You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Benign Anorectal Conditions: Ahmed Badrek-AmoudiDocument20 pagesBenign Anorectal Conditions: Ahmed Badrek-AmoudiAna De La RosaNo ratings yet
- Reh Prevod SpineDocument4 pagesReh Prevod SpineErmin HamidovicNo ratings yet
- Oxygen Administration in Infants: ReviewDocument6 pagesOxygen Administration in Infants: ReviewIndra PutraNo ratings yet
- Quick Reference DMARDsDocument12 pagesQuick Reference DMARDsEman MohamedNo ratings yet
- Rife Consolidated Annotated Frequency List - EMR Labs, LLCDocument38 pagesRife Consolidated Annotated Frequency List - EMR Labs, LLCMia Janette Husted MadsenNo ratings yet
- Questões - Questoes de Vestibular3 PDFDocument6 pagesQuestões - Questoes de Vestibular3 PDFVictor Araujo PontesNo ratings yet
- Case StudyDocument5 pagesCase StudyDeo Micah GoNo ratings yet
- Cupping & Hijama BookDocument25 pagesCupping & Hijama BookMatthew GilsonNo ratings yet
- Test Bank For Essentials of Pathophysiology 3rd Edition, PorthDocument23 pagesTest Bank For Essentials of Pathophysiology 3rd Edition, PorthILL110100% (1)
- ECT - Patient LeafletDocument4 pagesECT - Patient LeafletSarah GrixtiNo ratings yet
- Intestinal Amebiasis: A Concerning Cause of Acute Gastroenteritis Among Hospitalized Lebanese ChildrenDocument9 pagesIntestinal Amebiasis: A Concerning Cause of Acute Gastroenteritis Among Hospitalized Lebanese ChildrenFrancisca OrenseNo ratings yet
- PAPO Statement Regarding The PhilHealth Cataract Operations ScandalDocument5 pagesPAPO Statement Regarding The PhilHealth Cataract Operations ScandalJess LorenzoNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanPutra AginaNo ratings yet
- PepDocument22 pagesPepNithin NairNo ratings yet
- DR Titus Presentation of CBD Oil and Further Why & How CBD Oil (Cannabinoids) Works & Effect Your Body - You Are Born With CBD Receptors Within Your Body Which Became Confirmed Back in 1992Document46 pagesDR Titus Presentation of CBD Oil and Further Why & How CBD Oil (Cannabinoids) Works & Effect Your Body - You Are Born With CBD Receptors Within Your Body Which Became Confirmed Back in 1992indigo1967No ratings yet
- National Mental Health ProgrammeDocument4 pagesNational Mental Health ProgrammeMANISH MAMIDINo ratings yet
- Managing Preeclampsia and Eclampsia with Magnesium SulfateDocument23 pagesManaging Preeclampsia and Eclampsia with Magnesium SulfateDevy Oktavia AnisaNo ratings yet
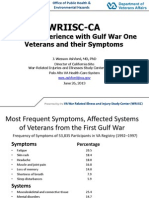
- Presentation - Dr. Wes Ashford - IOM Gulf War Illness "CMI" Panel.Document16 pagesPresentation - Dr. Wes Ashford - IOM Gulf War Illness "CMI" Panel.Anthony HardieNo ratings yet
- NCM 106 Pharmacology Task Performace Written Assignment Format For FINALSDocument5 pagesNCM 106 Pharmacology Task Performace Written Assignment Format For FINALSNoemie DanaoNo ratings yet
- Hospital ProposalDocument5 pagesHospital ProposalSushant Sharma100% (1)
- Community Health Nursing Part 1 & 2Document35 pagesCommunity Health Nursing Part 1 & 2mark OrpillaNo ratings yet
- Nutrition Management For CancerDocument50 pagesNutrition Management For CancerPCMC Dietitians NDDNo ratings yet
- Species Common/Other Name Pathogenesis Mot/Infective Stage Diagnostic Stage I. NematodesDocument2 pagesSpecies Common/Other Name Pathogenesis Mot/Infective Stage Diagnostic Stage I. NematodesautumntreesNo ratings yet
- Textbook of Oral Medicine Oral DiagnosisDocument924 pagesTextbook of Oral Medicine Oral DiagnosisSonal100% (1)
- 2019 - Health Promoting Lifestyle and Its Determinants Among FemaleDocument6 pages2019 - Health Promoting Lifestyle and Its Determinants Among FemaleSubhan AnsariNo ratings yet
- Risk Factors of Cesarean Delivery Due To Cephalopelvic Disproportion in Nulliparous Women at Sisaket HospitalDocument7 pagesRisk Factors of Cesarean Delivery Due To Cephalopelvic Disproportion in Nulliparous Women at Sisaket HospitalManangioma ManNo ratings yet
- How To Stop Macular DegenerationDocument66 pagesHow To Stop Macular DegenerationJenny Bhatt100% (1)
- Free Report-Smoking CessationDocument5 pagesFree Report-Smoking CessationdapextilburyNo ratings yet
- (Escitalopram) : NC CH O N CH C H ODocument2 pages(Escitalopram) : NC CH O N CH C H OKhurram AzizNo ratings yet
- Sexually Transmitted Disesase.: Ralph Gabriel QuinalDocument16 pagesSexually Transmitted Disesase.: Ralph Gabriel QuinalJohn Michael MonteflacoNo ratings yet