You might also like
- Are All Stents EqualDocument3 pagesAre All Stents EqualZulkarnain MuinNo ratings yet
- Viability Study 2Document66 pagesViability Study 2berneNo ratings yet
- Protocol Template V1.0 040717Document65 pagesProtocol Template V1.0 040717ירדן לויןNo ratings yet
- Protocol Template Version 1.0 040717Document65 pagesProtocol Template Version 1.0 040717Abhishek Sharma / SAI CHEMPARTNERS100% (1)
- Point of Care DiagnosticsDocument109 pagesPoint of Care Diagnosticschhatra0% (1)
- Failure of MiniscrewsDocument24 pagesFailure of MiniscrewsMaha Ahmed SolimanNo ratings yet
- 12 Evidence Based Period Ontology Systematic ReviewsDocument17 pages12 Evidence Based Period Ontology Systematic ReviewsAparna PandeyNo ratings yet
- Analysis of Total Knee Arthroplasty Revision Causes: Researcharticle Open AccessDocument6 pagesAnalysis of Total Knee Arthroplasty Revision Causes: Researcharticle Open AccessCláudia SilvaNo ratings yet
- Challenges Writing Patient Safety NarrativesDocument4 pagesChallenges Writing Patient Safety Narrativessanjeeva reddyNo ratings yet
- Contemporary World - GlobalizationDocument5 pagesContemporary World - GlobalizationVjay AbendaNo ratings yet
- Allowable Strength DesignDocument5 pagesAllowable Strength DesignnvnrevNo ratings yet
- H59a SampleDocument14 pagesH59a SampleResidencia BioquímicaNo ratings yet
- Literature Review of Snomed CT UseDocument7 pagesLiterature Review of Snomed CT Useuziianwgf100% (1)
- 1 s2.0 S0889540612007536 MainDocument24 pages1 s2.0 S0889540612007536 MainPanaite TinelaNo ratings yet
- Protocol Template 05feb2016 508Document61 pagesProtocol Template 05feb2016 508Dawit Birhanu100% (1)
- Chapter 8Document50 pagesChapter 8Komal TalrejaNo ratings yet
- Jurnal Reading THTDocument7 pagesJurnal Reading THTSucii Sekar NingrumNo ratings yet
- EU CER WhitepaperDocument5 pagesEU CER Whitepaperibrahim kademogluNo ratings yet
- Technology Assessment of Innovative Medical Devices in EuropeDocument4 pagesTechnology Assessment of Innovative Medical Devices in EuropeMARIA JULIANA GONZALEZNo ratings yet
- Design and Manufacturing of Catheter Protector DeviceDocument6 pagesDesign and Manufacturing of Catheter Protector DeviceIJRASETPublicationsNo ratings yet
- Section Two - Evidence-Based Validation of Safety and EfficacyDocument17 pagesSection Two - Evidence-Based Validation of Safety and EfficacyKomal TalrejaNo ratings yet
- Apps To Help You Manage Your Ballya in Vitro Diagnostics Rapid Test ManufacturerDocument3 pagesApps To Help You Manage Your Ballya in Vitro Diagnostics Rapid Test ManufacturerdenopehecpNo ratings yet
- Reporting of Computational Modeling Studies in Medical Device Submissions Guidance For Industry and Food and Drug Administration StaffDocument48 pagesReporting of Computational Modeling Studies in Medical Device Submissions Guidance For Industry and Food and Drug Administration StaffAnonymous P8Bt46mk5INo ratings yet
- Clinical Literature Review Medical DevicesDocument5 pagesClinical Literature Review Medical Devicesea6p1e99100% (1)
- FDA Bone Anchor Testing GuidanceDocument7 pagesFDA Bone Anchor Testing GuidanceMarcelo Alves100% (1)
- USFDA On Stent UpdatesDocument10 pagesUSFDA On Stent UpdatesKarishmaNo ratings yet
- Cris Pautas IgualDocument5 pagesCris Pautas IgualcsalameaNo ratings yet
- In Vitro Diagnostic Creatinine Test System: Guidance For IndustryDocument5 pagesIn Vitro Diagnostic Creatinine Test System: Guidance For IndustryrajtanniruNo ratings yet
- Post-Market Surveillance - VigilanceDocument40 pagesPost-Market Surveillance - VigilanceSergio Mosa100% (1)
- 2016 TechnologyWatch Vol1Document27 pages2016 TechnologyWatch Vol1amit545No ratings yet
- 02 Handout HIV Test Kit Selection-Operational - Considerations-1Document4 pages02 Handout HIV Test Kit Selection-Operational - Considerations-1Amy TanNo ratings yet
- Development and Validation of A Paediatric Long-Bone Fracture Classification. A Prospective Multicentre Study in 13 European Paediatric Trauma CentresDocument13 pagesDevelopment and Validation of A Paediatric Long-Bone Fracture Classification. A Prospective Multicentre Study in 13 European Paediatric Trauma CentresArul WidyaNo ratings yet
- The Evolution of Car T-Cell Therapy: Ethics and EfficiencyDocument8 pagesThe Evolution of Car T-Cell Therapy: Ethics and EfficiencyIJAR JOURNALNo ratings yet
- Jaeger J1 EquivalentDocument2 pagesJaeger J1 EquivalentmukeshkbhattNo ratings yet
- Review of Literature On Health and Safety MeasuresDocument9 pagesReview of Literature On Health and Safety MeasuresfrqofvbndNo ratings yet
- The Impacts of Lead Time On Supply Chain Resilience in Medical Device IndustryDocument24 pagesThe Impacts of Lead Time On Supply Chain Resilience in Medical Device IndustryTrúc LoanNo ratings yet
- 10 1016@j Jebdp 2020 101402Document18 pages10 1016@j Jebdp 2020 101402ali asiriNo ratings yet
- Literature Review of Snomed CTDocument5 pagesLiterature Review of Snomed CTbav1dik0jal3100% (1)
- A Comprehensive Analysis of The Literature On The Impact of The Surgical Safety ChecklistDocument7 pagesA Comprehensive Analysis of The Literature On The Impact of The Surgical Safety ChecklistInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Process Capability EngDocument11 pagesProcess Capability EngApoloTrevinoNo ratings yet
- Total Ankle Replacement Surgery (Arthroplasty)Document12 pagesTotal Ankle Replacement Surgery (Arthroplasty)ashut1No ratings yet
- Artificial intelligence approach in building automated diagnostics venipuncture blood analysis machineDocument14 pagesArtificial intelligence approach in building automated diagnostics venipuncture blood analysis machineKIPNGENO EMMANUELNo ratings yet
- F Kynaston-Pearson, A M Ashmore, T T Malak, I Rombach, A Taylor, D Beard, N K Arden, A Price, D Prieto-Alhambra, A Judge, A J Carr, S Glyn-JonesDocument11 pagesF Kynaston-Pearson, A M Ashmore, T T Malak, I Rombach, A Taylor, D Beard, N K Arden, A Price, D Prieto-Alhambra, A Judge, A J Carr, S Glyn-JonesLuis Gerardo Pérez CastroNo ratings yet
- 2-Statistical Controversies in Reporting of Clinical Trials - Part-2-Of-A-4 - 2015 - Journal-of-the-AmericaDocument15 pages2-Statistical Controversies in Reporting of Clinical Trials - Part-2-Of-A-4 - 2015 - Journal-of-the-AmericaPaulo SCNo ratings yet
- Ispor Literature ReviewDocument8 pagesIspor Literature Reviewafmzbzdvuzfhlh100% (1)
- Quality Control in HistopathologyDocument30 pagesQuality Control in HistopathologyMuhammad Jamiu Bello78% (9)
- Igrt ThesisDocument8 pagesIgrt Thesislisanetkowiczerie100% (1)
- Cytometry Part B Clinical - 2020 - Illingworth - International Guidelines For The Flow Cytometric Evaluation of PeripheralDocument28 pagesCytometry Part B Clinical - 2020 - Illingworth - International Guidelines For The Flow Cytometric Evaluation of PeripheralUcha PrasetyoNo ratings yet
- Drug-Eluting Stents: A Systematic Review and Economic EvaluationDocument6 pagesDrug-Eluting Stents: A Systematic Review and Economic EvaluationAleksandar CokanovicNo ratings yet
- Applying Taguchi Methods To Health CareDocument12 pagesApplying Taguchi Methods To Health CarehamzaabdalameerNo ratings yet
- On the Shelf Life of Pharmaceutical ProductsDocument8 pagesOn the Shelf Life of Pharmaceutical ProductsMihir DixitNo ratings yet
- Spinal Plating Systems Performance CriteriaDocument10 pagesSpinal Plating Systems Performance CriteriaJose Esteban Gomez LiscanoNo ratings yet
- Standards: Medical DevicesDocument3 pagesStandards: Medical DevicesDr M GeethanjaliNo ratings yet
- Unraveling The Potential of Real-World Studies (2017)Document4 pagesUnraveling The Potential of Real-World Studies (2017)Arturo Lopez GilNo ratings yet
- The Use of Short Dental Implants in Clinical Practice Literature ReviewDocument7 pagesThe Use of Short Dental Implants in Clinical Practice Literature Reviewd1jim0pynan2No ratings yet
- BMC Medical Research MethodologyDocument22 pagesBMC Medical Research MethodologyFabricio LafebreNo ratings yet
- Literature Review On Surgical Safety ChecklistDocument11 pagesLiterature Review On Surgical Safety Checklistfut0mipujeg3100% (1)
- Clinical Decision Support SystemsDocument8 pagesClinical Decision Support SystemsPushpendra ChauhanNo ratings yet
- Residual Life Prediction and Optimal Maintenance Decision for a Piece of EquipmentFrom EverandResidual Life Prediction and Optimal Maintenance Decision for a Piece of EquipmentNo ratings yet
- Data - Management - Dipen KhannaDocument45 pagesData - Management - Dipen KhannarubarooNo ratings yet
- Guidance - Engineering Tests For StentsDocument55 pagesGuidance - Engineering Tests For StentshamartinezNo ratings yet
- Saccharomyces boulardii May Shorten Diarrhea in ChildrenDocument5 pagesSaccharomyces boulardii May Shorten Diarrhea in ChildrenShankar YadavNo ratings yet
- Right To Try Act - UsaDocument4 pagesRight To Try Act - UsaJessica MessaNo ratings yet
- Kythera S-1 Ex. 99.1Document471 pagesKythera S-1 Ex. 99.1darwinbondgrahamNo ratings yet
- 2007 NiceDocument249 pages2007 NiceIrfan MohammadNo ratings yet
- Indian Life SciencesDocument3 pagesIndian Life Sciencesmukesh516No ratings yet
- Seattle Angina QuestionaireDocument9 pagesSeattle Angina QuestionaireBeaNo ratings yet
- Focus On Nursing Pharmacology Karch 5th Edition Test BankDocument36 pagesFocus On Nursing Pharmacology Karch 5th Edition Test Bankelapsionjealousymwhjl100% (38)
- Leachables Best Practice Guideline Disposable Solutions For Biomanufacturing PDFDocument36 pagesLeachables Best Practice Guideline Disposable Solutions For Biomanufacturing PDFAziz Aditya Wiguna100% (2)
- Acotiamide 8058Document6 pagesAcotiamide 8058MIHAELANo ratings yet
- Orthodontics Treatment For TMD JournalDocument19 pagesOrthodontics Treatment For TMD JournalEndang SetiowatiNo ratings yet
- Integrating Smoking Cessation Into Daily Nursing PracticeDocument86 pagesIntegrating Smoking Cessation Into Daily Nursing PracticeHamada BakheetNo ratings yet
- Health-Professionals Warn COVID Being A Hoax by Big Pharma CartelDocument61 pagesHealth-Professionals Warn COVID Being A Hoax by Big Pharma CartelCarlCordNo ratings yet
- Making Sense of Medical Evidence: Participant'S WorkbookDocument13 pagesMaking Sense of Medical Evidence: Participant'S Workbookmedia_allori100% (2)
- Oracle Argus Safety Data SheetDocument3 pagesOracle Argus Safety Data SheetDrmengani Vamsi Krishna Reddy100% (1)
- Logemann and Vitalstim Therapy PDFDocument2 pagesLogemann and Vitalstim Therapy PDFjoygarridoNo ratings yet
- Biocon:: Launching A New Cancer Drug in IndiaDocument10 pagesBiocon:: Launching A New Cancer Drug in IndiaDeepak Jangid0% (1)
- MLWH JapanDocument190 pagesMLWH JapanAsadulhaq Ali HamidiNo ratings yet
- Report On 3 Clinical Trials Involving Babies and Children in Institutional Settings 1960 61 1970 And1 973Document45 pagesReport On 3 Clinical Trials Involving Babies and Children in Institutional Settings 1960 61 1970 And1 973Mark MaloneNo ratings yet
- Monitoring Plan 4 WebsiteDocument5 pagesMonitoring Plan 4 WebsitejohncuyNo ratings yet
- Origins of Writing Ancient Civilizations Attributed The Origins of Writing To The GodsDocument8 pagesOrigins of Writing Ancient Civilizations Attributed The Origins of Writing To The GodsPeHmyang Pineda DielNo ratings yet
- Biocompatibility of Dental MaterialsDocument51 pagesBiocompatibility of Dental MaterialsEsome Sharma100% (1)
- Public Health Interventions: Applications For Public Health Nursing PracticeDocument249 pagesPublic Health Interventions: Applications For Public Health Nursing PracticeJemimah AdaclogNo ratings yet
- Statistical Analysis PlanDocument92 pagesStatistical Analysis PlanhimeshagrawalNo ratings yet
- 2020-The Impact of China's Policies On GlobalDocument364 pages2020-The Impact of China's Policies On GlobalChet PengNo ratings yet
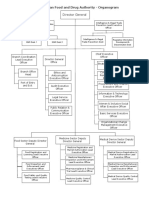
- EFDA Organogram English VersionDocument6 pagesEFDA Organogram English VersionRobsan YasinNo ratings yet
- Biological Testing of BiomaterialsDocument92 pagesBiological Testing of BiomaterialsShazia Rehman100% (1)
- Vertigoheel - Double - Blind - Comparative Betahistine 2000Document6 pagesVertigoheel - Double - Blind - Comparative Betahistine 2000Cristobal CarrascoNo ratings yet
- 1.41-4 Preamble Technological in NatureDocument19 pages1.41-4 Preamble Technological in NatureResearch and Development Tax Credit Magazine; David Greenberg PhD, MSA, EA, CPA; TGI; 646-705-2910No ratings yet