pages559 PDFDyah Putri Ayu DinastyarNo ratings yet
- Ijapsbs 2.3 149-155Document7 pagesIjapsbs 2.3 149-155Dyah Putri Ayu DinastyarNo ratings yet
- Sodium Lauryl SulfateDocument9 pagesSodium Lauryl SulfateMoxzJr VianzNo ratings yet
- Hiragana Chart - ひらがな PDFDocument1 pageHiragana Chart - ひらがな PDFDoni SetiawanNo ratings yet
- Micro Manual EngDocument262 pagesMicro Manual EngEmad ManniNo ratings yet
- 106 GuptaDocument5 pages106 GuptaDyah Putri Ayu DinastyarNo ratings yet
- Formulation and evaluation of herbal anti-dandruff shampooDocument5 pagesFormulation and evaluation of herbal anti-dandruff shampoofaizawidiNo ratings yet
- Jocpr 26Document7 pagesJocpr 26sumendersinghNo ratings yet
- Katakana Chart - カタカナ PDFDocument1 pageKatakana Chart - カタカナ PDFDoni SetiawanNo ratings yet
- r600 Part 1Document36 pagesr600 Part 1Dyah Putri Ayu DinastyarNo ratings yet
- Sinesis L.) Dalam Sediaan Krim Terhadap Sifat Fisik Dan AktivitasDocument10 pagesSinesis L.) Dalam Sediaan Krim Terhadap Sifat Fisik Dan AktivitasDyah Putri Ayu DinastyarNo ratings yet
- Sen PR 0011Document12 pagesSen PR 0011Dyah Putri Ayu DinastyarNo ratings yet
- Screening For The Antimicrobial Activities of Alcoholic and Aqueous Extracts of Some Common Spices in EgyptDocument8 pagesScreening For The Antimicrobial Activities of Alcoholic and Aqueous Extracts of Some Common Spices in EgyptDyah Putri Ayu DinastyarNo ratings yet
- Formulation and Evaluation of Herbal Shampoo From: ISSN 2229-3566 Research ArticleDocument5 pagesFormulation and Evaluation of Herbal Shampoo From: ISSN 2229-3566 Research ArticleJorge Sergio CondeNo ratings yet
- In The Context of Nepal, Most of The Studies Have Identi Ed Iron de Ciency Anemia Only Based On Hemoglobin Level in The Context of Nepal, Most of The Studies Have Identi EdDocument10 pagesIn The Context of Nepal, Most of The Studies Have Identi Ed Iron de Ciency Anemia Only Based On Hemoglobin Level in The Context of Nepal, Most of The Studies Have Identi EdAshma KhulalNo ratings yet
- Our Lady of Fatima UniversityDocument5 pagesOur Lady of Fatima UniversityEmmanuel De LeonNo ratings yet
- Jipmer 2010 Rapid Review: Jawaharlal Institute of Postgraduate Medical Education & ResearchDocument15 pagesJipmer 2010 Rapid Review: Jawaharlal Institute of Postgraduate Medical Education & ResearchgokunambiarNo ratings yet
- Fundamentals of Epidemiology (EPID 610) Exercise 12 Screening Learning ObjectivesDocument4 pagesFundamentals of Epidemiology (EPID 610) Exercise 12 Screening Learning Objectiveswelcome martin100% (1)
- Investigation of Blood Culture Using BACTEC SystemsDocument36 pagesInvestigation of Blood Culture Using BACTEC SystemsGregorio De Las CasasNo ratings yet
- Hesi Hints Part 4Document2 pagesHesi Hints Part 4Sharon TanveerNo ratings yet
- Emergency drugs study guideDocument75 pagesEmergency drugs study guideQuinonez Anna MarieNo ratings yet
- 1B Cytokine Instruction Manual-10014905CDocument52 pages1B Cytokine Instruction Manual-10014905CJose EstrellaNo ratings yet
- Full HD English Editorials 2-1-2022Document25 pagesFull HD English Editorials 2-1-2022uihuyhyubuhbNo ratings yet
- Global Food Problems and SolutionsDocument21 pagesGlobal Food Problems and SolutionsMd Umar HaadNo ratings yet
- A Case Report - Ayurvedic Management of Pariplutayonivyapada W.S.R To Pelvic Inflammatory DiseaseDocument6 pagesA Case Report - Ayurvedic Management of Pariplutayonivyapada W.S.R To Pelvic Inflammatory DiseaseIJAR JOURNALNo ratings yet
- Brochure Systeme MedilogDocument8 pagesBrochure Systeme MedilogAbrourNo ratings yet
- First Aid Plan ConstructionDocument13 pagesFirst Aid Plan ConstructionUmair KhanNo ratings yet
- Prevalence of Erectile Dysfunction in Urology Consultation: A Prospective StudyDocument6 pagesPrevalence of Erectile Dysfunction in Urology Consultation: A Prospective StudyIJAR JOURNALNo ratings yet
- Potassium: Enzymatic MethodDocument2 pagesPotassium: Enzymatic MethodFariz KasyidiNo ratings yet
- Memoir ExampleDocument6 pagesMemoir Exampleapi-397214410No ratings yet
- STROKE-pathophysiology, Diagnosis, and Management, 4th EditionDocument3 pagesSTROKE-pathophysiology, Diagnosis, and Management, 4th EditionNishi RuciNo ratings yet
- Risk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriDocument14 pagesRisk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriSi PuputNo ratings yet
- Oral Myiasis PublicationDocument6 pagesOral Myiasis PublicationAnkita GoklaniNo ratings yet
- Ijmm 31 6 1375 PDFDocument6 pagesIjmm 31 6 1375 PDFAlex RogobeteNo ratings yet
- Assignment 2 Biol 1700 Fall 2020Document20 pagesAssignment 2 Biol 1700 Fall 2020api-535587985No ratings yet