IOSR Journal of Computer Engineering (IOSR-JCE)
e-ISSN: 2278-0661,p-ISSN: 2278-8727, Volume 17, Issue 5, Ver. IV (Sep. Oct. 2015), PP 01-06
www.iosrjournals.org
Development of a Force Acquisition Instrument for Orthodontics
John Carlo Valdez1
1
(Department of Computer Engineering, University of the East, Philippines)
Abstract : In the field of Orthodontics, various appliances and components are being utilized to facilitate tooth
movement. Tissue responses range from physiologic tooth movement to irreversible damage such as pulling a
tooth out of a socket. The aim of the study is to develop a force acquisition instrument which can accurately
measure forces applied by orthodontic components to the tooth. Furthermore, in this paper it test and present
the linearity, bias, and significant difference on the measured and true values when exposed to varying room
temperature of the developed force acquisition instrument for orthodontics.
Keywords: force acquisition instrument, orthodontics, force measurement, ortho-components
I.
Introduction
Edward Angle, the father of Modern Orthodontics, is credited with the emergence of orthodontics as a
specialty. Orthodontic treatment involves movement of malpositioned teeth. Brackets are connected to the
surface of the patients teeth and an arch wire is placed in a slot of each bracket to move the teeth [1].
Adjustments are made with the replacement of arch wires and use of elastics and coil springs.
A dynamometer is a general instrument that evaluates an applied force. In the practice of orthodontics,
it measures the forces specifically applied on the tooth by orthodontic components. Current clinical
dynamometer is constructed for measuring tensile and compression forces exerted by the springs and elastics for
a range of 1oz-16 oz. It is calibrated with 1 oz. single line and 4 oz. double line increment. The double-ended
calibrated shaft makes it possible to evaluate pull and push forces.
An Australian research that focused on the effect of a static magnetic field on orthodontic movement in
the rat [2], measured the residual forces in each appliance from the induction of tooth movement and verified at
the end of each experimental period using a dynamometer. In [3], it demonstrated the use of the dynamometer in
their application in ensuring that the magnitude of load was always 85g from the force applied by the Ni-Ti
closed-coil springs in the effects of orthodontic load on the periodontium of autogenously transplanted teeth in
beagle dogs.
In general, the clinical dynamometers capability varies on the specific application in orthodontics,
ranging from simply assessing the applied force by the orthodontic appliances to estimate the tooth movement
output to standardizing the thickness of adhesive material [4], among others.
The researcher had carefully studied the clinical dynamometer being used in the dental profession.
From the testaments provided to the researcher by the dental faculty members and dental practitioners, no
dynamometer in the market has been manufactured with precise measurement and with sufficient amount of
significant numbers to accurately measure the force applied on the tooth. Dental practitioners and students use
the aid of mechanical dynamometer in measuring gram-force acting on the tooth. Though inaccurate, they
accept the truncated gram-force reading of the device with insufficient number of significant values in the
device scale.
In this study, it aims to develop a force acquisition instrument to measure these forced for orthodontics.
Specifically, it determines the acceptability of the proposed instrument, during the testing, it must satisfy the
hypothesis set to test the linearity, that no offset exist between true and measured value at the specific target
both for the minimum and maximum range, (Ho: a = 0) and bias, that slope between the true and measured
values is equal to one, (Ho: b = 1) at the accuracy of the measurements over the full range. Likewise, no
significant difference must be observed in the measurement once the instrument is exposed to varying
temperature during orthodontic procedures (Ho: c = 0).
II.
Related Literature
Certain situations still pose challenges in the practice of orthodontics, even with the great advancement
in technology. The researcher is inspired by how engineering should be applied to a different field of study and
practice. With his specialty in computer engineering, the researcher is initiated to be engaged in an
interdisciplinary application between engineering and orthodontics. Thus, applying the field of biomedical
engineering to enhance and improve the efficiency of orthodontic practice.
The dental profession has to address the following challenges: properly determine the nominal force
applied during orthodontic tooth movement and how this will affect the efficiency of orthodontic tooth
movement.
DOI: 10.9790/0661-17540106
www.iosrjournals.org
1 | Page
Development of a Force Acquisition Instrument for Orthodontics
Orthodontic tooth movement is defined as result of a biologic response to interference in the
physiologic equilibrium of the dentofacial complex by an externally applied force [5]. Only small amounts of
force might be required to effect this outcome, which is accompanied by remodeling changes in the periodontal
ligament and alveolar bone [6].
A typical mechanical dynamometer is used to measure the force enacted by elastics, arch wires and coil
springs as shown in [7]. The researcher asked Orthodontic postgraduate students in the University of the East
Graduate School to use this device. The current device used is unable to provide an exact numerical value of the
measured force. The students are unable to assume nor estimate the exact value due to the limitation of the
device. They only consider the most significant value from the scale, i.e. if there is a scale point between
20grams-force and 40 grams-force, the user cannot include the values in between.
III.
Design Methodology
In this study, a system design was created to gather and measure the force applied by the orthodontic
appliances. As suggested by several research studies, a typical magnitude of force to be applied to achieved
orthodontic tooth movement ranges from 25 grams-force to 1515 grams-force [8][9][10]. However, for this
experimental set-up, forces from 5 to 550 grams-force were utilized.
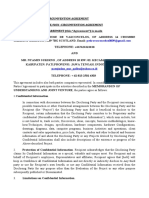
A. Block Diagram
The development of the instrument was guided with the following crucial components as illustrated at
Fig. 1. The full-bridge force sensor configuration was used to acquire the force applied in the sensor in an
analog signal. In which it is necessary to convert the analog signal taken to a digital signal by means of an
analog-to-digital converter (ADC). This is to ensure that the communication of the signal is processed in
accordance to the compability of the microcontroller unit to process the gathered data. Furthermore, the ADC
increases the numerical resolution of the output signal to provide the microcontroller unit to process and display
a higher resolution in the display panel. And lastly, the switch acts a force voltage reference reset switch to
ensure that the reference reading before any measurement is set to zero.
Fig. 1.
Force Measurement Instrument Block Diagram
B. Hardware Components and Circuits
In this section, it further elaborates the circuit design of each hardware components.
1) Full-Bridge Force Sensor Configuration:
The force sensor is configured to have four active elements namely the: E+, S+, S-, and E-. Where, E+
and E- are the active elements measuring compressive forces while S+ and S- are the active elements measuring
tensile forces. These pins (E+ and E-) are then connected to be fed with a voltage source, at a nominal 5V, from
the ADC circuit and pins (S+ and S-) are analog signals that holds the corresponding values of the applied force
which are then to be process by the ADC with a 10.15mV/V output rating.
Fig. 2.
DOI: 10.9790/0661-17540106
Full-Bridge Configuration of the Force Sensor
www.iosrjournals.org
2 | Page
Development of a Force Acquisition Instrument for Orthodontics
2) 24-bit Analog-to-Digital Converter Circuit:
It is a 24-bit analog-to-digital converter for industrial control applications to interface with a bridge
sensor. The circuit is powered with a 5V AVDD analog power supply. An SOP-16L package integrated chip
was used to minimize the space it consumes during the design. The X1 pin (Pin 14) is set to ground to activate
the on-chip oscillator where the output data rate when it uses the internal oscillator is 10. The PD_SCK (Pin 11)
and DOUT (Pin 12) are used for data retrieval, input selection, and gain selection for the microcontroller unit.
Fig. 3.
24-bit Analog-to-Digital Converter Circuit
3) Power Supply:
The normal voltage operability of the circuits generally falls within the 5V source. This circuit ensures
that a stable source of 5V is fed to the entire circuitry system and prevent fluctuation of the voltage signal and
regulate an external battery (V1) to an output voltage with a stable 5V analog voltage.
Fig. 4.
5V Power Supply Circuit
4) PIC16F876A, Force Voltage Reference Reset Switch, and Display:
The PIC16F876A an 28-pin Shrink Small Outline Package (SSOP) which is optimal to achieve
compact design of the circuit and with reasonable operating clock speed, with the 4MHz crystal (X1) which is
ideal for real-time data acquisition processing. The processed digital output by the ADC are then fed to the RA1
(Pin 3) and RA2 (Pin 4) to numerically program the values and display the output at the three 7-segment
display. The displays are multiplex with the microcontroller unit from RB7 (Pin 28) to RB1 (Pin 22) and RC4
(Pin 15) to RC6 (Pin 17) where used to activate the particular 7-segment display and show its corresponding
reading. The VDD (Pin 20) is supplied with a +5V supply while VSS (Pin 8 and Pin 9) were set to ground. In
addition, the SW1 (Pin 6 and Pin 7) is introduced such that any measurement reading, before the actual
measurement, is always set to zero. This is to ensure that no offset will be observed once the device attempts to
conduct the measuring.
DOI: 10.9790/0661-17540106
www.iosrjournals.org
3 | Page
Development of a Force Acquisition Instrument for Orthodontics
Fig. 5. PIC16F876A and 3 7-Segment Display
C. System Flow Chart
As shown in Fig. 6, it presents the flow of the operation of the force measuring instrument from how it
gathers the force data, processing, and displaying the expected real-time values.
Fig. 6.
Force Measurement Instrument Flow Chart
D. Test Procedures
The instrument underwent numerous testing to ensure that the measurement reading is stable. The
measured and true values are linear or at most nearly close to each other. And the measurement will not be
affected by the given range of room temperature. The instrument were tested using the Universal Testing
Machine (UTM) where it applied forces ranging from 40 grams-force to 550 grams-force. These force ranges
are divided into two: the minimum and maximum range of measurement, with 40-80 grams-force and 300-550
grams-force, respectively. Under each force increment in the testing, each was given with 10 test sample. The
applied force by the UTM is considered the true value in which it will then be compared with the reading taken
by the instrument which is the measured value.
DOI: 10.9790/0661-17540106
www.iosrjournals.org
4 | Page
Development of a Force Acquisition Instrument for Orthodontics
IV.
Results
In this study, it was tested that the hypothesis set in the research satisfies the followings: (1) no offset
exist between the true and measured values; (2) the slope between the true and measured values is equal to one;
and (3) the measured values with respect to the true values were not affected when exposed to various levels of
room temperature.
Using the SPSS, a statistical software, the gathered data are transformed which supports to validate the
hypothesis set in this study. The followings are the results taken after the testing procedure.
True Value
Table 1. t-Test on the Significance Between the True Value and Measured Value from 40 grams-force to
80 grams-force for the Minimum Force Measurement
g-f
40
Mean
39.8
Measured Value
SD
t-value
0.422
-1.500
P-value
0.168
45
44.8
0.422
-1.500
0.168
50
49.8
0.422
-1.500
0.168
55
54.8
0.422
-1.500
0.168
60
59.7
0.483
-1.964
0.081
65
64.9
0.316
-1.000
0.343
70
69.7
0.675
-1.406
0.193
75
74.8
0.422
-1.500
0.168
80
79.9
0.316
-1.500
0.343
True Value
Table 2. t-Test on the Significance Between the True Value and Measured Value from 300 grams-force to
550 grams-force for the Minimum Force Measurement
Measured Value
SD
t-value
0.707
-2.236
g-f
300
Mean
299.5
P-value
0.052
325
324.4
0.843
-2.25
0.051
350
349.3
1.16
-1.909
0.089
375
374.7
0.483
-1.964
0.081
400
399.5
0.707
-2.236
0.052
425
424.5
0.707
-2.236
0.052
450
449.9
0.732
-0.429
0.678
475
474.5
0.972
-1.67
0.138
500
498.8
3.521
-1.078
0.309
525
524.4
0.843
-2.25
0.051
550
549.5
0.972
-1.627
0.138
Table 3. Model Summary for the Linearity of forces from 40 gram-force to 550 gram-force
Model
1
R
1.000
R2
1.000
Adjusted R2
1.000
Std. Error of the Estimate
2.05523
Table 4. One-Way ANOVA on the Significant Difference in the Measurement on the 50 grams-force
When Exposed to Varying Temperature
Source
Columns
SS
0.787
df
7
Error
13.228
72
Total
14.015
79
MS
0.112
0.184
F-value
0.612
P-value
0.744
Table 5. One-Way ANOVA on the Significant Difference in the Measurement on the 500 grams-force
When Exposed to Varying Temperature
Source
Columns
SS
15.350
df
7
Error
220.599
72
Total
235.949
79
DOI: 10.9790/0661-17540106
MS
2.193
3.064
F-value
0.716
www.iosrjournals.org
P-value
0.659
5 | Page
Development of a Force Acquisition Instrument for Orthodontics
V.
Discussions
Referring to Table 1 and 2, the P-value calculated shows values which are greater than the 0.05 level of
confidence. This also suggests that the hypothesis set (Ho: a=0) is accepted. The test range is true from the
minimum measurement range of 40-80 grams-force and for the maximum measurement range of 300-550
grams-force.
A model summary, in Table 3, was generated to determine if the true and measured values produce a
slope equal to one. Using the test values taken from 40 grams-force to 550 grams-force, with 10 test samples
for each incremented forces, the R2 value is equal to one (Ha: b=1). Statistically, it suggests that there is a
perfect correlation between the values of the true and the measured force.
Lastly, under the exposure of varying temperature during testing, it determines if there is a significance
in the measured values and the true values. Using one-way ANOVA, under Table 4, the test sample at 50 gramsforce when exposed from 18C to 32C shows a P-value of 0.744. While in Table 5, at a 500 grams-force
sample, it exhibit a P-value of 0.659. Comparing the computed P-value, the instruments reading were
comparable with the true values when exposed to various level of room temperature.
VI.
Conclusion
In this study, it was tested that the hypothesis set in the research satisfies the followings: (1) no offset
exist between the true and measured values; (2) the slope between the true and measured values is equal to one;
and (3) the measured values with respect to the true values were not affected when exposed to various levels of
room temperature.
References
[1]
[2]
[3]
[4]
[5]
[6]
[7]
[8]
[9]
[10]
Parker, L., Setting It Straight Advanced Orthodontics. Retrieved from http://www.dentalcare.com/en-US/dentaleducation/continuing-education/ce326/ce326.aspx?ModuleName=coursecontent&PartID=1&SectionID=Tengku, B., Joseph, B., Harbrow, D., Taverne, A., & Symons, A. (2010). Effect of a static magnetic field on orthodontic tooth
movement in the rat. The European Journal of Orthodontics, 22(5), 475-487.
Lu, L., Sun, H.S., Xue, H., Guo, J., and Chen, Y. (2013). Effects of orthodontic load on the periodontium of autogenously
transplanted teeth in beagle dogs. Journal of Zhejiang University SCIENCE B.
Invernic, S., Maruo, I., Camargo, E., Hirata, T., Maruo, H., Filho, O., and Tanaka, O. (2012). Influence of Ortho Primer Morelli
adhesion booster on orthodontic brackets shear bond strength. Dental Press J Orthod, 17(3), 31-39.
Proffit, W. (2007). Biological basis of orthodontic therapy. In Contemporary Orthodontics (4th ed., pp. 331-358). Mosby, St.
Louise.
Vinod, K., and Davidovitch, Z. (2006). Cellular, molecular, and tissue-level reactions to orthodontic force. American Journal of
Orthodontics and Dentofacial Orthopedics.
White
Oak
Orthodontic
Products.
(2013).
Force
gauge
dynamometer.
Retrieved
from
http://www.whiteoakorthodontics.com/instruments/in-ha-force-guage-dynamometer.html
Ren, Y., Maltha, J., Vant Hof, M., and Kuijpers-Jagtman, A. (2004). Optimum force magnitude for orthodontic tooth movement: a
mathematical model. Am J Orthod Dentofacial Orthop. 125(1):71-7.
Krishnan, V., and Davidovitch, Z. (2015). Biological Mechanisms of Tooth Movement. 2 nd ed., Wiley Blackwell.
Ren, Y., Maltha, J., Vant Hof, M., and Kuijpers-Jagtman, A. (2003). Optimum force magnitude for orthodontic tooth movement: a
systematic literature review. Angle Orthod. (1):86-92.
DOI: 10.9790/0661-17540106
www.iosrjournals.org
6 | Page
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Conflict WaiverDocument2 pagesConflict WaiverjlurosNo ratings yet
- 950 MW Coal Fired Power Plant DesignDocument78 pages950 MW Coal Fired Power Plant DesignJohn Paul Coñge Ramos0% (1)
- Canopy CountersuitDocument12 pagesCanopy CountersuitJohn ArchibaldNo ratings yet
- IEEE Conference Template ExampleDocument14 pagesIEEE Conference Template ExampleEmilyNo ratings yet
- "I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweDocument5 pages"I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweInternational Organization of Scientific Research (IOSR)No ratings yet
- Socio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanDocument7 pagesSocio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanInternational Organization of Scientific Research (IOSR)No ratings yet
- Attitude and Perceptions of University Students in Zimbabwe Towards HomosexualityDocument5 pagesAttitude and Perceptions of University Students in Zimbabwe Towards HomosexualityInternational Organization of Scientific Research (IOSR)No ratings yet
- A Review of Rural Local Government System in Zimbabwe From 1980 To 2014Document15 pagesA Review of Rural Local Government System in Zimbabwe From 1980 To 2014International Organization of Scientific Research (IOSR)No ratings yet
- The Role of Extrovert and Introvert Personality in Second Language AcquisitionDocument6 pagesThe Role of Extrovert and Introvert Personality in Second Language AcquisitionInternational Organization of Scientific Research (IOSR)No ratings yet
- Assessment of The Implementation of Federal Character in Nigeria.Document5 pagesAssessment of The Implementation of Federal Character in Nigeria.International Organization of Scientific Research (IOSR)No ratings yet
- A Proposed Framework On Working With Parents of Children With Special Needs in SingaporeDocument7 pagesA Proposed Framework On Working With Parents of Children With Special Needs in SingaporeInternational Organization of Scientific Research (IOSR)No ratings yet
- Comparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesDocument7 pagesComparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesInternational Organization of Scientific Research (IOSR)No ratings yet
- Investigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehDocument4 pagesInvestigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehInternational Organization of Scientific Research (IOSR)No ratings yet
- The Impact of Technologies On Society: A ReviewDocument5 pagesThe Impact of Technologies On Society: A ReviewInternational Organization of Scientific Research (IOSR)100% (1)
- Edward Albee and His Mother Characters: An Analysis of Selected PlaysDocument5 pagesEdward Albee and His Mother Characters: An Analysis of Selected PlaysInternational Organization of Scientific Research (IOSR)No ratings yet
- An Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyDocument14 pagesAn Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyInternational Organization of Scientific Research (IOSR)No ratings yet
- Designing of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesDocument5 pagesDesigning of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesIOSRjournalNo ratings yet
- Topic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshDocument7 pagesTopic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshInternational Organization of Scientific Research (IOSR)No ratings yet
- Relationship Between Social Support and Self-Esteem of Adolescent GirlsDocument5 pagesRelationship Between Social Support and Self-Esteem of Adolescent GirlsInternational Organization of Scientific Research (IOSR)No ratings yet
- Importance of Mass Media in Communicating Health Messages: An AnalysisDocument6 pagesImportance of Mass Media in Communicating Health Messages: An AnalysisInternational Organization of Scientific Research (IOSR)No ratings yet
- Role of Madarsa Education in Empowerment of Muslims in IndiaDocument6 pagesRole of Madarsa Education in Empowerment of Muslims in IndiaInternational Organization of Scientific Research (IOSR)No ratings yet
- Different Software Life Cycle Models: Mini Project OnDocument11 pagesDifferent Software Life Cycle Models: Mini Project OnSagar MurtyNo ratings yet
- Guidelines Use of The Word AnzacDocument28 pagesGuidelines Use of The Word AnzacMichael SmithNo ratings yet
- Bismillah SpeechDocument2 pagesBismillah SpeechanggiNo ratings yet
- La Salle Lipa Integrated School Senior High School Community 1 Quarter Summative Assessment Earth Science AY 2021-2022 Household Conservation PlanDocument4 pagesLa Salle Lipa Integrated School Senior High School Community 1 Quarter Summative Assessment Earth Science AY 2021-2022 Household Conservation PlanKarlle ObviarNo ratings yet
- CT018 3 1itcpDocument31 pagesCT018 3 1itcpraghav rajNo ratings yet
- PovidoneDocument2 pagesPovidoneElizabeth WalshNo ratings yet
- Codex Standard EnglishDocument4 pagesCodex Standard EnglishTriyaniNo ratings yet
- ISP Flash Microcontroller Programmer Ver 3.0: M Asim KhanDocument4 pagesISP Flash Microcontroller Programmer Ver 3.0: M Asim KhanSrđan PavićNo ratings yet
- Descriptive Statistics - SPSS Annotated OutputDocument13 pagesDescriptive Statistics - SPSS Annotated OutputLAM NGUYEN VO PHINo ratings yet
- Understanding Consumer and Business Buyer BehaviorDocument47 pagesUnderstanding Consumer and Business Buyer BehaviorJia LeNo ratings yet
- Pega AcademyDocument10 pagesPega AcademySasidharNo ratings yet
- Review of Accounting Process 1Document2 pagesReview of Accounting Process 1Stacy SmithNo ratings yet
- Shopnil Tower 45KVA EicherDocument4 pagesShopnil Tower 45KVA EicherBrown builderNo ratings yet
- Unit 13 - Business Hotels and Sales ConferencesDocument24 pagesUnit 13 - Business Hotels and Sales ConferencesMiguel Angel Escoto CanoNo ratings yet
- ELC Work DescriptionDocument36 pagesELC Work DescriptionHari100% (1)
- Case Notes All Cases Family II TermDocument20 pagesCase Notes All Cases Family II TermRishi Aneja100% (1)
- Between:-Mr. Pedro Jose de Vasconcelos, of Address 14 CrombieDocument2 pagesBetween:-Mr. Pedro Jose de Vasconcelos, of Address 14 Crombiednd offiNo ratings yet
- Aman 5Document1 pageAman 5HamidNo ratings yet
- Soneri Bank Compensation PolicyDocument20 pagesSoneri Bank Compensation PolicySapii Mandhan100% (1)
- Business Testimony 3Document14 pagesBusiness Testimony 3Sapan BanerjeeNo ratings yet
- Service ManualDocument30 pagesService ManualYoni CativaNo ratings yet
- V Series: Three Wheel, Counterbalanced Lift TruckDocument126 pagesV Series: Three Wheel, Counterbalanced Lift TruckВиктор МушкинNo ratings yet
- CNG Fabrication Certificate16217Document1 pageCNG Fabrication Certificate16217pune2019officeNo ratings yet
- Audit Certificate: (On Chartered Accountant Firm's Letter Head)Document3 pagesAudit Certificate: (On Chartered Accountant Firm's Letter Head)manjeet mishraNo ratings yet
- List of People in Playboy 1953Document57 pagesList of People in Playboy 1953Paulo Prado De Medeiros100% (1)
- Jetweigh BrochureDocument7 pagesJetweigh BrochureYudi ErwantaNo ratings yet