International Journal of Mathematics and Statistics Invention (IJMSI)
E-ISSN: 2321 4767 P-ISSN: 2321 - 4759
www.ijmsi.org Volume 4 Issue 6 || August. 2016 || PP-11-17
Under- Five Mortality in the West Mamprusi District of Ghana
MubarikaAlhassan1, MaahiTuahiru2, Abdul-HananAbdulai3
123
Department of Statistics, Mathematics &Science, Tamale Polytechnic, P. O. Box 3 E/R, Tamale-Ghana.
ABSTRACT: This study applied both descriptive and logistic regression analysis to the factors associated
with under five mortalities in the West Mamprusi district of Ghana. Results from the descriptive analysis
revealed that male deaths occur more than female deaths with a percentage of 52(52%) for the three years
whiles majority (32.24%) of the deaths were being cause by malaria. The interesting finding in this study was
that, among all the factors (variables) associated with under five mortalities, only one variable (i.e.
Prematurity) showed significant impact after running the analysis.
Keywords:Under-five mortality, Logistic Regression, Disease, Prematurity
I.
INTRODUCTION
Under-Five Mortality also known as Child Mortality refers to the death of infants and children under age of five.
The Under -Five Mortality Rate is the number of children who die by the age of five per thousand live births per
year. Worldwide an estimated 10.5 million children aged 0-4 years died in 1999, a reduction of about 2.2
million or 17.5% a decade ago. A report by UNICEF; WHO; The World Bank and UN Population Division
(2007), indicated that worldwide the number of children dying before the age of five reached a record low,
falling below 10 million for the first time in 2006. A decline which however is not evenly distributed. There are
still some regional differentials. The WHO (2006) estimates that on average about 15% of new born children in
Africa are expected to die before reaching their fifth birthday. The corresponding figures for many parts of
developing world are in the range of 3-8% and Europe under 2%. Sub-Saharan Africas infant and under five (5)
mortality rates are by far the highest. Situations like under development, armed conflict and the spread of
HIV/AIDS have seriously undermined the efforts to improve child survival. The estimated under-fivemortality
rate exceeds 200 deaths per 1000 live birth in ten countries in this region. Infant and child mortality rates also
remain relatively high in South Asia.
Omar, et al (2000) gives a good summary of the global trend of infant and child mortality. There have been
dramatic declines in mortality in almost all countries of the world, regardless of initial levels, socio-economic
circumstances and development strategies. In advance economies the declines were already apparent at the end
of the 19th century. In the period leading to 1970 under-five mortality in these countries were 27 deaths per 1000
live births, this decline to 10 deaths per 1000 live births in the period 1970-1990. In the decade that
followed,under-fivemortality decline to 7 deaths per 1000 live births. The decline took place during the time of
steady economic growth and major improvements in nutrition, housing, and living condition. Garenne and
Gakusi (2006) point out the development during the above period; the benefits during the period were
improvement in water and sanitation, hygiene, child feeding practices and the development of vaccines.
UNICEF (2004) identified a better, more effective and less costly medicines, technology, and interventions as
the main contributor to the steady decline in mortality rates in the industrialized countries during the period
1990-2003.
In the developing countries, under-fivemortality has declined, however it is still high compared to the develop
regions. In the period 1960-1970 under-fivemortality were 164 deaths per 1000 live birth and it further declined
to 128 deaths per 1000 live birth during the 1970-1980 period. In the following decade a further decline to 103
deaths per 1000 live births was observed. The downward trend continued beyond the year 1990. The 2006
figures indicatedthat under-fivemortality in this region declined to 79 deaths per 1000 live births. However, East
Asia and the Pacific, Latin America and the Caribbean, and Central/Eastern Europe and the Commonwealth of
Independent states had achieved under-five mortality rates of bellow 30 deaths per 1000 live births. Achieving
the Millennium Development Goal (MDG4) the target requires that the under-five mortality rate declines, on
average, by 4.4%annually between 1990 and 2015. These regions achieved this benchmark through 2006 or
came closer to it, putting them on track to achieve the MDG4 together (UNICEF, et al. 2007:7). Murray, et al.
(2007) suspected that some other factors might have been shared across these regions, such as educational or
environmental policies or the key driver of mortality change, accumulation of stocks of household, community
and national physical and human capital. All these put together could have driven the mortality decline in these
regions. UNICEF (2004) identified common conditions in countries where progress has been slow. Access to
clean water was low; percentage of under-five moderately or severally underweight was high; percentage of one
year olds who did not receive 3 doses of Diphtheria, Pertussis (whooping cough), and Tetanus (DPT)was high,
and percentage of children under-6 month of age who are not exclusively breastfed is high.
www.ijmsi.org
11 | Page
Under- Five Mortality In The West Mamprusi District Of Ghana.
Finally, among the developing regions mortality in Sub-Saharan Africa has remained notoriously high. UNICEF
(2004) approximates that 42% of children who die before they are five live in Sub-Saharan Africa. In 1960 the
under-fivemortality was 277 deaths per 1000 live births and adecade later it had decline to only 243 deaths per
1000 live births. In the period 1970-1980 the under-five mortality declined to 200 deaths per 1000 live births.
The pace of decline slowed down in the following decade when under-five mortality rate declined to 187 deaths
per1000 live births in 1990. During the period 1990-2000, the under-fivemortality declined further to 170 deaths
per 1000 live birth. However, West and Central Africa showed a higher rate of 193 per 1000 live births in the
same period while Eastern and Southern Africa reported 145 deaths per 1000 live births. The 2006 figures
indicates that the under-five mortality rate was 160 deaths per 1000 live births for the region, however, in West
and Central Africa it was 186 death per 1000 live births.
In Ghana currently, 50 children per 1,000 live births die before their first birthday (30 per 1,000 before the age
of one month and 21 per 1,000 between one and twelve months). Overall, 80 children per 1,000 live births, or
about one child out of twelve, die before reaching age five. These are dramatic decreases over the 20-year
period since the 1988 GDHS. Mortality rates differ by residence. The under-five mortality rate for the 10-year
period before the survey in urban areas was 75 per 1,000 live births compared to 90 per 1000 live births in rural
areas (GDHS, 2008).
The infant mortality rate has reduced from 20 deaths per 1,000 live births in 2010 to 17 per 1000 live births in
2011 in the west Mamprusi district. The child mortality rate has also declined from 49 per 1,000 live births to 37
per 1,000 live births for 2010 and2011 respectively (Wale District Hospital, 2011). These figures are below the
national infant mortality rate of 64 deaths per 1,000 live births and child mortality rate of 50 deaths per 1,000
(Ghana Statistical Service, 2004).
It is within this context that this paper proposes to explore the factors associated with under- five mortalities in
the West Mamprusi District.
The logistic regression model was use as the main statistical methodology for analyzing the data in order to
achieve the objective of this paper. The model tries to show the association between a categorical response
variable and a set of independent or predictor variables.
1.2 Statement of the Problem
According to Goro (2007) the disparities within countries in infant and child mortality observed in Africa are
equally experienced in Ghana. As with any averages, the national statistics has masked the disparities among the
regions and among the various socioeconomic groups within the country. According to Ghana Statistical Service
(2004) cited in Goro (2007), there is striking differential in infant mortality rates among the three northern
regions (Upper East, Upper West and Northern). Upper East region has the lowest infant mortality rate of 33 per
1000 live births in the country, with Upper West region having the highest infant mortality rate of 105 per 1000
live births followed by Ashanti region of 80 per 1000 live births, 75 for Volta region and 69 per 1000 live births
for Northern region. With regards to child mortality rate, there is sharp difference between the three northern
regions on one hand and the rest of the regions on the other hand. Upper West region has the highest child
mortality rate of 115 per 1000 live births in the country, followed by Northern region with 90 child deaths per
1000 live births and Upper East region having the third largest child mortality rate of 48 per 1000 live births in
country. In addition, marked regional differentials in under-five mortality are also observed. The Under- five
mortality rate ranges from a low of 75 per 1000 live births in the Greater Accra region to as high as 208 per
1000 live births in Upper West region followed by 116 in the Ashanti region and 154 per 1000 live births in
Northern region, however Upper East region ranked second to Greater Accra region with 79 deaths per 1000
live births (GSS, 2004). It is noticed from the above that Upper West region has the highest rates for all the three
levels of mortality in the country.
According to West Mamprusi district health directorate, Malaria and other diseases have claimed the lives of
many under five years children in West Mamprusi district of Northern region of Ghana. In 2010 and 2011 the
neonatal death rate was 7.8 and 3.7 per 1000 live birth respectively. Also post neonatal death was 26, 20 and 17
per 1000 live birth for 2010, 2011 and 2012 respectively (West Mamprusi district health directorate 2012
Annual Report).
In order to implement effective child survival programmers, there is the need to identify the factors that
contribute to child deaths and assess their effects. It is also important to take note of sharp mortality differentials
among various communities in the same district as different intervention strategies may be required to arrest the
situation. It is against this background that the study seeks to find out the factors associated with under-five
mortality trends (2010-2012) in West Mamprusi District of the Northern Region.
www.ijmsi.org
12 | Page
Under- Five Mortality In The West Mamprusi District Of Ghana.
II.
MATERIALS AND METHODS
The data for analysis of this paper was based on Secondary data from the West Mamprusi District hospital. The
data gathered was on under-five mortalities and the factors associated with it in the West Mamprusi district for
the period 2010-2012 indicating their sex, etc.
The logistic regression model was use as the main statistical method for analyzing the data in order to achieve
the objective of the paper. The model tried to show the association between a categorical response variable and a
set of independent or predictor variables. The dependent variable in this research is a binary response variable
(dichotomous) which is under-five mortalities. Factors in the data sampled were categorized as either death or
alive.
Furthermore, the Wald test together with the deviance and Chi-square test is use as criteria to either reject or fail
to reject independent variables in the model. SPSS was used to analyze the responses in order to address the
central question.
2.1 Logistic Regression Model
Logistic regression is a form of regression analysis used when the response variable is a binary variable. This
method is based on the logistic transformation or logic of a proportion p ;
p x
1 exp
1 p x 1
1 p x
0 1x
exp
exp
(1)
0 1x
1 exp
1 exp
0 1x
0 1x
0 1x
1 exp
exp
0 1x
0 1x
1
0 1x
1 exp
Writing the logistic regression in terms of Odds
Odds
p x
(2)
p
x
This can be obtained as follows
p x
1 p x
p x
1 p x
0 1x
exp
1 exp
exp
0 1x
1 exp
exp
0 1x
0 1x
1
1 exp
1 exp
0 1x
0 1x
0 1x
Taking logarithm of the odds gives the link function
p x
0 1 x (3)
g x log
1 p x
Hence, the transformation of logistic function known as the logit transformation becomes
p x
0 1x
log
1 p x
Where p = probability (dependent variable =1), and x is the explanatory variables.
www.ijmsi.org
13 | Page
Under- Five Mortality In The West Mamprusi District Of Ghana.
III.
DATA ANALYSIS AND RESULTS
3.1 Descriptive analysis
TABLE 1 below shows the summary statistics of diseases in relation to under-five mortalities in the district by
the various years (i.e. 2010-2012).Diseases are displayed in the first column as against the Deaths/Alive in the
top row by years.
Table 1 shows the number of diseases causing under-5 mortality by years
Disease
2010
2011
2012
Total
Death Alive Death Alive Death Alive Death Alive
Malaria
19
878
17
1596 13
1914
49
4388
Anaemia
5
104
2
164
3
221
10
489
Asphyxia
2
19
1
32
3
37
6
88
Dehydration 3
28
2
78
3
82
8
188
Typhoid
3
48
1
103
4
137
8
288
Malnutrition 3
87
5
240
4
361
12
688
Others
3
103
4
164
2
186
9
453
Pneumonia
5
98
3
212
4
278
12
588
Respitory
2
96
5
197
3
196
10
489
Prematurity
5
44
1
102
1
42
7
188
Sepsis
7
236
9
529
5
819
21
1584
Total
57
1741
50
3417 45
4273
152
9431
It is clear from the above Table 1that most of the under-five deaths are caused by malaria considering the three
years whiles the rest of the diseases fluctuates. As indicated in row 3 column 8, malaria has the highest number
(i.e. 49 cases) of death cases
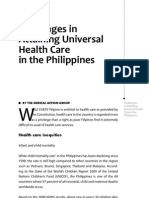
Figure 1: Proportions of Diseases Causing Under-5 Mortality
It is obvious from Figure 1 above that 32 % (49) of the deaths are caused by malaria while 4 %(6)are caused by
Asphyxia.
TABLE 2 shows the number of admissions, births, and deaths and alive by gender for the three years. It has the
various years shown in the first column whiles the Births, Number of admissions, male, female Deaths and
Alive in the first row
Table 2: summary of the number of admissions, births, deaths and alive from 2010-2012
Year Birth Admission Alive Death Male Death Female Death
2010 1186 1798
1741 57
32
25
2011 1453 3467
3417 50
22
28
2012 1578 4318
4273 45
32
13
Total 4217 9583
9431 152
86
66
www.ijmsi.org
14 | Page
Under- Five Mortality In The West Mamprusi District Of Ghana.
The TABLE 2 above suggests that, out of the 9583 admissions records for the three years, bulk(32) of the deaths
were males which occurred in 2010 and 2012 while fewwere females which occurred in 2012. Also, the number
of births in the health center increases accordingly from 1186 to 1578 for the three years.
TABLE 3 shows the frequency and percentage of admissions by gender in the West Mamprusi District. The
numbers of Female or Male admissions are displayed column wise whiles the frequency and percentages are in
row wise.
Table 3: Number of admissions by Gender
Gender
Frequency
Percent
Female
4578
47.7
Male
5005
52.3
Total Admissions
9583
100
It is obvious from Table 3 that, male admissions outweigh female admissions in the West Mamprusi District
Health Center by 52% and 46% respectively.
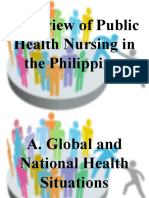
Figure 2: A pie chart showing the proportion of Admissions by Gender
From Figure 2, it can be seen clearly that out of the 9583 admissions in the Health Center for the period 20102012, majority are males (52%).
3.2 Data Analysis
Presented in TABLE 4 below are the results of the logit model for the factors with significant effect on underfive mortality. The coefficient, standard error,wald statistics, significant level, odds ratio and 95% confidence
level for all the variables (factors) are displayed rowwise whiles the variables are in column wise. Significant
factors are mainly identified by the significant levels.
Variables
S.E.
sex(1)
Malaria(1)
Anaemia(1)
Asphyxia(1)
Dehydration(1)
Typhoid(1)
Malnutrition(1)
Others(1)
Pneumonia(1)
Respitory(1)
Prematurity(1)
Constant
-38.194
38.365
36.212
15.886
16.063
16.212
.264
-.405
-.432
-.436
-1.033
4.324
1937.408
1937.408
1937.408
2174.979
1708.556
1528.880
.439
.402
.365
.388
.443
.220
Table 4: Parameter Estimation
Wald
Df Sig. Exp(B)
.000
.000
.000
.000
.000
.000
.362
1.016
1.400
1.265
5.436
387.470
1
1
1
1
1
1
1
1
1
1
1
1
www.ijmsi.org
.984
.984
.985
.994
.992
.992
.547
.313
.237
.261
.020
.000
.000
45874411684691100.000
5327620828285560.000
7928885.702
9466928.989
10985789.491
1.302
.667
.649
.647
.356
75.476
95%
C.I.for
EXP(B)
Lower Upper
0.000
0.000
0.000
0.000
0.000
0.000
.551
3.078
.303
1.466
.317
1.328
.302
1.382
.149
.848
15 | Page
Under- Five Mortality In The West Mamprusi District Of Ghana.
It is clear from the above TABLE 4 that, Prematurity and the Constantare the only variables that shows some
significant effect whiles the rest of the variables are not significant. Therefore, only one of the variables was
found statistically significant at 0.05 levels. The variable prematurity is significant at 0.05 significant level; thus
the variable becomes the variable used for the model.
Hence, the Logit Model Formulated is;
g ( x ) 4 . 324 1 . 033 prematurit
TABLE 5 illustrates the values of -2log likelihood, Cox and Snell and Pseeudo R square values for the logistic
regression model with the headings displayed in the top row follow by the values associated with them.
Table 5 Pseudo R Square of the Logit Regression Model for under five Mortality.
-2 Log likelihood Cox & Snell R Square
Negelkerke R Square
1273.627
.030
.197
The value of -2log likelihood is fairly large(1273.627), besides, the Cox and Snell R square value of 0.03 and
NegelkerkeRsquare of 0.197 are moderate. Hence the two values are between 3 per cent and 19.7 per cent. This
signifies that 3 per cent and 19.7 per cent of the variability in the dependent variable is explained by the model.
Shown in TABLE 6 below is the Hosmer and Lemeshow test for the fitted logistic regression model. The chi
square, degree of freedom and significant level are displayed in the top row with their corresponding values
below.
Table 6: Hosmer and Lemeshow Test of the Logit Model for Under-five Mortality.
Chi-square Degrees of Freedom(d.f) Significant level
.000
4
1.000
From TABLE 6 above the Hosmer and Lemeshow test has a chi-square value of 0.000 with corresponding pvalue of 1.00.This p-value is greater than the level of significance (i.e. 0.05), therefore, indicating support for
the model.
Presented in TABLE 7 is the results of the Omnibus test of the logit model coefficients of the factor associated
with under-five mortality. The table also shows in the first row, the Chi-square values, degrees of freedom (d.f)
and corresponding p-value for the three test criteria with their values displayed in columns 2, 3 and 4
respectively.
Table 7: OmnibusTest of the Logit Model for Under Five Mortality
Chi-square
df
Sig.
Step
287.684
11
.000
Block 287.684
11
.000
Model 287.684
11
.000
Indicated from TABLE 7 above, the Chi-square value and their corresponding p-values are 287.684 and 0.00 for
the entire omnibus test criterion. This p value implies that it is less than the significant level (i.e. p<0.05).Hence
suggesting that the entire test is statistically (highly) significant at 0.05(5%) level.
3.3 Discussion
The results from the descriptive analyses and the hierarchical logistic regression analysis from 2010-2012 birth
cohorts was provided and discussed.Among the demographic variables, the number of death occurrences for the
three years decreases with male deaths (52.3%) being the most dominant.Furthermore, results suggest that
malaria is the most dominant (32.24%) disease affecting under five mortality, followed by sepsis (13.82%) and
lastly by Asphyxia (3.95%).Findings show that Prematurity has adverse significant impact on underfivemortality. Similarly, our results suggest that malaria and prematurity adversely affects under five mortality.
However only the effect of Prematurity was statistically significant. It was also realized that the cox and Snell
values between 3% and 19.7%suggests that the variability in the dependent variable is explained by the set of
variables in the model.However the Hosmer and Lemeshow test has its p-value of 1.000 greater than the level
significant (0.05), suggesting that the model is statistically significant.
www.ijmsi.org
16 | Page
Under- Five Mortality In The West Mamprusi District Of Ghana.
IV.
CONCLUSION
In summary under-fivemortality was significantly associated with only one variable during 2010-2012 period
namely; Prematurity. The observed level of significance for regression coefficients(i.e. 0.02) for this variable
was less than 5% suggesting that this variable was indeed good explanatory Variable. Hence the Logit Model
for Prematurity as the only significant variable was
g ( x ) 4 . 324 1 . 033 prematurit
Results emerging from the pseudo R Square (i.e. Cox and Snell =0.30; Negelkerke R Square = 0.197) suggests
that the factors identified as the significant factors in the model gives a moderate prediction of under-five
mortality. Moreover, the chi-square value of 0.000with corresponding p-values of 1.000 from the Hosmer and
Lemeshow test gives an indication that the fitted logit model is consistent with the data used in this paper.Also,
the chi-square value of 287.684 with corresponding p-values of 0.00 from the omnibus test signifies that the
predictors are significant.Furthermore, the table classification shows that we were 98.7% right in the
classification of our causes (cases). Thus indicating that, the model presents a reasonable statistical fit.
REFERENCES
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
[10].
[11].
[12].
[13].
[14].
[15].
[16].
UNICEF, WHO, The World Bank & United Nations Population Division. Levels and trends of child mortality in 2006 Estimates
developed by the inter-agency Group for Child Mortality Estimation 2007.
World Health Organization. Neonatal and Perinatal Mortality Country, Regional and Global Estimates 2006.
Omar B. A., Alan D.L., & Mie I.The Decline in Child Mortality: A Reappraisal. Bulletin of the World Health Organization
78(10): 1,1751,191, 2000.
Garenne, M. &Gakusi, E. Under-five Mortality Trends in Africa: Reconstruction from Demographic Sample Survey.
Demographic and Health Research 2005 No. 26.
UNICEF.
Progress
for
Children,
A
Child
Survival
Report
Card:
Number1,
2004
http://www.unicef.org/prgressforchildren/2004v1/industrialized.phd
UNICEF (2007). The State of the World's Children Reports. Access from www.unicef.org/sowc07/docs/sowc07.pdf on Nov
28,2014
Murray, J.L., Laakso, A., B., Shibuya, K., Hill, K. & Lopez, A.D. Can we achieve Millennium Development Goal 4? New analysis
of country trends and forecasts of under-5 mortality to 2015. Lancet 2007; Vol (370) 1040-54.
Ghana Demographic and Health Survey 2008. Accessed from www.statsghana.gov.gh/nada/index.php/catalog/121/download/132
on Sept 20,2014
West Mamprusi district Health Directorate (2012): Annual report-2012. Walewale, Ghana.
Ghana
Statistical
Service
(2004):
Ghana
Demographic
and
Health
Survey
2004.
Accessed
from
www.statsghana.gov.gh/nada/index.php/catalog/13/download/18 on Sept 20,2014
th
Iddrisu, M. G. The Stalling Child Mortality in Ghana: The case of the three Northern Regions. The 5 Conference of union for
Africa Population Studies (UAPS) at Arusha, Tanzania, 2007.
Agresti,A. An introduction to Categorical data analysis.2ndEdition,JohnWileyand Sons,Inc.,New York, 2007.
Pallant J: SPSS Survival Manual, A Step by Step guide to data analysis using SPSS ,4th edition
Peter B. Factors Associated With Under-5 Mortality In South Africa: Trends 1997- 2002. Masters Thesis, Faculty of Humanities,
University Of Pretoria, Pretoria, 2010.
UNICEF Statistics (2010). Levels and Trends in Child Mortality Report: Estimates Developed by the UN Inter-agency Group for
Child
Mortality
Estimation.
Access
from
www.chilgmortality.org/filesv19/download/levels%20and%20Trends%20in%20Child%20Mortality%20Report%202010.pdf
on
Nov 28, 2014
World Bank, (2003). Ghana Poverty Reduction Strategy 2003-2005: An agenda for growth and prosperity vol (1): Analysis and
Policy Statement, February 19, 2003. Washington D.C. The World Bank.
www.ijmsi.org
17 | Page
You might also like
- Skip To Main ContentDocument5 pagesSkip To Main ContentReza SaputreeNo ratings yet
- UNIT SEVENDocument47 pagesUNIT SEVENThomas GebeyehuNo ratings yet
- Chapter Two Mortality NewDocument16 pagesChapter Two Mortality NewElijah boluwatifrNo ratings yet
- Infant Mortality: Its Trends, Reasons and Impact Upon Pakistani Society From 2007 To 2017Document10 pagesInfant Mortality: Its Trends, Reasons and Impact Upon Pakistani Society From 2007 To 2017Huma SadiaNo ratings yet
- Community Slides 02 DemographyDocument63 pagesCommunity Slides 02 Demographyhamza jassar100% (1)
- Infant Child Mortality Rates and LEDocument18 pagesInfant Child Mortality Rates and LEZanzibarNo ratings yet
- Health ReportDocument17 pagesHealth ReportSaima DanaNo ratings yet
- 2006 FPS NSO Press ReleaseDocument3 pages2006 FPS NSO Press Release7simjNo ratings yet
- Lec 3 Basic Demography 21Document84 pagesLec 3 Basic Demography 21MOSESNo ratings yet
- MICS Ghana 2011 - Bit17Document2 pagesMICS Ghana 2011 - Bit17BobNo ratings yet
- Philippines Population, Health Issues & TrendsDocument16 pagesPhilippines Population, Health Issues & TrendsMilo PlacinoNo ratings yet
- Under Age 5 Mortality: 3. Health StatusDocument3 pagesUnder Age 5 Mortality: 3. Health StatusSolomon Nageso LaaftooNo ratings yet
- Demography (Supplemental Lecture)Document3 pagesDemography (Supplemental Lecture)Roldan MapeNo ratings yet
- Nursing Research On Early PregnancyDocument15 pagesNursing Research On Early PregnancyMARY ANGELICA AQUINO100% (1)
- Philippines Country Landscape OutlineDocument7 pagesPhilippines Country Landscape OutlineMa. Cristina TanadaNo ratings yet
- Challenges in Attaining Universal Health Care in The PhilippinesDocument42 pagesChallenges in Attaining Universal Health Care in The Philippineskasamahumanrights100% (1)
- Population Dynamics: Causes, Trends & Factors Affecting GrowthDocument28 pagesPopulation Dynamics: Causes, Trends & Factors Affecting GrowthNicole OngNo ratings yet
- 2 Revised Guen Gant PaperDocument22 pages2 Revised Guen Gant PaperAhmad Wid SanjayaNo ratings yet
- Overview of Public Health Nursing in The PhilippinesDocument52 pagesOverview of Public Health Nursing in The PhilippinesWilma BeraldeNo ratings yet
- MortalityDocument21 pagesMortalityvishalkrmahathaNo ratings yet
- 2021-Epidemiology of Atrial FibrillationDocument23 pages2021-Epidemiology of Atrial FibrillationAlberto Jesus Morales JuradoNo ratings yet
- Mortality RateDocument5 pagesMortality Rateamit kumar dewanganNo ratings yet
- Progress of Goal 3 in 2017: Reproductive, Maternal, Newborn and Child HealthDocument5 pagesProgress of Goal 3 in 2017: Reproductive, Maternal, Newborn and Child HealthIsni Fatimah Azura SaragihNo ratings yet
- IB SL Geography Revision NotesDocument46 pagesIB SL Geography Revision NotesMohamed Shariff100% (10)
- Case Study On Ending Female Genital Mutilation: in The State of EritreaDocument12 pagesCase Study On Ending Female Genital Mutilation: in The State of EritreaSamridhi PrakashNo ratings yet
- Demography Final Handout CorrectedDocument20 pagesDemography Final Handout Correctedmadanlal sainiNo ratings yet
- Population: PROF.: Juan Luis 3º E.S.O. Social SciencesDocument15 pagesPopulation: PROF.: Juan Luis 3º E.S.O. Social SciencesmarcelnegreaNo ratings yet
- The Location and Growth of AIDS/HIV.: Grade 9 AIDS Report Due 10 October (Friday) 2014. Task: Due WednesdayDocument6 pagesThe Location and Growth of AIDS/HIV.: Grade 9 AIDS Report Due 10 October (Friday) 2014. Task: Due WednesdayAnamika DebNo ratings yet
- Dhs Working Papers Dhs Working Papers: Factors Affecting Maternal Health Care Seeking Behavior in RwandaDocument31 pagesDhs Working Papers Dhs Working Papers: Factors Affecting Maternal Health Care Seeking Behavior in Rwanda15-0001No ratings yet
- CF AdaptedDocument13 pagesCF AdaptedCynthia Anggraini PutriNo ratings yet
- SSRN Id3432263Document16 pagesSSRN Id3432263Sameera AfNo ratings yet
- The Millennium Development GoalsDocument7 pagesThe Millennium Development Goalsjug27No ratings yet
- Demographic and Socioeconomic Statistics: Orld Ealth TatisticsDocument11 pagesDemographic and Socioeconomic Statistics: Orld Ealth Tatisticsingrid_panturu5576No ratings yet
- AssignmentDocument3 pagesAssignmentPaul Nyakeh KandorNo ratings yet
- Mother-To-Child Transmission (MTCT) of Hiv/AidsDocument23 pagesMother-To-Child Transmission (MTCT) of Hiv/AidsParamita ArdiyantiNo ratings yet
- Population Growth and Economic Development:: Causes, Consequences and ControversiesDocument14 pagesPopulation Growth and Economic Development:: Causes, Consequences and Controversiesjainaastha111No ratings yet
- Assignment On Demography....Document4 pagesAssignment On Demography....biswasjoyNo ratings yet
- Understanding Global Population TrendsDocument4 pagesUnderstanding Global Population TrendsArvie TVNo ratings yet
- Demography Cycle: Ashish Gaur Assistant Professor Department of Community MedicineDocument23 pagesDemography Cycle: Ashish Gaur Assistant Professor Department of Community MedicineSamiksha goyalNo ratings yet
- FCM3-3.02 Philippine Cancer Control ProgramDocument11 pagesFCM3-3.02 Philippine Cancer Control ProgramJoher MendezNo ratings yet
- Mm61e0416 Injury DeathDocument7 pagesMm61e0416 Injury DeathThalia SandersNo ratings yet
- Global Maternal, Newborn, and Child Health - So Near and Yet So FarDocument10 pagesGlobal Maternal, Newborn, and Child Health - So Near and Yet So FarAngellaNo ratings yet
- Concepts of Demography ExplainedDocument19 pagesConcepts of Demography ExplainedPhilemon MsangiNo ratings yet
- Environmental Management - Population RevisionDocument14 pagesEnvironmental Management - Population RevisionNikhil YadavNo ratings yet
- HIV AIDS HandoutDocument11 pagesHIV AIDS HandoutMarius BuysNo ratings yet
- Missing Women Revisited by Amartya SenDocument2 pagesMissing Women Revisited by Amartya SenDebashish BoseNo ratings yet
- LESSON 2 - Human Population Dynamic - IssuesDocument8 pagesLESSON 2 - Human Population Dynamic - IssuesDalupire, Jhonryl A.No ratings yet
- 2014 PL9 Afghanistan - CPD Final - Approved ENDocument12 pages2014 PL9 Afghanistan - CPD Final - Approved ENWilliam LinaresNo ratings yet
- The Demographic TransitionDocument6 pagesThe Demographic TransitionUbaid KhanNo ratings yet
- Massachusetts Teen Births 2013Document18 pagesMassachusetts Teen Births 2013Patrick JohnsonNo ratings yet
- The Socio-Economic Determinants of HIV/AIDS Infection Rates in Lesotho, Malawi, Swaziland and ZimbabweDocument22 pagesThe Socio-Economic Determinants of HIV/AIDS Infection Rates in Lesotho, Malawi, Swaziland and Zimbabweecobalas7No ratings yet
- 2014 PL10 Sierra - Leone - CPD Final - Approved ENDocument12 pages2014 PL10 Sierra - Leone - CPD Final - Approved ENWilliam LinaresNo ratings yet
- Population Dynamics (CSEC Geography)Document25 pagesPopulation Dynamics (CSEC Geography)Kym Singh100% (2)
- Factors Affecting Mortality Rate I Ri JDocument8 pagesFactors Affecting Mortality Rate I Ri Jismail taiwoNo ratings yet
- IB Revision The Core Topic 1 - Populations in TransitionDocument10 pagesIB Revision The Core Topic 1 - Populations in TransitiontomNo ratings yet
- Public Health Data Concepts - DR Rajan DubeyDocument13 pagesPublic Health Data Concepts - DR Rajan DubeyDr Rajan DubeyNo ratings yet
- Health Related Millennium Development Goals Part IDocument24 pagesHealth Related Millennium Development Goals Part IGudegna GemechuNo ratings yet
- Overpopulation MLS 2E (Revised)Document23 pagesOverpopulation MLS 2E (Revised)Yvonne Mae CapatayanNo ratings yet
- The Effect of Transformational Leadership, Organizational Commitment and Empowerment On Managerial Performance Through Organizational Citizenship Behavior at PT. Cobra Direct Sale IndonesiaDocument9 pagesThe Effect of Transformational Leadership, Organizational Commitment and Empowerment On Managerial Performance Through Organizational Citizenship Behavior at PT. Cobra Direct Sale Indonesiainventionjournals100% (1)
- Effects of Online Marketing On The Behaviour of Consumers in Selected Online Companies in Owerri, Imo State - NigeriaDocument12 pagesEffects of Online Marketing On The Behaviour of Consumers in Selected Online Companies in Owerri, Imo State - Nigeriainventionjournals100% (1)
- Islamic Insurance in The Global EconomyDocument3 pagesIslamic Insurance in The Global EconomyinventionjournalsNo ratings yet
- A Discourse On Modern Civilization: The Cinema of Hayao Miyazaki and GandhiDocument6 pagesA Discourse On Modern Civilization: The Cinema of Hayao Miyazaki and GandhiinventionjournalsNo ratings yet
- Muslims On The Margin: A Study of Muslims OBCs in West BengalDocument6 pagesMuslims On The Margin: A Study of Muslims OBCs in West BengalinventionjournalsNo ratings yet
- An Appraisal of The Current State of Affairs in Nigerian Party PoliticsDocument7 pagesAn Appraisal of The Current State of Affairs in Nigerian Party PoliticsinventionjournalsNo ratings yet
- The Social Composition of Megaliths in Telangana and Andhra: An Artefactual AnalysisDocument7 pagesThe Social Composition of Megaliths in Telangana and Andhra: An Artefactual AnalysisinventionjournalsNo ratings yet
- Effects of Online Marketing On The Behaviour of Consumers in Selected Online Companies in Owerri, Imo State - Nigeria.Document12 pagesEffects of Online Marketing On The Behaviour of Consumers in Selected Online Companies in Owerri, Imo State - Nigeria.inventionjournalsNo ratings yet
- The Network Governance in Kasongan Industrial ClusterDocument7 pagesThe Network Governance in Kasongan Industrial ClusterinventionjournalsNo ratings yet
- Negotiated Masculinities in Contemporary American FictionDocument5 pagesNegotiated Masculinities in Contemporary American FictioninventionjournalsNo ratings yet
- The Usage and Understanding of Information and Communication Technology On Housewife in Family Welfare Empowerment Organization in Manado CityDocument10 pagesThe Usage and Understanding of Information and Communication Technology On Housewife in Family Welfare Empowerment Organization in Manado CityinventionjournalsNo ratings yet
- Literary Conviviality and Aesthetic Appreciation of Qasa'id Ashriyyah (Decaodes)Document5 pagesLiterary Conviviality and Aesthetic Appreciation of Qasa'id Ashriyyah (Decaodes)inventionjournalsNo ratings yet
- Inter-Caste or Inter-Religious Marriages and Honour Related Violence in IndiaDocument5 pagesInter-Caste or Inter-Religious Marriages and Honour Related Violence in IndiainventionjournalsNo ratings yet
- Student Engagement: A Comparative Analysis of Traditional and Nontradional Students Attending Historically Black Colleges and UniversitiesDocument12 pagesStudent Engagement: A Comparative Analysis of Traditional and Nontradional Students Attending Historically Black Colleges and Universitiesinventionjournals100% (1)
- The Impact of Leadership On Creativity and InnovationDocument8 pagesThe Impact of Leadership On Creativity and InnovationinventionjournalsNo ratings yet
- E0606012850 PDFDocument23 pagesE0606012850 PDFinventionjournalsNo ratings yet
- Effect of P-Delta Due To Different Eccentricities in Tall StructuresDocument8 pagesEffect of P-Delta Due To Different Eccentricities in Tall StructuresinventionjournalsNo ratings yet
- A Critical Survey of The MahabhartaDocument2 pagesA Critical Survey of The MahabhartainventionjournalsNo ratings yet
- Non-Linear Analysis of Steel Frames Subjected To Seismic ForceDocument12 pagesNon-Linear Analysis of Steel Frames Subjected To Seismic ForceinventionjournalsNo ratings yet
- D0606012027 PDFDocument8 pagesD0606012027 PDFinventionjournalsNo ratings yet
- C0606011419 PDFDocument6 pagesC0606011419 PDFinventionjournalsNo ratings yet
- F0606015153 PDFDocument3 pagesF0606015153 PDFinventionjournalsNo ratings yet
- E0606012850 PDFDocument23 pagesE0606012850 PDFinventionjournalsNo ratings yet
- H0606016570 PDFDocument6 pagesH0606016570 PDFinventionjournalsNo ratings yet
- C0606011419 PDFDocument6 pagesC0606011419 PDFinventionjournalsNo ratings yet
- F0606015153 PDFDocument3 pagesF0606015153 PDFinventionjournalsNo ratings yet
- Non-Linear Analysis of Steel Frames Subjected To Seismic ForceDocument12 pagesNon-Linear Analysis of Steel Frames Subjected To Seismic ForceinventionjournalsNo ratings yet
- H0606016570 PDFDocument6 pagesH0606016570 PDFinventionjournalsNo ratings yet
- Development of Nighttime Visibility Assessment System For Road Using A Low Light CameraDocument5 pagesDevelopment of Nighttime Visibility Assessment System For Road Using A Low Light CamerainventionjournalsNo ratings yet
- D0606012027 PDFDocument8 pagesD0606012027 PDFinventionjournalsNo ratings yet
- Standards TattooingDocument12 pagesStandards Tattooingcaleyramsay100% (1)
- Chapter 1 - Performance TaskDocument18 pagesChapter 1 - Performance Taskmargarita perezNo ratings yet
- Gram Negative Cocci (Lecture Notes)Document5 pagesGram Negative Cocci (Lecture Notes)Dayledaniel Sorveto100% (1)
- Antivirals (Katzung)Document6 pagesAntivirals (Katzung)sarguss1467% (3)
- Summary of Key Points: Tetanus Vaccines: WHO Position Paper - February 2017Document19 pagesSummary of Key Points: Tetanus Vaccines: WHO Position Paper - February 2017rendha sasongkoNo ratings yet
- HPV GardasilDocument2 pagesHPV Gardasilapi-237098034No ratings yet
- Guidelines For Office Gynecology in JapanDocument17 pagesGuidelines For Office Gynecology in JapanKatherine ZevallosNo ratings yet
- Journal Pmed 1001125 s005Document71 pagesJournal Pmed 1001125 s005Arhi WidhiaNo ratings yet
- MHC Class II Deficiency Case StudyDocument2 pagesMHC Class II Deficiency Case StudyBre GlynnNo ratings yet
- Drug StudyDocument1 pageDrug StudyBSN 3-2 RUIZ, Jewel Anne F.No ratings yet
- Blackleg (Black Quarter)Document18 pagesBlackleg (Black Quarter)Chursi BillaNo ratings yet
- Using Teleprimary Care To Monitor Immunization Status in Sarikei HealthDocument5 pagesUsing Teleprimary Care To Monitor Immunization Status in Sarikei Healthnazul izwanNo ratings yet
- Statement From Marathon Pharmaceuticals On EmflazaDocument4 pagesStatement From Marathon Pharmaceuticals On EmflazaNed PagliaruloNo ratings yet
- QIMP14 AppendixDocument12 pagesQIMP14 AppendixShahriar MostafaNo ratings yet
- Biology Chapter 5 Form 5Document15 pagesBiology Chapter 5 Form 5Nadiah BorhanNo ratings yet
- Snap 4dx Plus Sensitivity Specificity PDFDocument1 pageSnap 4dx Plus Sensitivity Specificity PDFDesriwanAnggaMedicaNo ratings yet
- Haitian Creole For HealthcareDocument15 pagesHaitian Creole For HealthcareAlton Johnson100% (1)
- Emergency Health KitDocument72 pagesEmergency Health KitAmit ChatterjeeNo ratings yet
- (Digeorge Syndrom) : Dr. Ahmed A. Azab MBBCH, MSC, MDDocument44 pages(Digeorge Syndrom) : Dr. Ahmed A. Azab MBBCH, MSC, MDDrAhmed Abdulfattah AzabNo ratings yet
- IPPI 2013 Manpower Planning FormDocument35 pagesIPPI 2013 Manpower Planning FormhariharansnsNo ratings yet
- Welcome To CanadaDocument89 pagesWelcome To Canadaapi-3761095No ratings yet
- OB HistoryDocument2 pagesOB Historyela garciaNo ratings yet
- Measles Outbreak Political Cartoon AnalysisDocument4 pagesMeasles Outbreak Political Cartoon AnalysisRamizNo ratings yet
- COPARDocument118 pagesCOPARleemeiOO100% (1)
- Febrile SeizureDocument16 pagesFebrile SeizureRashed Shatnawi100% (1)
- FormulaDocument27 pagesFormulaSadia KausarNo ratings yet
- Critical Thinking Exercises Pediatric NursingDocument8 pagesCritical Thinking Exercises Pediatric NursingCharmaine Rose Inandan TriviñoNo ratings yet
- Factors Associated With Home Maternal Deliveries in Rural AreasDocument24 pagesFactors Associated With Home Maternal Deliveries in Rural AreasJASH MATHEW100% (1)
- The Wall Street Journal - 24.02.2021Document34 pagesThe Wall Street Journal - 24.02.2021xguessNo ratings yet