You might also like
- Jensen JE-990 Opamp JAES Reprint 1980 PDFDocument10 pagesJensen JE-990 Opamp JAES Reprint 1980 PDFrogerlapinNo ratings yet
- Easy(er) Electrical Principles for General Class Ham License (2019-2023)From EverandEasy(er) Electrical Principles for General Class Ham License (2019-2023)No ratings yet
- ABB HV Shunt ReactorDocument30 pagesABB HV Shunt Reactortkdrt2166100% (1)
- Control Engineering April 12Document72 pagesControl Engineering April 12Mauro SánchezNo ratings yet
- Measuring Output Transformer PerformanceDocument8 pagesMeasuring Output Transformer PerformanceJonathon Diaz100% (1)
- Light Triggering Thyristor For HVDC and Other Applications.Document6 pagesLight Triggering Thyristor For HVDC and Other Applications.IDESNo ratings yet
- Basic Calculation of A Boost Converter's Power StageDocument9 pagesBasic Calculation of A Boost Converter's Power Stagexuanvan1303No ratings yet
- CHAPTER 2 (Autosaved)Document76 pagesCHAPTER 2 (Autosaved)dray09100% (1)
- Ieee 1584 - 2002 Incident Energy Factors and Simple 480 V Incident Energyb Equations PDFDocument9 pagesIeee 1584 - 2002 Incident Energy Factors and Simple 480 V Incident Energyb Equations PDFRicardo CardonaNo ratings yet
- PAPER 2003 03 en HV Shunt Reactor Secrets For Protection EngineersDocument30 pagesPAPER 2003 03 en HV Shunt Reactor Secrets For Protection Engineerslamugre20003506No ratings yet
- Engineering Method For Calculation of Short-CircuitDocument7 pagesEngineering Method For Calculation of Short-CircuitnicklionsNo ratings yet
- Automatic Phase ChangerDocument55 pagesAutomatic Phase ChangerGanpati Kucheria75% (4)
- The K FactorDocument11 pagesThe K FactorSOURAV PRASADNo ratings yet
- Paper - An Electric Fence Energizer Design MethodDocument6 pagesPaper - An Electric Fence Energizer Design MethodMaria G AnimalistaNo ratings yet
- Ferroresonance VT Gis v002Document4 pagesFerroresonance VT Gis v002qais652002No ratings yet
- Electricity Booklet IGCSE 1.0Document45 pagesElectricity Booklet IGCSE 1.0Fiona YoungNo ratings yet
- 60 HZ Interference in ElectrocardiographyDocument11 pages60 HZ Interference in Electrocardiographyjhon123scribdNo ratings yet
- Nalula Exp7 PDFDocument18 pagesNalula Exp7 PDFHero CourseNo ratings yet
- I, and I, and Zref Separately We Measured Changes of AboutDocument5 pagesI, and I, and Zref Separately We Measured Changes of AboutBodhayan PrasadNo ratings yet
- Design of Dynamic Frequency Divider Using NegativeDocument5 pagesDesign of Dynamic Frequency Divider Using NegativeEditor IJRITCCNo ratings yet
- Dual-Frequency Modified C/V Technique: 150 125 100 7 5 1 50 25 / I 15MW/600nmDocument2 pagesDual-Frequency Modified C/V Technique: 150 125 100 7 5 1 50 25 / I 15MW/600nmkurabyqldNo ratings yet
- 05735442Document2 pages05735442kothari_rubinNo ratings yet
- Single Electron Based Binary Multipliers With Overflow DetectionDocument13 pagesSingle Electron Based Binary Multipliers With Overflow Detectionprabhjot singh1No ratings yet
- Voltage Divider Circuit ExperimentDocument11 pagesVoltage Divider Circuit ExperimentLorshiel Anne TusingNo ratings yet
- Current/Voltage Measurement Scheme Using A Flexible Coil/Electrode Power Sensor To Monitor The Power of Two-Wired Household AppliancesDocument11 pagesCurrent/Voltage Measurement Scheme Using A Flexible Coil/Electrode Power Sensor To Monitor The Power of Two-Wired Household AppliancesInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- IEEE - 2006 - Degen and Jackel - A Pseudodiffer Amp For Bioelectric Events With DC Offset Compensation Using Two Wired Amplifying ElectrodesDocument11 pagesIEEE - 2006 - Degen and Jackel - A Pseudodiffer Amp For Bioelectric Events With DC Offset Compensation Using Two Wired Amplifying ElectrodesshreypathakNo ratings yet
- Impact of Variable Switching Frequency Over Power Loss On Converter TopologiesDocument6 pagesImpact of Variable Switching Frequency Over Power Loss On Converter TopologiesskrtamilNo ratings yet
- 65 Caprio ElecLett 1973Document2 pages65 Caprio ElecLett 1973kurabyqldNo ratings yet
- LVDT and Capacitance Strain GuagesDocument13 pagesLVDT and Capacitance Strain GuagesJignesh P Korat100% (1)
- BBEE203 Module 5 StudentsDocument35 pagesBBEE203 Module 5 StudentsshilpaNo ratings yet
- V2I300142Document3 pagesV2I300142editor_ijarcsseNo ratings yet
- Prepared by The Education and Student Activities Committee of The IEEE EMC SocietyDocument8 pagesPrepared by The Education and Student Activities Committee of The IEEE EMC Societymaku lulajNo ratings yet
- Circuit Design Techniques for Linear Integrated CircuitsDocument5 pagesCircuit Design Techniques for Linear Integrated CircuitsNoita EnolaNo ratings yet
- Electronics 08 01137 v2Document14 pagesElectronics 08 01137 v2sigit kurniawanNo ratings yet
- The Design and Construction of A 1kva Inverter 49596Document11 pagesThe Design and Construction of A 1kva Inverter 49596Emmanuel KutaniNo ratings yet
- International Journal of Electronics and Communications (AEÜ)Document12 pagesInternational Journal of Electronics and Communications (AEÜ)RajeeNo ratings yet
- Chapter 03Document5 pagesChapter 03api-285133030No ratings yet
- Simple PotentiostatDocument3 pagesSimple PotentiostatguiburNo ratings yet
- Analog Electronic WattmetrDocument2 pagesAnalog Electronic WattmetrKaran AnejaNo ratings yet
- A Three Phase Transformer Modelling For Distribution System: Department of Electrical and ElectronicsDocument6 pagesA Three Phase Transformer Modelling For Distribution System: Department of Electrical and ElectronicsrahulNo ratings yet
- Wideband Resistive Voltage Divider For A Standard Wattmeter: Journal of Physics: Conference SeriesDocument8 pagesWideband Resistive Voltage Divider For A Standard Wattmeter: Journal of Physics: Conference SeriesAngel SamanthaNo ratings yet
- Voltage Dip's Mitigation During PV-Grid-Connection Using STATCOMDocument7 pagesVoltage Dip's Mitigation During PV-Grid-Connection Using STATCOMMohammedSaeedNo ratings yet
- Fayako Rapor 8Document10 pagesFayako Rapor 8Eren YükselNo ratings yet
- Exp 02Document10 pagesExp 02mohammeda AlmaitahNo ratings yet
- Fully Integrated Power Supply Design For Wireless Biomedical ImplantsDocument6 pagesFully Integrated Power Supply Design For Wireless Biomedical ImplantsDon ReloNo ratings yet
- 29-04-2021-1619695048-6-Ijeee-2. Ijeee - Power Quality Improvement Using Fuzzy Based StatcomDocument10 pages29-04-2021-1619695048-6-Ijeee-2. Ijeee - Power Quality Improvement Using Fuzzy Based Statcomiaset123No ratings yet
- Bilotti 1966Document3 pagesBilotti 1966dycsteiznNo ratings yet
- Coated Electrode Manual-Metal Arc Welding With High Frequency Welding Inverter Power SourcesDocument6 pagesCoated Electrode Manual-Metal Arc Welding With High Frequency Welding Inverter Power Sourcessapreswapnil8388No ratings yet
- Hu Melvyl 99 25Document5 pagesHu Melvyl 99 25Mouna RobertoNo ratings yet
- Shell Electrical Engineer HandbookDocument16 pagesShell Electrical Engineer Handbookimemyself009No ratings yet
- Familiarization of The Electrical Machine Laboratory ApparatusDocument5 pagesFamiliarization of The Electrical Machine Laboratory ApparatusRosalinda CondeNo ratings yet
- Curve Tracer PDFDocument8 pagesCurve Tracer PDFurenhu9970100% (2)
- Arcing-Fault Models For Low Voltage Power SystemsDocument8 pagesArcing-Fault Models For Low Voltage Power Systemsautomation vguardNo ratings yet
- Inverter Lifetime PhotovoltaicDocument6 pagesInverter Lifetime Photovoltaicescuadrian9043No ratings yet
- Lab Report 1. Diode Characteristics HalfDocument10 pagesLab Report 1. Diode Characteristics HalfayasumireNo ratings yet
- Libro2 PDocument6 pagesLibro2 PJose Luis Arellano CamachoNo ratings yet
- Analisa Kesalahan Pemasangan Grounding Pada KWH Meter PrabayarDocument12 pagesAnalisa Kesalahan Pemasangan Grounding Pada KWH Meter Prabayarmamai nebeNo ratings yet
- Ee6701 Hve Eee Viist Au Unit VDocument19 pagesEe6701 Hve Eee Viist Au Unit VGeorge CietNo ratings yet
- Modeling of Coplanar Waveguide Meander-LineInductorsDocument10 pagesModeling of Coplanar Waveguide Meander-LineInductorsalisazidNo ratings yet
- Mirrored Coupling Structures For Microwave Signal Splitting and Combining PDFDocument6 pagesMirrored Coupling Structures For Microwave Signal Splitting and Combining PDFagmnm1962No ratings yet
- SP 500 SpecDocument2 pagesSP 500 Specagmnm1962No ratings yet
- 12 G To 20 G Compact Rectangle Waveguide To Circular Waveguide Mode ConvertorDocument2 pages12 G To 20 G Compact Rectangle Waveguide To Circular Waveguide Mode Convertoragmnm1962No ratings yet
- Broadband Lumped-Element Integrated - Way Power Dividers For Voltage StandardsDocument9 pagesBroadband Lumped-Element Integrated - Way Power Dividers For Voltage Standardsagmnm1962No ratings yet
- MRF 175 GVDocument1 pageMRF 175 GVagmnm1962No ratings yet
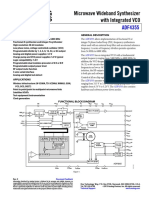
- ADF4355 54-6800 MHZ Microwave Wideband Synthesizer With Integrated VCODocument35 pagesADF4355 54-6800 MHZ Microwave Wideband Synthesizer With Integrated VCOagmnm1962No ratings yet
- ACS712 Demo Board Guide PDFDocument11 pagesACS712 Demo Board Guide PDFagmnm1962No ratings yet
- High Power CombinerDocument5 pagesHigh Power Combineragmnm1962No ratings yet
- 51W 10540 1Document16 pages51W 10540 1Mitrofan AnduNo ratings yet
- Patch Antenna Design MAnualDocument36 pagesPatch Antenna Design MAnualkarthikvel_852246No ratings yet
- A Compact Ultra-Wideband Power Divider With High Isolation 3.1-10.6 GHZDocument2 pagesA Compact Ultra-Wideband Power Divider With High Isolation 3.1-10.6 GHZagmnm1962No ratings yet
- 200watt Active Load UnitDocument14 pages200watt Active Load Unitagmnm1962No ratings yet
- A Novel Wideband Bandpass Power Divider With Harmonic Suppressed Ring Resonator 1.41-2.68 GHZDocument4 pagesA Novel Wideband Bandpass Power Divider With Harmonic Suppressed Ring Resonator 1.41-2.68 GHZagmnm1962No ratings yet
- AN5142 Radio Link-Budget Calculations For ISM-RF ProductsDocument11 pagesAN5142 Radio Link-Budget Calculations For ISM-RF Productsagmnm1962No ratings yet
- DB3 DB4 SMDB3 - Diac PDFDocument6 pagesDB3 DB4 SMDB3 - Diac PDFmsicoie1851No ratings yet
- C106BOS Datasheetz PDFDocument6 pagesC106BOS Datasheetz PDFAnonymous na7OSZaNo ratings yet
- Tipl762 - NPN Silicon Power TransistorsDocument7 pagesTipl762 - NPN Silicon Power Transistorsagmnm1962No ratings yet
- Scr's & Triacs Cross ReferenceDocument11 pagesScr's & Triacs Cross Referenceagmnm1962No ratings yet
- Sprabw0b PDFDocument19 pagesSprabw0b PDFAshok KumarNo ratings yet
- Variable High Voltage BJT Regulator User ManualDocument7 pagesVariable High Voltage BJT Regulator User Manualagmnm1962No ratings yet
- SP431 Adjustable Precision RegulatorsDocument11 pagesSP431 Adjustable Precision Regulatorsagmnm1962No ratings yet
- Data Sheet: UHF Push-Pull Power MOS TransistorDocument15 pagesData Sheet: UHF Push-Pull Power MOS Transistoragmnm1962No ratings yet
- tl783 PDFDocument26 pagestl783 PDFLuiz CaldeiraNo ratings yet
- Testing A Power Supply For Line and Load TransientsDocument7 pagesTesting A Power Supply For Line and Load Transientsagmnm1962No ratings yet
- Creating A Fast Load TransientDocument3 pagesCreating A Fast Load Transientagmnm1962No ratings yet
- Pads WhitepaperDocument23 pagesPads Whitepaperagmnm1962No ratings yet
- Design of a 2.5kW isolated DC/DC fullbridge converter for electric vehicle applicationDocument55 pagesDesign of a 2.5kW isolated DC/DC fullbridge converter for electric vehicle applicationmarconi-agNo ratings yet
- LXA-7500 Series X-Band Low Noise AmplifiersDocument4 pagesLXA-7500 Series X-Band Low Noise Amplifiersagmnm1962No ratings yet
- A Review of Implantable Antennas For Wireless Biomedical DevicesDocument11 pagesA Review of Implantable Antennas For Wireless Biomedical Devicesagmnm1962No ratings yet
- Gain Margin and Phase Margin Physical MeaningDocument2 pagesGain Margin and Phase Margin Physical MeaningSaad MemonNo ratings yet
- Switch-Mode Power Converter Compensation Made Easy: Robert SheehanDocument38 pagesSwitch-Mode Power Converter Compensation Made Easy: Robert Sheehanjimmyboy111No ratings yet
- L420 OpAmpCompIDocument14 pagesL420 OpAmpCompIShreerama Samartha G BhattaNo ratings yet
- Designing DC/DC converters with Si9110 switchmode controllerDocument19 pagesDesigning DC/DC converters with Si9110 switchmode controllerLiem NguyenNo ratings yet
- Opamp ProjectDocument10 pagesOpamp Projectbirla_sNo ratings yet
- Overshoot As A Function of Phase MarginDocument4 pagesOvershoot As A Function of Phase MarginJayesh PatilNo ratings yet
- 1028 FBDocument28 pages1028 FBNguyễn Trung ThaoNo ratings yet
- Control SystemsDocument8 pagesControl SystemsprakashjntuNo ratings yet
- EC2255 Control Systems Question BankDocument62 pagesEC2255 Control Systems Question BankreporterrajiniNo ratings yet
- Ti Tl972-q1 Rail-To-rail Output, Very Low-Noise Operational AmplifiersDocument20 pagesTi Tl972-q1 Rail-To-rail Output, Very Low-Noise Operational Amplifiersyura yuraNo ratings yet
- Cooperative Control Multi Master Slave MicrogridsDocument12 pagesCooperative Control Multi Master Slave Microgridsali jafarianNo ratings yet
- Applications FeaturesDocument12 pagesApplications FeatureseduardofelisNo ratings yet
- Class-D Audio II Evaluation Board (HIP4080AEVAL2)Document16 pagesClass-D Audio II Evaluation Board (HIP4080AEVAL2)Enos Marcos BastosNo ratings yet
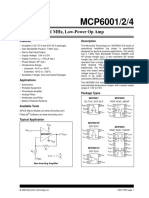
- 2.5V To 6.0V Micropower CMOS Op Amp: FeaturesDocument32 pages2.5V To 6.0V Micropower CMOS Op Amp: FeaturesJuan Carlos Ramirez FuentesNo ratings yet
- DatasheetDocument28 pagesDatasheetKevin AlegreNo ratings yet
- Half-Bridge Bidirectional DC-DC Converter For Small Electric VehicleDocument5 pagesHalf-Bridge Bidirectional DC-DC Converter For Small Electric VehiclePradeepChandraVarmaMandapati100% (1)
- The Recycling Folded Cascode A General Enhancement of The Folded Cascode AmplifierDocument8 pagesThe Recycling Folded Cascode A General Enhancement of The Folded Cascode AmplifierAyanabho BanerjeeNo ratings yet
- Tps 54231Document31 pagesTps 54231pvickyNo ratings yet
- KFlopManual PDFDocument306 pagesKFlopManual PDFandrea772No ratings yet
- EL2020Document14 pagesEL2020api-3825669No ratings yet
- Ec 614Document89 pagesEc 614Akash yadavNo ratings yet
- LINEAR INTEGRATED CIRCUITS Unit3 Raghudathesh VTUDocument30 pagesLINEAR INTEGRATED CIRCUITS Unit3 Raghudathesh VTUraghudatheshNo ratings yet
- Control System Design by Frequency ResponseDocument8 pagesControl System Design by Frequency ResponseSatyamGuptaNo ratings yet
- D D D D D D D D: TLV4110, TLV4111, TLV4112, TLV4113 Family of High Output Drive Operational Amplifiers With ShutdownDocument21 pagesD D D D D D D D: TLV4110, TLV4111, TLV4112, TLV4113 Family of High Output Drive Operational Amplifiers With ShutdownAndrew AguilarNo ratings yet
- Control Loop Cookbook PDFDocument27 pagesControl Loop Cookbook PDFDmytro RakNo ratings yet
- MECN5015A - Chapter 5 - Lecture SLidesDocument36 pagesMECN5015A - Chapter 5 - Lecture SLidesGulain MayomboNo ratings yet