You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Motivation For Drug UseDocument19 pagesMotivation For Drug UseGabrielaNo ratings yet
- Premature EjaculationDocument44 pagesPremature EjaculationTarek Anis67% (6)
- Myers AP 3e - Unit 3 - WatermarkDocument78 pagesMyers AP 3e - Unit 3 - WatermarkRahaf AftanNo ratings yet
- Drugs That Affect Smooth MuscleDocument90 pagesDrugs That Affect Smooth MuscleGeraldine Marie Salvo100% (1)
- NkpsycologyDocument387 pagesNkpsycologyCenter for Global NonkillingNo ratings yet
- Imbalanced Neurotransmitters and Abnormal BehaviorDocument3 pagesImbalanced Neurotransmitters and Abnormal BehaviorInah100% (1)
- BugSpeaks Sample ReportDocument27 pagesBugSpeaks Sample ReportAnonymous 76wOMTpNo ratings yet
- Neurotransmitters - 2016Document183 pagesNeurotransmitters - 2016AdminNo ratings yet
- AmphetaminesDocument39 pagesAmphetaminesRonie Alvarez MaldonadoNo ratings yet
- 06.a Happy HormonesDocument2 pages06.a Happy Hormones박소이No ratings yet
- Sharma M Et - Al. (1) - 1Document12 pagesSharma M Et - Al. (1) - 1P S AmritNo ratings yet
- Drug Interactions Results - MICROMEDEX - MAYODocument10 pagesDrug Interactions Results - MICROMEDEX - MAYOMARIA JULIANA RENGIFO LARANo ratings yet
- Dwnload Full Psychology of Criminal Behaviour A Canadian Perspective Canadian 2nd Edition Brown Test Bank PDFDocument36 pagesDwnload Full Psychology of Criminal Behaviour A Canadian Perspective Canadian 2nd Edition Brown Test Bank PDFslipknotdartoid0wdc100% (9)
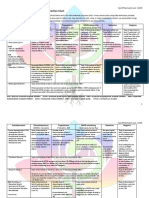
- Drug Interaction Chart for Antidepressants and PsychedelicsDocument3 pagesDrug Interaction Chart for Antidepressants and PsychedelicsFred The Nomad100% (2)
- Nonstop Natural GainsDocument38 pagesNonstop Natural GainsFabiano LacerdaNo ratings yet
- Core Concepts of Psychiatric-Mental Health NursingDocument31 pagesCore Concepts of Psychiatric-Mental Health NursingCyrille Anne MongeNo ratings yet
- OcdDocument11 pagesOcdNem AlNo ratings yet
- 08 - Gastrointestinal and Exocrine Pancreatic FunctionDocument7 pages08 - Gastrointestinal and Exocrine Pancreatic Functionhamadadodo7No ratings yet
- Cannon 11-27-2014Document76 pagesCannon 11-27-2014Dave MundyNo ratings yet
- Electromagnetic Properties of Rudraksha PDFDocument3 pagesElectromagnetic Properties of Rudraksha PDFPammy JainNo ratings yet
- Anxiety: Insights Into Signs, Symptoms, Etiology, Pathophysiology, and TreatmentDocument13 pagesAnxiety: Insights Into Signs, Symptoms, Etiology, Pathophysiology, and TreatmentMichael Judika Deardo PurbaNo ratings yet
- Yokukansan (TJ-54) in The Treatment Neurological Disorders - A ReviewDocument6 pagesYokukansan (TJ-54) in The Treatment Neurological Disorders - A ReviewAurelianNo ratings yet
- 3-Fluoromethcathinone, A Structural Analog of Mephedrone - Siedlecka-Kroplewska - Journal of Physiology and Pharmacology 64 (2014)Document6 pages3-Fluoromethcathinone, A Structural Analog of Mephedrone - Siedlecka-Kroplewska - Journal of Physiology and Pharmacology 64 (2014)dextroenantiomerNo ratings yet
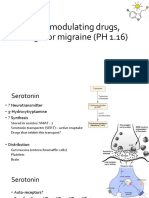
- 5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)Document13 pages5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)shruti sangwanNo ratings yet
- PHARMACOLOGY OVERVIEWDocument67 pagesPHARMACOLOGY OVERVIEWZehra KhanNo ratings yet
- Analysis, Nutrition, and Health Benefits of Tryptophan: Mendel FriedmanDocument12 pagesAnalysis, Nutrition, and Health Benefits of Tryptophan: Mendel Friedmanرشاد د.احمدNo ratings yet
- Does Healthy Diet Improve Mental HealthDocument3 pagesDoes Healthy Diet Improve Mental Healthananya singhalNo ratings yet
- Life Magazine March 25 1966Document12 pagesLife Magazine March 25 1966paulscribderNo ratings yet
- Gut-Brain Connection: How the Enteric Nervous System Impacts Mood & DigestionDocument4 pagesGut-Brain Connection: How the Enteric Nervous System Impacts Mood & Digestionjuanitos111No ratings yet
- Serotonin SyndromeDocument6 pagesSerotonin SyndromeCarlos ÁgredaNo ratings yet