You might also like
- Content: 2. Literature Survey 3. Problem Definition 4. Objective 5. Methodology 6. ReferencesDocument10 pagesContent: 2. Literature Survey 3. Problem Definition 4. Objective 5. Methodology 6. ReferencesImran ShaikhNo ratings yet
- BSP OelDocument7 pagesBSP OelAli AliNo ratings yet
- Nazmi 2015Document6 pagesNazmi 2015u5600291No ratings yet
- Electrophysiology of LarynxDocument12 pagesElectrophysiology of LarynxNehasish SahuNo ratings yet
- Electromyography: About The TestDocument3 pagesElectromyography: About The TestMicromaxHuaweiNo ratings yet
- TestsDocument8 pagesTestsNamrathaThalatoti ywSSAmHsULNo ratings yet
- EMG Signal Features Extraction of Different Arm Movement For Rehabilitation Device PDFDocument12 pagesEMG Signal Features Extraction of Different Arm Movement For Rehabilitation Device PDFulfahrifNo ratings yet
- EmgDocument6 pagesEmgDhabia AhmedNo ratings yet
- An Explanatory Study of The Parameters To Be Measured From EMG SignalDocument7 pagesAn Explanatory Study of The Parameters To Be Measured From EMG SignalNawang Wahyu WNo ratings yet
- Real-Time Muscle Fatigue Monitoring Based On Median Frequency of Electromyography SignalDocument5 pagesReal-Time Muscle Fatigue Monitoring Based On Median Frequency of Electromyography SignalMuhammad Fauzi D4 ElektromedikNo ratings yet
- Design Considerations For A Robust EMG AmplifierDocument5 pagesDesign Considerations For A Robust EMG AmplifierAlexNo ratings yet
- Electromyography I PDFDocument13 pagesElectromyography I PDFkeithtrahNo ratings yet
- EEG (ElectroEncephaloGraph)Document47 pagesEEG (ElectroEncephaloGraph)Dhvij KmlNo ratings yet
- Signal Condition and Acquisition System For A Low Cost EMG Based Prosthetic HandDocument9 pagesSignal Condition and Acquisition System For A Low Cost EMG Based Prosthetic HandNazhan HakeemNo ratings yet
- Clinical Electro Physiological TestingDocument22 pagesClinical Electro Physiological TestingPaul VkNo ratings yet
- Measurement System:: Signal Processing, ADC and Digital ProcessingDocument1 pageMeasurement System:: Signal Processing, ADC and Digital ProcessingZz_TyranT_zZNo ratings yet
- Ijbb 121 PDFDocument8 pagesIjbb 121 PDFRahma WatiNo ratings yet
- Denoising of EMG Signals Based On Wavelet Transform: N. M. SobahiDocument7 pagesDenoising of EMG Signals Based On Wavelet Transform: N. M. SobahiTher SitaNo ratings yet
- Collective Task 2 - Effects of The Electric Current. Property of The Eye.Document2 pagesCollective Task 2 - Effects of The Electric Current. Property of The Eye.ibrahimjahangir1No ratings yet
- Analise EmgDocument36 pagesAnalise EmgBruno SantosNo ratings yet
- EMG Biofeedback - The Principles: Biofeedback As A Component of TreatmentDocument4 pagesEMG Biofeedback - The Principles: Biofeedback As A Component of TreatmentFaisal Qureshi100% (1)
- Surface EMG Design PDFDocument22 pagesSurface EMG Design PDFJuan LizamaNo ratings yet
- EMG Processing SignalDocument36 pagesEMG Processing SignalafrizalNo ratings yet
- The Use of Surface EMG in Biomechanics PDFDocument38 pagesThe Use of Surface EMG in Biomechanics PDFMarshall BananaNo ratings yet
- EMG Signal ProcessingDocument38 pagesEMG Signal ProcessingAbdi TeferiNo ratings yet
- ELEC5650 - Lecture - Physiological 20 - 21 Parts 2 and 1Document69 pagesELEC5650 - Lecture - Physiological 20 - 21 Parts 2 and 1Asad JaviedNo ratings yet
- EMG-bio Feed BackDocument52 pagesEMG-bio Feed BackRaghu NadhNo ratings yet
- Development of EMG Sensor For Transfemoral Amputation (Knee Flexor and Knee Extensor)Document5 pagesDevelopment of EMG Sensor For Transfemoral Amputation (Knee Flexor and Knee Extensor)seventhsensegroupNo ratings yet
- sEMG Tech: Strengths & LimitationsDocument4 pagessEMG Tech: Strengths & LimitationsJes GarciaNo ratings yet
- ElectromiographyDocument30 pagesElectromiographyphysics loverNo ratings yet
- EMG IntroductionDocument6 pagesEMG IntroductionramadanNo ratings yet
- BiosignalDocument7 pagesBiosignalveenadivyakishNo ratings yet
- By: Eng Mai HassanDocument17 pagesBy: Eng Mai HassanAhmed ElhuseinyNo ratings yet
- Introduction To EMGDocument4 pagesIntroduction To EMGGomugan MahalingamNo ratings yet
- The Role of Electrical Stimulators in Contemporary Physical TherapyDocument33 pagesThe Role of Electrical Stimulators in Contemporary Physical Therapyeager_learner100% (2)
- EMG (Electromyograph)Document2 pagesEMG (Electromyograph)Pulkit SharmaNo ratings yet
- Biopac Electomygraphy Lab: Bio 137 - Human Anatomy & Physiology IDocument6 pagesBiopac Electomygraphy Lab: Bio 137 - Human Anatomy & Physiology IIrina Luciana DumitriuNo ratings yet
- Biomedical Signals Improve LivesDocument10 pagesBiomedical Signals Improve Livesاحمد كاظمNo ratings yet
- Introduction EmgDocument3 pagesIntroduction EmgVaneet KumarNo ratings yet
- Emg Signal Noise Removal Using Neural Netwoks: Head of Department, Govt. Polytechnic, Amravati IndiaDocument23 pagesEmg Signal Noise Removal Using Neural Netwoks: Head of Department, Govt. Polytechnic, Amravati IndiabrianNo ratings yet
- Proyecto EstanciaDocument15 pagesProyecto Estanciaarath jaimesNo ratings yet
- On-the-Field Resistance-Tubing Exercises For Throwers: An Electromyographic AnalysisDocument8 pagesOn-the-Field Resistance-Tubing Exercises For Throwers: An Electromyographic AnalysisJaime SotoNo ratings yet
- Electrodiagnostic ProceduresDocument3 pagesElectrodiagnostic Proceduresakheel ahammedNo ratings yet
- Muscle Force Estimation From Lower Limb EMG Signals Using Novel Optimised Machine Learning TechniquesDocument17 pagesMuscle Force Estimation From Lower Limb EMG Signals Using Novel Optimised Machine Learning Techniquesu5600291No ratings yet
- Report on Training at Chettinad Health City HospitalDocument35 pagesReport on Training at Chettinad Health City HospitalChitralekha GaneshNo ratings yet
- Laryngeal ElectromyographyDocument21 pagesLaryngeal Electromyographyapi-19500641No ratings yet
- Experiment Ii: Electromyography: I. Goal of The Experiment and SummaryDocument7 pagesExperiment Ii: Electromyography: I. Goal of The Experiment and Summaryİlayda KavascıkNo ratings yet
- Noise in Biomedical InstrumentationDocument17 pagesNoise in Biomedical InstrumentationMadiha Wajeeh100% (1)
- Emg, NCVDocument38 pagesEmg, NCVMaria Isabel Nabor100% (1)
- Assignment 3.2 SolutionDocument2 pagesAssignment 3.2 SolutionHan hoNo ratings yet
- EMG Signal Processing for Prosthetic Hand ControlDocument14 pagesEMG Signal Processing for Prosthetic Hand ControlSrijan AdhikariNo ratings yet
- BME 449 Fall 2021 Experiement ProposalDocument1 pageBME 449 Fall 2021 Experiement ProposalkinleyNo ratings yet
- Simulate EMG Waveform and analyze noise (39Document7 pagesSimulate EMG Waveform and analyze noise (39dipakNo ratings yet
- A Myoelectric Hand For Writing English Alphabets (FINAL)Document8 pagesA Myoelectric Hand For Writing English Alphabets (FINAL)ashishsundarNo ratings yet
- 27 Feature Extraction and Classifier in The Development of Exoskeleton Based On Emg Signal Control A ReviewDocument7 pages27 Feature Extraction and Classifier in The Development of Exoskeleton Based On Emg Signal Control A ReviewTriwiyanto TriwiyantoNo ratings yet
- 2008 - Uso Eficiente de Energia No Setor Hospitalar - Hospitais PúblicosDocument13 pages2008 - Uso Eficiente de Energia No Setor Hospitalar - Hospitais PúblicosademargcjuniorNo ratings yet
- Neurofeedback - The Neurofeedback Book for Patients and Therapists : A Symphony of the MindFrom EverandNeurofeedback - The Neurofeedback Book for Patients and Therapists : A Symphony of the MindNo ratings yet
- Design Development and Analysis of a Nerve Conduction Study System An Auto Controlled Biofeedback ApproachFrom EverandDesign Development and Analysis of a Nerve Conduction Study System An Auto Controlled Biofeedback ApproachNo ratings yet
- Bioactivity study of modified curcumin loaded polymeric nanoparticlesFrom EverandBioactivity study of modified curcumin loaded polymeric nanoparticlesNo ratings yet
- A Critical Study of The Work Vaimanika ShastraDocument8 pagesA Critical Study of The Work Vaimanika ShastraMauroBonolloNo ratings yet
- ASR On DesikaaDocument5 pagesASR On DesikaaPankajashree Raghu100% (1)
- ReviewDocument3 pagesReviewPankajashree RaghuNo ratings yet
- 2011CI Rajan Financial DevelopmentDocument43 pages2011CI Rajan Financial DevelopmentAshima MishraNo ratings yet
- 38213-Astonishing Human BrainDocument115 pages38213-Astonishing Human BrainPankajashree RaghuNo ratings yet
- The Life of RamanujacharyaDocument271 pagesThe Life of RamanujacharyaPankajashree RaghuNo ratings yet
- Vedantasara of Sri Ramanujacharya Translated by V KrishnamacharyaDocument494 pagesVedantasara of Sri Ramanujacharya Translated by V KrishnamacharyaPankajashree RaghuNo ratings yet
- Uttararmacharit 00 BhavgoogDocument116 pagesUttararmacharit 00 BhavgoogPankajashree RaghuNo ratings yet
- Vaishnav It e Reformers of IndiaDocument194 pagesVaishnav It e Reformers of IndiaPankajashree RaghuNo ratings yet
- Inspiration Intuition EcstasyDocument75 pagesInspiration Intuition EcstasyPankajashree RaghuNo ratings yet
- Vakyapadiya With Eng TransDocument274 pagesVakyapadiya With Eng TransPankajashree RaghuNo ratings yet
- Intro SrivaishnavisamDocument19 pagesIntro SrivaishnavisamSuganya NarayananNo ratings yet
- Bhojaprabandha - Ballala Deva, Saradaprosad Vidyabhushan PDFDocument235 pagesBhojaprabandha - Ballala Deva, Saradaprosad Vidyabhushan PDFShishirNo ratings yet
- GD011 - Swami Desika DarsanamDocument88 pagesGD011 - Swami Desika DarsanamPankajashree Raghu100% (2)
- Relevance of Vedic Ideals of Education in The Modern Education SystemDocument7 pagesRelevance of Vedic Ideals of Education in The Modern Education SystemInternational Organization of Scientific Research (IOSR)No ratings yet
- Koil Olugu English 1954Document106 pagesKoil Olugu English 1954Pankajashree RaghuNo ratings yet
- YathirajavimsathyDocument32 pagesYathirajavimsathyPankajashree RaghuNo ratings yet
- Yathiraja SaptatiDocument291 pagesYathiraja SaptatiPankajashree RaghuNo ratings yet
- Ecg Artifact Removal From Surface Emg Signals by Combining Empirical Mode Decomposition and Independent Component AnalysisDocument4 pagesEcg Artifact Removal From Surface Emg Signals by Combining Empirical Mode Decomposition and Independent Component AnalysisPankajashree RaghuNo ratings yet
- YathirajavimsathyDocument32 pagesYathirajavimsathyPankajashree RaghuNo ratings yet
- Rationale of Rāhukālam TimesDocument5 pagesRationale of Rāhukālam TimesPankajashree RaghuNo ratings yet
- Intro SrivaishnavisamDocument19 pagesIntro SrivaishnavisamSuganya NarayananNo ratings yet
- TraditionDocument10 pagesTraditionPankajashree RaghuNo ratings yet
- 0 FCFD 50 e 4 CDC 148 Ece 000000Document12 pages0 FCFD 50 e 4 CDC 148 Ece 000000Pankajashree RaghuNo ratings yet
- Embc09 Jhlee Semg Emd08Document4 pagesEmbc09 Jhlee Semg Emd08Pankajashree RaghuNo ratings yet
- AA DL LS DPM Multivariate Synchrosqueezing SP 2015Document11 pagesAA DL LS DPM Multivariate Synchrosqueezing SP 2015Pankajashree RaghuNo ratings yet
- Denoising in Biomedical Signals Using Ensemble Empirical Mode DecompositionDocument7 pagesDenoising in Biomedical Signals Using Ensemble Empirical Mode DecompositionPankajashree RaghuNo ratings yet
- Emd 1Document26 pagesEmd 1Pankajashree RaghuNo ratings yet
- Exercise Muscle Fatigue Detection System Implementation Via Wireless Surface Electromyography and Empirical Mode DecompositionDocument4 pagesExercise Muscle Fatigue Detection System Implementation Via Wireless Surface Electromyography and Empirical Mode DecompositionPankajashree RaghuNo ratings yet
- Exo SkeltonDocument44 pagesExo SkeltonPankajashree Raghu100% (1)
- Project The Ant Ranch Ponzi Scheme JDDocument7 pagesProject The Ant Ranch Ponzi Scheme JDmorraz360No ratings yet
- Internship Report Recruitment & Performance Appraisal of Rancon Motorbikes LTD, Suzuki Bangladesh BUS 400Document59 pagesInternship Report Recruitment & Performance Appraisal of Rancon Motorbikes LTD, Suzuki Bangladesh BUS 400Mohammad Shafaet JamilNo ratings yet
- 04 Dasmarinas Vs Reyes GR No 108229Document2 pages04 Dasmarinas Vs Reyes GR No 108229Victoria Melissa Cortejos PulidoNo ratings yet
- StandardsDocument3 pagesStandardshappystamps100% (1)
- L-1 Linear Algebra Howard Anton Lectures Slides For StudentDocument19 pagesL-1 Linear Algebra Howard Anton Lectures Slides For StudentHasnain AbbasiNo ratings yet
- Group 4-Hospital Information System - His - QuizDocument2 pagesGroup 4-Hospital Information System - His - QuizGeeyan Marlchest B NavarroNo ratings yet
- Competency-Based Learning GuideDocument10 pagesCompetency-Based Learning GuideOliver BC Sanchez100% (2)
- Craft's Folder StructureDocument2 pagesCraft's Folder StructureWowNo ratings yet
- Chapter 2a Non Structured DataRozianiwatiDocument43 pagesChapter 2a Non Structured DataRozianiwatiNur AnisaNo ratings yet
- 28 Government Service Insurance System (GSIS) vs. Velasco, 834 SCRA 409, G.R. No. 196564 August 7, 2017Document26 pages28 Government Service Insurance System (GSIS) vs. Velasco, 834 SCRA 409, G.R. No. 196564 August 7, 2017ekangNo ratings yet
- Cib DC22692Document16 pagesCib DC22692Ashutosh SharmaNo ratings yet
- BAR Digest MenuDocument4 pagesBAR Digest MenuFloila Jane YmasNo ratings yet
- Material Properties L2 Slides and NotesDocument41 pagesMaterial Properties L2 Slides and NotesjohnNo ratings yet
- Tyron Butson (Order #37627400)Document74 pagesTyron Butson (Order #37627400)tyron100% (2)
- Battery Impedance Test Equipment: Biddle Bite 2PDocument4 pagesBattery Impedance Test Equipment: Biddle Bite 2PJorge PinzonNo ratings yet
- Individual Differences: Mental Ability, Personality and DemographicsDocument22 pagesIndividual Differences: Mental Ability, Personality and DemographicsAlera Kim100% (2)
- Benzon CaseDocument3 pagesBenzon Casejulieanne07100% (1)
- Prestressing ProductsDocument40 pagesPrestressing ProductsSakshi Sana100% (1)
- Elementary School: Cash Disbursements RegisterDocument1 pageElementary School: Cash Disbursements RegisterRonilo DagumampanNo ratings yet
- 6vortex 20166523361966663Document4 pages6vortex 20166523361966663Mieczysław MichalczewskiNo ratings yet
- (Free Scores - Com) - Stumpf Werner Drive Blues en Mi Pour La Guitare 40562 PDFDocument2 pages(Free Scores - Com) - Stumpf Werner Drive Blues en Mi Pour La Guitare 40562 PDFAntonio FresiNo ratings yet
- Nature of ConversionDocument18 pagesNature of ConversionKiranNo ratings yet
- Indian Institute of Management KozhikodeDocument5 pagesIndian Institute of Management KozhikodepranaliNo ratings yet
- Diagnostic Information For Database Replay IssuesDocument10 pagesDiagnostic Information For Database Replay IssuesjjuniorlopesNo ratings yet
- CCS PDFDocument2 pagesCCS PDFАндрей НадточийNo ratings yet
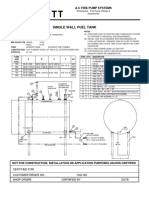
- Single Wall Fuel Tank: FP 2.7 A-C Fire Pump SystemsDocument1 pageSingle Wall Fuel Tank: FP 2.7 A-C Fire Pump Systemsricardo cardosoNo ratings yet
- Global Cleantech Innovation Programme IndiaDocument122 pagesGlobal Cleantech Innovation Programme Indiaficisid ficisidNo ratings yet
- Computers As Components 2nd Edi - Wayne WolfDocument815 pagesComputers As Components 2nd Edi - Wayne WolfShubham RajNo ratings yet
- Philippine Architecture, Film Industry EvolutionDocument4 pagesPhilippine Architecture, Film Industry EvolutionCharly Mint Atamosa IsraelNo ratings yet
- Aptio ™ Text Setup Environment (TSE) User ManualDocument42 pagesAptio ™ Text Setup Environment (TSE) User Manualdhirender karkiNo ratings yet