You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
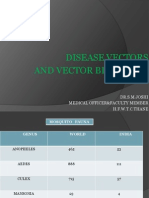
- Disease Vectors and Vector BionomicsDocument16 pagesDisease Vectors and Vector BionomicsSuhas JoshiNo ratings yet
- 2020 Safe List: Drugs That Are Considered To Be SAFE For Use in The Acute PorphyriasDocument2 pages2020 Safe List: Drugs That Are Considered To Be SAFE For Use in The Acute PorphyriasAlexandra LupuNo ratings yet
- Antigen - Antibody Reactions: Dr.D.BinduDocument46 pagesAntigen - Antibody Reactions: Dr.D.Bindubindu dhanapalNo ratings yet
- Pneumoslide LiteratratureDocument23 pagesPneumoslide LiteratratureGREENCROSS PALDINo ratings yet
- Legionella SamplingDocument71 pagesLegionella SamplingAnonymous G6ceYCzwt100% (1)
- Management of Peri-Implant Mucositis and Peri-Implantitis PDFDocument19 pagesManagement of Peri-Implant Mucositis and Peri-Implantitis PDFgirl33No ratings yet
- Herbal Approaches for Liver DisordersDocument45 pagesHerbal Approaches for Liver DisordersRakshit JainNo ratings yet
- TBL 15 V4 - Viral PneumoniaDocument24 pagesTBL 15 V4 - Viral PneumoniaFaysal RafiNo ratings yet
- Colloidal Silver Testimonials PDFDocument17 pagesColloidal Silver Testimonials PDFADRNo ratings yet
- Feline Dermatophytosis Treatment RecommendationsDocument21 pagesFeline Dermatophytosis Treatment RecommendationsFrancisca Thenée SerranoNo ratings yet
- Antibiotic Resistance - A Growing Global Health IssueDocument6 pagesAntibiotic Resistance - A Growing Global Health IssueBramaNo ratings yet
- Mouth WashesDocument33 pagesMouth WashesMaxNo ratings yet
- JCR Article PDFDocument3 pagesJCR Article PDFSai KalyanNo ratings yet
- ICOPHAI Abstract Book 2017Document131 pagesICOPHAI Abstract Book 2017Omar TalhaNo ratings yet
- UC Davis Koret Shelter Medicine Program - Flea Treatment in Animal Shelters - 2013-10-09Document2 pagesUC Davis Koret Shelter Medicine Program - Flea Treatment in Animal Shelters - 2013-10-09Kitt KaosNo ratings yet
- Odessa National Medical University: Surgical InfectionsDocument34 pagesOdessa National Medical University: Surgical InfectionsDrRajneesh ShastriNo ratings yet
- Communicable DiseasesDocument8 pagesCommunicable DiseasesKarla Fralala100% (1)
- Preparation Outline (Informative Speech)Document3 pagesPreparation Outline (Informative Speech)AmirAircoolNo ratings yet
- Immune Response ExplainedDocument34 pagesImmune Response ExplainedAtanas NaydenovNo ratings yet
- Food PoisoningDocument7 pagesFood PoisoningYoser ThamtonoNo ratings yet
- Crop Protection - Plant Pathology (Session 1-3)Document382 pagesCrop Protection - Plant Pathology (Session 1-3)jessamendoza179No ratings yet
- Takushige Retreat J LSTRDocument5 pagesTakushige Retreat J LSTRPascalis Adhi KurniawanNo ratings yet
- The Social Impact of Covid-19Document1 pageThe Social Impact of Covid-19Trisha MaguikayNo ratings yet
- Expanded Program On Immunization Philippines)Document8 pagesExpanded Program On Immunization Philippines)Mark AcuzarNo ratings yet
- Guidelines: Consolidated Guidelines On HIV Testing Services - 5cs: Consent, Confidentiality, Counselling, Correct Results and ConnectionDocument192 pagesGuidelines: Consolidated Guidelines On HIV Testing Services - 5cs: Consent, Confidentiality, Counselling, Correct Results and ConnectionHayZara Madagascar100% (2)
- Production of Germicidal SoapDocument39 pagesProduction of Germicidal Soapapi-233859278No ratings yet
- Kumar Indoor Air Quality Study Summary - Proffer SweepsDocument1 pageKumar Indoor Air Quality Study Summary - Proffer SweepsAnonymous Pb39klJNo ratings yet
- TUGas Bahasa InggrisDocument86 pagesTUGas Bahasa InggrisRianda Dwi PutraNo ratings yet
- Submitted By: Group 6 MT 3BDocument49 pagesSubmitted By: Group 6 MT 3BChristine Joy TanglaoNo ratings yet
- Ap Biology CH 19 Reading GuideDocument4 pagesAp Biology CH 19 Reading Guideapi-293174360No ratings yet