You might also like
- When You Tell Me That Ou Love MeDocument2 pagesWhen You Tell Me That Ou Love Merahmawati aliwarmanNo ratings yet
- Westlife - My Love Song LyricsDocument2 pagesWestlife - My Love Song LyricsBuddy ArifNo ratings yet
- CREZIERDocument1 pageCREZIERrahmawati aliwarmanNo ratings yet
- F24 - Epilepsy After StrokeDocument6 pagesF24 - Epilepsy After StrokeplocnicuNo ratings yet
- JCN 11 E34Document8 pagesJCN 11 E34kakarafnieNo ratings yet
- What Is RH IncompatibilityDocument30 pagesWhat Is RH Incompatibilityrahmawati aliwarmanNo ratings yet
- Facts About Chikungunya17806 PDFDocument6 pagesFacts About Chikungunya17806 PDFNitin NaharNo ratings yet
- Without You (Reference Vocal) : Posting Lirik Ini Di Blog AndaDocument1 pageWithout You (Reference Vocal) : Posting Lirik Ini Di Blog Andarahmawati aliwarmanNo ratings yet
- All by MyselfDocument2 pagesAll by Myselfrahmawati aliwarmanNo ratings yet
- Bhattacharyya BPPV CPGDocument35 pagesBhattacharyya BPPV CPGrahmawati aliwarmanNo ratings yet
- 10 5923 J Ajdv 20150403 01Document3 pages10 5923 J Ajdv 20150403 01rahmawati aliwarmanNo ratings yet
- Vertigo diagnosis and management in primary careDocument3 pagesVertigo diagnosis and management in primary careAacg MeryendNo ratings yet
- Health Panel Seeks Sweeping Changes in Fertility TherapyDocument4 pagesHealth Panel Seeks Sweeping Changes in Fertility Therapyrahmawati aliwarmanNo ratings yet
- All by MyselfDocument2 pagesAll by Myselfrahmawati aliwarmanNo ratings yet
- Desviat 2006 CcaDocument4 pagesDesviat 2006 Ccarahmawati aliwarmanNo ratings yet
- True Vertigo Patients in Emergency Department An Epidemiologic StudyDocument4 pagesTrue Vertigo Patients in Emergency Department An Epidemiologic Studyrahmawati aliwarmanNo ratings yet
- 38 Acne PDFDocument7 pages38 Acne PDFRamadhan Harya Puja KusumaNo ratings yet
- JCN 11 262Document6 pagesJCN 11 262rahmawati aliwarmanNo ratings yet
- Histamine Antagonists For Treatment of Peripheral Vertigo: A Meta-AnalysisDocument5 pagesHistamine Antagonists For Treatment of Peripheral Vertigo: A Meta-Analysisrahmawati aliwarmanNo ratings yet
- Pi Is 0002934300004125Document8 pagesPi Is 0002934300004125rahmawati aliwarmanNo ratings yet
- 1 SS Skin Cancer - Chapter 1Document12 pages1 SS Skin Cancer - Chapter 1Muhammad IqbalNo ratings yet
- The Analysis of The Mycobacterium Leprae Resistance Against Ofloxacin After The Rifampicin Ofloxacin Minocycline (ROM) TherapyDocument5 pagesThe Analysis of The Mycobacterium Leprae Resistance Against Ofloxacin After The Rifampicin Ofloxacin Minocycline (ROM) Therapyrahmawati aliwarmanNo ratings yet
- Sel KeratinositDocument6 pagesSel KeratinositChristover Firstnando Saragih SimarmataNo ratings yet
- MelasmaDocument5 pagesMelasmarahmawati aliwarmanNo ratings yet
- Human SkinDocument15 pagesHuman Skinrahmawati aliwarmanNo ratings yet
- Bawang Ke SaDocument14 pagesBawang Ke SaDyah Anugrah KiranaNo ratings yet
- J. Nutr.-1992-Yamamoto-871-7Document7 pagesJ. Nutr.-1992-Yamamoto-871-7rahmawati aliwarmanNo ratings yet
- Should We Use Ceftriaxone To Treat Staphylococcal.2Document2 pagesShould We Use Ceftriaxone To Treat Staphylococcal.2rahmawati aliwarmanNo ratings yet
- 5 and Type 8 Capsular Polysaccharides by Type Regulation Of: Staphylococcus AureusDocument6 pages5 and Type 8 Capsular Polysaccharides by Type Regulation Of: Staphylococcus Aureusrahmawati aliwarmanNo ratings yet
- Correspondence: Methicillin-Resistant Staphylococcus Aureus Clinical Strain With Reduced Vancomycin SusceptibilityDocument12 pagesCorrespondence: Methicillin-Resistant Staphylococcus Aureus Clinical Strain With Reduced Vancomycin Susceptibilityrahmawati aliwarmanNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
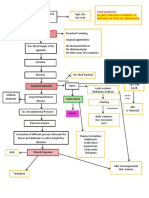
- CPC - Appendicitis (Flowchart)Document1 pageCPC - Appendicitis (Flowchart)Milet NacionalesNo ratings yet
- 5 Minute Fluency - Volume IDocument79 pages5 Minute Fluency - Volume IAlexandre Magno AlvesNo ratings yet
- Test Questionnaire For Needs AnalysisDocument5 pagesTest Questionnaire For Needs AnalysisYenyen Quirog-PalmesNo ratings yet
- Journal Pone 0118161Document10 pagesJournal Pone 0118161David PesireronNo ratings yet
- (Coll.) WHO Classification of Head and Neck Tumour (B-Ok - Xyz)Document285 pages(Coll.) WHO Classification of Head and Neck Tumour (B-Ok - Xyz)Andrea GonzalezNo ratings yet
- ĐỀ 26Document6 pagesĐỀ 26Uyên Lê PhươngNo ratings yet
- Manual of Cardio-Oncology - Cardiovascular Care in The Cancer Patient (PDFDrive)Document472 pagesManual of Cardio-Oncology - Cardiovascular Care in The Cancer Patient (PDFDrive)jimurgaNo ratings yet
- Nursing Management: Nursing Management: Acute Kidney Injury and Chronic Kidney DiseaseDocument22 pagesNursing Management: Nursing Management: Acute Kidney Injury and Chronic Kidney Diseasedian rachmat saputroNo ratings yet
- Adult Acute Lymphoblastic LeukemiaDocument22 pagesAdult Acute Lymphoblastic Leukemiamelki hadisasmitaNo ratings yet
- LiliDocument7 pagesLilialan azizNo ratings yet
- A Case Study On Breast Cancer (2003)Document58 pagesA Case Study On Breast Cancer (2003)Katty Rine100% (6)
- Adrenal Function Urine Test ExplainedDocument30 pagesAdrenal Function Urine Test ExplainedDamarys ReyesNo ratings yet
- Philippine Music and Arts QuizDocument4 pagesPhilippine Music and Arts Quizrizabesmonte100% (1)
- Seed Rotation Ebook Final 2Document10 pagesSeed Rotation Ebook Final 2Andreea Cretiu100% (3)
- Veterinary Surgery and Radiology MCQDocument66 pagesVeterinary Surgery and Radiology MCQJihad Anad81% (59)
- AmebaDocument21 pagesAmebamihaelaemma100% (2)
- Report On KhatDocument13 pagesReport On KhatYounas BhattiNo ratings yet
- Serenoa Repens (Saw Palmetto) A Systematic Review of Adverse EventsDocument11 pagesSerenoa Repens (Saw Palmetto) A Systematic Review of Adverse EventsAdam ZhangNo ratings yet
- Neoplasia Outline Notes - PathologyDocument4 pagesNeoplasia Outline Notes - Pathologykep1313No ratings yet
- Female Genital Cysts Tract PDFDocument6 pagesFemale Genital Cysts Tract PDFRaraNo ratings yet
- The Histological Aspects of Fillers Complications: Ute S. Zimmermann, MD, and Thierry J. Clerici, MDDocument10 pagesThe Histological Aspects of Fillers Complications: Ute S. Zimmermann, MD, and Thierry J. Clerici, MDMichele CarvalhoNo ratings yet
- DR J GowingDocument2 pagesDR J GowingkaylekayprNo ratings yet
- INTUSSUSCEPTIONDocument1 pageINTUSSUSCEPTIONMaecy PasionNo ratings yet
- Diabetes Mellitus Part 1 - Prof - AskandarDocument40 pagesDiabetes Mellitus Part 1 - Prof - AskandarAdekresnaHernataNo ratings yet
- The detection of Bence Jones protein in urine by the heat test helps in diagnosis of multiple myelomaDocument4 pagesThe detection of Bence Jones protein in urine by the heat test helps in diagnosis of multiple myelomaCarla PereiraNo ratings yet
- RACGP - Bones and JointsDocument31 pagesRACGP - Bones and JointstjelongNo ratings yet
- Medical TerminologyDocument47 pagesMedical TerminologyGina Andinia AzizahNo ratings yet
- Zebra XX, Part 2 PDFDocument3 pagesZebra XX, Part 2 PDFRamona MateiNo ratings yet