You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Pathogenesis and Classification of NeoplasiaDocument36 pagesPathogenesis and Classification of NeoplasiaCLEMENT0% (1)
- Absolute Clinical Radiation Oncology Review (PDFDrive) PDFDocument500 pagesAbsolute Clinical Radiation Oncology Review (PDFDrive) PDFMd. Ashikur Rahman100% (1)
- DSM V Clinical Cases - Chapter 12 Sleep Wake DisordersDocument13 pagesDSM V Clinical Cases - Chapter 12 Sleep Wake DisordersIzzyinOzzieNo ratings yet
- Orthopedics Ebook Notes PDFDocument42 pagesOrthopedics Ebook Notes PDFindia2puppy100% (2)
- SOP Kids Club COVID 19 Measure For GO 2Document2 pagesSOP Kids Club COVID 19 Measure For GO 2adjcdaughtNo ratings yet
- Gastrointestinal Oncology - J. Abbruzzese, Et Al., (Oxford, 2004) WW PDFDocument938 pagesGastrointestinal Oncology - J. Abbruzzese, Et Al., (Oxford, 2004) WW PDFRaluca MărgulescuNo ratings yet
- Hypertension Related To Faulty Eating Habits As Evidence My Blood Pressure of 13080.Document2 pagesHypertension Related To Faulty Eating Habits As Evidence My Blood Pressure of 13080.Senyorita KHayeNo ratings yet
- ARI CONTROL PROGRAMMEDocument13 pagesARI CONTROL PROGRAMMEArun George50% (8)
- 2014 EDAIC II Istanbul 2014 1Document2 pages2014 EDAIC II Istanbul 2014 1igorNo ratings yet
- Clinical Efficacy of Enhanced Recovery After Surgery in Percutaneous Nephrolithotripsy: A Randomized Controlled TrialDocument8 pagesClinical Efficacy of Enhanced Recovery After Surgery in Percutaneous Nephrolithotripsy: A Randomized Controlled TrialfaundraNo ratings yet
- BJS5 4 157Document7 pagesBJS5 4 157faundraNo ratings yet
- Enhanced Recovery After SurgeryDocument36 pagesEnhanced Recovery After Surgeryfaundra100% (1)
- Joacp 35 5Document9 pagesJoacp 35 5faundraNo ratings yet
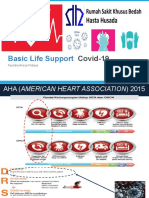
- Basic Life Support: Covid-19Document12 pagesBasic Life Support: Covid-19faundraNo ratings yet
- Icd Non TraumaDocument4 pagesIcd Non TraumafaundraNo ratings yet
- Physrev 00048 2010Document77 pagesPhysrev 00048 2010faundraNo ratings yet
- Sellick ManuverDocument2 pagesSellick ManuverfaundraNo ratings yet
- CKDDocument25 pagesCKDiwansagarNo ratings yet
- Sellick ManuverDocument2 pagesSellick ManuverfaundraNo ratings yet
- Chronic Complications of Spinal Cord Injury and Disease - UpToDateDocument25 pagesChronic Complications of Spinal Cord Injury and Disease - UpToDateElinaldo Soares Costa SilvaNo ratings yet
- Nurani Kaeda - Part 1Document5 pagesNurani Kaeda - Part 1farah_nishuNo ratings yet
- Li V Sps. SolimanDocument4 pagesLi V Sps. SolimanTriccie MangueraNo ratings yet
- Vitamin K DeficiencyDocument10 pagesVitamin K Deficiencyassassain creedNo ratings yet
- Systemic Sclerosis (Scleroderma)Document3 pagesSystemic Sclerosis (Scleroderma)AtiqahNo ratings yet
- Etiological Potential of Immature Platelet Fraction in Children with ThrombocytopeniaDocument29 pagesEtiological Potential of Immature Platelet Fraction in Children with Thrombocytopeniajhanavi rajeshNo ratings yet
- Computer Vision SyndromeDocument3 pagesComputer Vision Syndromeviren thakkarNo ratings yet
- Fever Proforma and Assignment - 1Document48 pagesFever Proforma and Assignment - 1SivaNo ratings yet
- Zoladex BC 2019 - ApprovedDocument23 pagesZoladex BC 2019 - ApprovedSiti DaraauliaNo ratings yet
- Skin Rejuvenation and Aging Process UpdatesDocument5 pagesSkin Rejuvenation and Aging Process UpdatesAmelluves ImanNo ratings yet
- Depression Euphoria and Anger in The Emergency SettingDocument38 pagesDepression Euphoria and Anger in The Emergency SettingpbsaintNo ratings yet
- GFCH-Sheng Mai FormulaDocument8 pagesGFCH-Sheng Mai Formulamday83No ratings yet
- Case On ColitisDocument34 pagesCase On ColitisAamer SyedNo ratings yet
- Clostridia and Bacillus Lecture NotesDocument37 pagesClostridia and Bacillus Lecture NotesPrincewill SeiyefaNo ratings yet
- Roberts, By: Cardiology 1993 E. Clinical Cardiology, 6th EditionDocument1 pageRoberts, By: Cardiology 1993 E. Clinical Cardiology, 6th EditionShiv GauravNo ratings yet
- How Can Blood Diseases Be IdentifiedDocument4 pagesHow Can Blood Diseases Be Identifiedllatham0% (1)
- Case Study SampleDocument4 pagesCase Study SamplemandyNo ratings yet
- Cerebral PalsyDocument2 pagesCerebral PalsyTracy100% (1)
- Antibiotics 1038832656Document20 pagesAntibiotics 1038832656Achilles Ok OkNo ratings yet
- Team Aproach With Diabetes PatientsDocument5 pagesTeam Aproach With Diabetes PatientsLuis Vazquez MoralesNo ratings yet
- CGHS Referral Procedure GuideDocument3 pagesCGHS Referral Procedure GuideadhityaNo ratings yet