You might also like
- NOAC ChartDocument2 pagesNOAC Chartsgod34No ratings yet
- Laparoscopic Peritoneal Entry TechniquesDocument52 pagesLaparoscopic Peritoneal Entry Techniquessgod34100% (1)
- Nutrition Support: Sean P Harbison MDDocument42 pagesNutrition Support: Sean P Harbison MDsgod34No ratings yet
- Modes of Mechanical VentilationDocument4 pagesModes of Mechanical Ventilationsgod34100% (1)
- Resident Rotation Schedule 2015-16 - FinalDocument14 pagesResident Rotation Schedule 2015-16 - Finalsgod34No ratings yet
- Abdominal InfectionsDocument6 pagesAbdominal InfectionsPatrico Rillah SetiawanNo ratings yet
- Surgery Preround Template SkeletonDocument2 pagesSurgery Preround Template Skeletonsgod34No ratings yet
- 2012 KevinSextonMay2 BC Wound HealingDocument40 pages2012 KevinSextonMay2 BC Wound HealingYulinda PrimilisaNo ratings yet
- Espinal STS PDFDocument2 pagesEspinal STS PDFsgod34No ratings yet
- Espinal STSDocument2 pagesEspinal STSsgod34No ratings yet
- Nadelman STSDocument2 pagesNadelman STSsgod34No ratings yet
- Basic Ventilator y ModesDocument47 pagesBasic Ventilator y ModesAlina VanceaNo ratings yet
- Venous DiseaseDocument50 pagesVenous Diseasesgod34No ratings yet
- Venous Disorder - GodelmanDocument27 pagesVenous Disorder - Godelmansgod34No ratings yet
- Master Schedule 10-22Document65 pagesMaster Schedule 10-22sgod34No ratings yet
- Abnormal LFTs in General PracticeDocument57 pagesAbnormal LFTs in General Practicesgod34No ratings yet
- Veins More DistensibleDocument27 pagesVeins More Distensiblesgod34No ratings yet
- Lecture 5 Vascular Disorders StudentsDocument103 pagesLecture 5 Vascular Disorders Studentssgod34No ratings yet
- Endoscopy TechniqueDocument8 pagesEndoscopy Techniquesgod34No ratings yet
- 7 MedEd Vascular Jonny Hodgkinson 12.11.12 1Document35 pages7 MedEd Vascular Jonny Hodgkinson 12.11.12 1sgod34No ratings yet
- HemostasisDocument38 pagesHemostasissgod34100% (1)
- ABSITE REVIEW: Vascular Cranial Nerves and Leg UlcersDocument183 pagesABSITE REVIEW: Vascular Cranial Nerves and Leg Ulcerssgod34No ratings yet
- Fluid Resucitation, 2015Document44 pagesFluid Resucitation, 2015sgod34No ratings yet
- ABX Dosing & RDocument11 pagesABX Dosing & Rsgod34No ratings yet
- Guidelines Management 2007w Bookmarks PDFDocument0 pagesGuidelines Management 2007w Bookmarks PDFdiaga081No ratings yet
- Colon CADocument16 pagesColon CAsgod34No ratings yet
- General Surgery - DR Tadros - CompressedDocument164 pagesGeneral Surgery - DR Tadros - Compressedsgod34No ratings yet
- Bile Duct Injuries: Dr. Joe M Das Junior Resident S3 UnitDocument149 pagesBile Duct Injuries: Dr. Joe M Das Junior Resident S3 Unitsgod34No ratings yet
- Anast Bleed MMDocument17 pagesAnast Bleed MMsgod34No ratings yet
- Bile Duct Injuries: Dr. Joe M Das Junior Resident S3 UnitDocument149 pagesBile Duct Injuries: Dr. Joe M Das Junior Resident S3 Unitsgod34No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Science Daily Test 1Document5 pagesScience Daily Test 1yuniNo ratings yet
- Acyanotic CHDDocument83 pagesAcyanotic CHDmrinmayee deshmukhNo ratings yet
- Right Sided Heart Failure Case 4.2Document4 pagesRight Sided Heart Failure Case 4.2Athari AdityaNo ratings yet
- Stroke and HypertensionDocument4 pagesStroke and HypertensionKhessie Laye Garcia JacintoNo ratings yet
- Cardiology: 27 Maret 2021Document52 pagesCardiology: 27 Maret 2021Dian ParamitaNo ratings yet
- Guide to Cardiac Exam Findings and DiagnosesDocument58 pagesGuide to Cardiac Exam Findings and Diagnoseseliaszavaleta100% (1)
- Cuarta Definicion de InfartoDocument41 pagesCuarta Definicion de InfartoJerax PNo ratings yet
- Icu Skills Assessment ExamDocument5 pagesIcu Skills Assessment ExamJona AureNo ratings yet
- 56 MediastinumDocument6 pages56 MediastinumRahmi Dwi AzkiahNo ratings yet
- Kasus Lain LainDocument14 pagesKasus Lain LainofislinNo ratings yet
- 2018 ESC-EACTS Guidelines On Myocardial RevascularizationDocument96 pages2018 ESC-EACTS Guidelines On Myocardial RevascularizationTony Miguel Saba SabaNo ratings yet
- Basic Life Support (BLS) : Franklin O. Que, BSN-RNDocument90 pagesBasic Life Support (BLS) : Franklin O. Que, BSN-RNfrank_1785No ratings yet
- Vital Signs ProcedureDocument10 pagesVital Signs ProcedureJojebelle Kate Iyog-cabanlet100% (3)
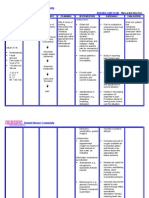
- Nursing Care Plan - Myocardial InfarctionDocument3 pagesNursing Care Plan - Myocardial Infarctionderic80% (10)
- Circulatory System Important Questions and AnswersDocument5 pagesCirculatory System Important Questions and Answerssamhi96No ratings yet
- Pathophysiology of Heart FailureDocument38 pagesPathophysiology of Heart FailureRizqy JoeandriNo ratings yet
- Advanced Cardiac Life Support AsystoleDocument14 pagesAdvanced Cardiac Life Support AsystoleKar TwentyfiveNo ratings yet
- Kanski's Clinical Ophthalmology A Systematic Approach by John SalmonDocument20 pagesKanski's Clinical Ophthalmology A Systematic Approach by John SalmonAliNo ratings yet
- Anatomi Organ DR - Siti Rafiah HusainDocument73 pagesAnatomi Organ DR - Siti Rafiah HusainfitrahfajrianihamingNo ratings yet
- ACS Case StudyDocument26 pagesACS Case StudyMari Lyn100% (1)
- IMELS New Approach in Basic Life SupportDocument28 pagesIMELS New Approach in Basic Life SupportAstri Arri FebriantiNo ratings yet
- Rheumatic Fever and Rheumatic Heart DiseaseDocument54 pagesRheumatic Fever and Rheumatic Heart DiseaseFian AldyNo ratings yet
- Amiodarone Hydro ChlorideDocument4 pagesAmiodarone Hydro Chlorideapi-3797941No ratings yet
- Occupational English Test: Writing Sub-Test: Nursing Time Allowed: Reading Time: 5 Minutes Writing Time: 40 MinutesDocument2 pagesOccupational English Test: Writing Sub-Test: Nursing Time Allowed: Reading Time: 5 Minutes Writing Time: 40 MinutesMathea Cohen0% (1)
- Ischaemic Heart DiseaseDocument23 pagesIschaemic Heart Diseasebrain bareNo ratings yet
- Cor Pulmonale: Definition, Causes, Symptoms & TreatmentDocument31 pagesCor Pulmonale: Definition, Causes, Symptoms & TreatmentAnjela BaidyaNo ratings yet
- Nursing Care of Patient With Cardiac ArrestDocument78 pagesNursing Care of Patient With Cardiac ArrestNurhamizah Abd hamidNo ratings yet
- Cardiovascular SystemDocument6 pagesCardiovascular Systemtasneem8No ratings yet
- Clinical Cardiology - April 1994 - Wareing - Cardiac Surgery 2nd Edition by John W Kirklin and Brian G Barratt BoyesDocument1 pageClinical Cardiology - April 1994 - Wareing - Cardiac Surgery 2nd Edition by John W Kirklin and Brian G Barratt BoyesOlga KochubeiNo ratings yet
- Study This Question Med Surg FinalDocument14 pagesStudy This Question Med Surg FinalAna Gonzalez83% (6)