You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Revue Des Études Juives. 1880. Volumes 76-77.Document474 pagesRevue Des Études Juives. 1880. Volumes 76-77.Patrologia Latina, Graeca et OrientalisNo ratings yet
- Encyclopedia of Controlled Drug Delivery (2 Vols) - E. Mathiowitz (Wiley, 1999) WWDocument903 pagesEncyclopedia of Controlled Drug Delivery (2 Vols) - E. Mathiowitz (Wiley, 1999) WWCiontu Valentin100% (4)
- The Epfl Student'S GuideDocument36 pagesThe Epfl Student'S GuideFabián LatorreNo ratings yet
- Medical Topography of Brazil and Uruguay With Incidental Remarks. G. R. B. H o R N e RDocument323 pagesMedical Topography of Brazil and Uruguay With Incidental Remarks. G. R. B. H o R N e RMarcia SiqueiraNo ratings yet
- 1909 Operation of Geographic SEMPLEDocument19 pages1909 Operation of Geographic SEMPLElouiscoraxNo ratings yet
- Prefácio Medical HistoryDocument2 pagesPrefácio Medical HistoryMarcia SiqueiraNo ratings yet
- Patterns of Crime Victimization in Latin AmericaDocument34 pagesPatterns of Crime Victimization in Latin AmericaMarcia SiqueiraNo ratings yet
- Chapter 12 Airs Waters Places Perennial Puzzles of HealthDocument7 pagesChapter 12 Airs Waters Places Perennial Puzzles of HealthMarcia SiqueiraNo ratings yet
- Estados Unidos Do Brasil Geographia, Ethnographia, Estatistica E. ReclusDocument527 pagesEstados Unidos Do Brasil Geographia, Ethnographia, Estatistica E. ReclusMarcia SiqueiraNo ratings yet
- Classes of Geographic Influences - Ellen Churchill SempleDocument13 pagesClasses of Geographic Influences - Ellen Churchill SempleMarcia SiqueiraNo ratings yet
- Usage GuidelinesDocument704 pagesUsage GuidelinesMarcia SiqueiraNo ratings yet
- Lista de Ilustrações Medical HistoryDocument3 pagesLista de Ilustrações Medical HistoryMarcia SiqueiraNo ratings yet
- Index Medical HistoryDocument8 pagesIndex Medical HistoryMarcia SiqueiraNo ratings yet
- Medical History Volume 44 Issue S20Document2 pagesMedical History Volume 44 Issue S20Marcia SiqueiraNo ratings yet
- Chapter 10 The First Global Map of The Distribution of HumanDocument11 pagesChapter 10 The First Global Map of The Distribution of HumanMarcia SiqueiraNo ratings yet
- Chapter 11 Heinrich Berghaus's Map of Human DiseasesDocument24 pagesChapter 11 Heinrich Berghaus's Map of Human DiseasesMarcia SiqueiraNo ratings yet
- Chapter 7 The Geography of Health and The Making of TheDocument26 pagesChapter 7 The Geography of Health and The Making of TheMarcia SiqueiraNo ratings yet
- Chapter 8 Geography Race and Nation AustraliaDocument15 pagesChapter 8 Geography Race and Nation AustraliaMarcia SiqueiraNo ratings yet
- Chapter 6 August Hirsch As Critic of and Contributor ToDocument21 pagesChapter 6 August Hirsch As Critic of and Contributor ToMarcia SiqueiraNo ratings yet
- Chapter 9 Humboldtian Representations in MedicalDocument15 pagesChapter 9 Humboldtian Representations in MedicalMarcia SiqueiraNo ratings yet
- Chapter 5 Adolf Mühry GöttingenDocument13 pagesChapter 5 Adolf Mühry GöttingenMarcia SiqueiraNo ratings yet
- Chapter 4 The Debate About Acclimatization in The DutchDocument17 pagesChapter 4 The Debate About Acclimatization in The DutchMarcia SiqueiraNo ratings yet
- Medical Topography Brazil and Uruguay: Incidental RemarksDocument334 pagesMedical Topography Brazil and Uruguay: Incidental RemarksMarcia SiqueiraNo ratings yet
- Chapter 1 Histories of Medical GeographyDocument27 pagesChapter 1 Histories of Medical GeographyMarcia SiqueiraNo ratings yet
- Biometeorology of Health StatusDocument34 pagesBiometeorology of Health StatusMarcia SiqueiraNo ratings yet
- Cap 3 Representations of IndiaDocument20 pagesCap 3 Representations of IndiaMarcia SiqueiraNo ratings yet
- Cem Anos de Endemias e EpidemiasDocument13 pagesCem Anos de Endemias e EpidemiasMarcia SiqueiraNo ratings yet
- Geographies of Health Cap 1 A 3Document49 pagesGeographies of Health Cap 1 A 3Marcia SiqueiraNo ratings yet
- Autores Medical HistoryDocument8 pagesAutores Medical HistoryMarcia SiqueiraNo ratings yet
- Environmental Thought and Action Pre-Modern CosgroveDocument15 pagesEnvironmental Thought and Action Pre-Modern CosgroveMarcia SiqueiraNo ratings yet
- Jean Brunhes BioDocument1 pageJean Brunhes BioMarcia SiqueiraNo ratings yet
- Blink Taxi Fare Sheet 4scribdDocument1 pageBlink Taxi Fare Sheet 4scribdtim8529No ratings yet
- Iso 6520 1 en FR PDFDocument11 pagesIso 6520 1 en FR PDFBahloul MohamedNo ratings yet
- Shostakovich Jazz Waltz 2 OrchestraDocument11 pagesShostakovich Jazz Waltz 2 OrchestraLi XianjiNo ratings yet
- Advice To Students Wishing To Become Conference InterpretersDocument6 pagesAdvice To Students Wishing To Become Conference InterpretersAdriatik MetaNo ratings yet
- Geofrey R. Watt - Calvin S Geneva Confronts Magic and Witchcraft The Evidence From The ConsistoryDocument31 pagesGeofrey R. Watt - Calvin S Geneva Confronts Magic and Witchcraft The Evidence From The ConsistoryMilica KovacevicNo ratings yet
- Thinking Under Turbulence. Geneva Colloquium, Published by CCC/HEAD Geneva and Motto Books, 2017, 192 Pages.Document6 pagesThinking Under Turbulence. Geneva Colloquium, Published by CCC/HEAD Geneva and Motto Books, 2017, 192 Pages.MERODENENo ratings yet
- 2016 GCSP Prize For Innovation in Global Security FlyerDocument1 page2016 GCSP Prize For Innovation in Global Security FlyersteelyheadNo ratings yet
- Jimmie Durham: Postmodernist 'Savage' ArtistDocument14 pagesJimmie Durham: Postmodernist 'Savage' ArtistAdriel VisottoNo ratings yet
- Mallet Du Pan and The French RevolutionDocument468 pagesMallet Du Pan and The French RevolutionNafisa LabibaNo ratings yet
- Dimensions for refractory bricksDocument5 pagesDimensions for refractory bricksSimon sunNo ratings yet
- List of Important International Organizations and HeadquartersDocument3 pagesList of Important International Organizations and Headquartersvickohli18No ratings yet
- Iso 565Document8 pagesIso 565Aravind BabuNo ratings yet
- E. William Monter - Calvin's Geneva (John Wiley 1967)Document138 pagesE. William Monter - Calvin's Geneva (John Wiley 1967)Mark CohenNo ratings yet
- Not Just Another Hunt! – Music for Horn and PianoDocument5 pagesNot Just Another Hunt! – Music for Horn and PianoKrystal kohNo ratings yet
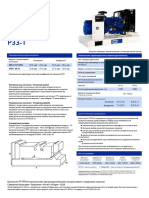
- Manual de FG Wilson P33-1Document4 pagesManual de FG Wilson P33-1Rene MirandaNo ratings yet
- Iso 8501-2Document178 pagesIso 8501-2NauthizNo ratings yet
- Struktur Dan Organisasi Pengakap Peringkat AntarabangsaDocument22 pagesStruktur Dan Organisasi Pengakap Peringkat AntarabangsaMuhammadHisyamuddin0% (1)
- Ikrar Lambang Bendera LaguDocument29 pagesIkrar Lambang Bendera LaguEricson GinsosNo ratings yet
- IEC 60364 - 1 - 2001 - Electrical Installation of BuildingsDocument80 pagesIEC 60364 - 1 - 2001 - Electrical Installation of BuildingsRebeca MancillaNo ratings yet
- Poster - KAKKAMPI Forum 04 (04 September 2005)Document1 pagePoster - KAKKAMPI Forum 04 (04 September 2005)KAKKAMPINo ratings yet
- F A Forel and LimnologyDocument13 pagesF A Forel and LimnologyTaukir AhmedNo ratings yet
- Europe BanksDocument39 pagesEurope BanksSheel ThakkarNo ratings yet
- Cathedral of Saint Pierre: The Chapel of The MaccabeansDocument6 pagesCathedral of Saint Pierre: The Chapel of The MaccabeansMaria MargiolouNo ratings yet
- Iso 4998Document12 pagesIso 4998Aravind BabuNo ratings yet
- Have A Look at Our: ContactsDocument3 pagesHave A Look at Our: ContactsIshan PatilNo ratings yet
- IEC 61010-2-041-1995 ScanDocument55 pagesIEC 61010-2-041-1995 ScanD SaiRajaNo ratings yet
- Iec 60726Document45 pagesIec 60726Sergio LungrinNo ratings yet