You might also like
- Case Processing SummaryDocument22 pagesCase Processing SummaryAsihPuspitaPutriNo ratings yet
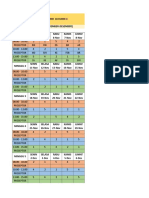
- JADWAL ASIH Copy 2Document2 pagesJADWAL ASIH Copy 2AsihPuspitaPutriNo ratings yet
- Influence of Pontic Design On Speech With An Anterior Fixed Dental Prosthesis, A Clinical Study and Finite Element AnalysisDocument9 pagesInfluence of Pontic Design On Speech With An Anterior Fixed Dental Prosthesis, A Clinical Study and Finite Element AnalysisAsihPuspitaPutriNo ratings yet
- Kegagalan GTC PDFDocument6 pagesKegagalan GTC PDFAsihPuspitaPutriNo ratings yet
- New Doc 2018-03-21 PDFDocument1 pageNew Doc 2018-03-21 PDFAsihPuspitaPutriNo ratings yet
- New Doc 2018-03-21 PDFDocument1 pageNew Doc 2018-03-21 PDFAsihPuspitaPutriNo ratings yet
- New Doc 2018-03-21Document1 pageNew Doc 2018-03-21AsihPuspitaPutriNo ratings yet
- New Doc 2018-04-16Document1 pageNew Doc 2018-04-16AsihPuspitaPutriNo ratings yet
- New Doc 2017-11-22Document25 pagesNew Doc 2017-11-22AsihPuspitaPutriNo ratings yet
- Kegagalan GTC PDFDocument6 pagesKegagalan GTC PDFAsihPuspitaPutriNo ratings yet
- New Doc 2017-11-22 PDFDocument25 pagesNew Doc 2017-11-22 PDFAsihPuspitaPutriNo ratings yet
- Jembatan AdhesifDocument5 pagesJembatan AdhesifAsihPuspitaPutriNo ratings yet
- LesiDocument31 pagesLesiAsihPuspitaPutriNo ratings yet
- Hand Lettering Letterform TemplateDocument1 pageHand Lettering Letterform TemplateMykovos0% (1)
- Pencetakan Dan Penatalaksanaan JaringanDocument8 pagesPencetakan Dan Penatalaksanaan JaringanAsihPuspitaPutriNo ratings yet
- Brush Lettering Practice Sheets DawnNicoleDesigns PDFDocument3 pagesBrush Lettering Practice Sheets DawnNicoleDesigns PDFAsihPuspitaPutriNo ratings yet
- Israels JCDADocument13 pagesIsraels JCDATiffany MonicaNo ratings yet
- 1169-1410158654 EmulsiDocument5 pages1169-1410158654 EmulsiAsihPuspitaPutriNo ratings yet
- ColorWorksheets DawnNicoleDesigns PDFDocument11 pagesColorWorksheets DawnNicoleDesigns PDFAsihPuspitaPutriNo ratings yet
- A Possible Plant Adaptogen: Rhodiola RoseaDocument10 pagesA Possible Plant Adaptogen: Rhodiola RoseaAsihPuspitaPutriNo ratings yet
- Israels JCDADocument13 pagesIsraels JCDATiffany MonicaNo ratings yet
- 1169-1410158654 EmulsiDocument5 pages1169-1410158654 EmulsiAsihPuspitaPutriNo ratings yet
- AttachmentDocument13 pagesAttachmentAsihPuspitaPutriNo ratings yet
- Hand Lettering Letterform TemplateDocument1 pageHand Lettering Letterform TemplateMykovos0% (1)
- Introduction of YNK Medical CorporationDocument19 pagesIntroduction of YNK Medical CorporationAsihPuspitaPutriNo ratings yet
- AttachmentDocument7 pagesAttachmentAsihPuspitaPutriNo ratings yet
- AttachmentDocument7 pagesAttachmentAsihPuspitaPutriNo ratings yet
- Breaking Emulsion (PDF)Document7 pagesBreaking Emulsion (PDF)adamsamodraNo ratings yet
- 225 FullDocument9 pages225 FullAsihPuspitaPutriNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- CX-5 BX-10 No. 1 & 1.5 Fluid Cylinder PartsDocument5 pagesCX-5 BX-10 No. 1 & 1.5 Fluid Cylinder PartsPierreNo ratings yet
- Typhoid FeverDocument9 pagesTyphoid FeverAli Al.JuffairiNo ratings yet
- ABS and Air Conditioner Wiring DiagramDocument207 pagesABS and Air Conditioner Wiring Diagramservice_00783% (30)
- TPB - Questionnaire Sample PDFDocument10 pagesTPB - Questionnaire Sample PDFhaneena kadeejaNo ratings yet
- HPC ReportDocument316 pagesHPC ReportmamansgNo ratings yet
- Usos HummusDocument36 pagesUsos HummusAlisson FernandaNo ratings yet
- Comparative Analysis of Mineral Constituents of Ethanol Leaf and SeedDocument9 pagesComparative Analysis of Mineral Constituents of Ethanol Leaf and SeedKIU PUBLICATION AND EXTENSIONNo ratings yet
- Duty Resume ReportDocument1 pageDuty Resume ReportaleemuddinNo ratings yet
- Ravi ProjectDocument92 pagesRavi ProjectAvinash Avii100% (1)
- Lecture 4 Part 1 PDFDocument11 pagesLecture 4 Part 1 PDFBashar AntriNo ratings yet
- Inu 2216 Idt - Question PaperDocument5 pagesInu 2216 Idt - Question PaperVinil JainNo ratings yet
- Climate and Cultural IdentityDocument2 pagesClimate and Cultural IdentityCha AbolucionNo ratings yet
- اللائحة التنظيمية لسفن الكروز - النسخة العربية - TransDocument10 pagesاللائحة التنظيمية لسفن الكروز - النسخة العربية - TranssalsabilNo ratings yet
- Norris Claire White Paper Liftware PDFDocument14 pagesNorris Claire White Paper Liftware PDFmeysam NaaNo ratings yet
- Frenny PDFDocument651 pagesFrenny PDFIftisam AjrekarNo ratings yet
- Neonatal Resuscitation: Dr. (Col) C.G.Wilson Professor& H.O.D (Paed)Document38 pagesNeonatal Resuscitation: Dr. (Col) C.G.Wilson Professor& H.O.D (Paed)shaharuddin_yahayaNo ratings yet
- PreparationDocument2 pagesPreparationmghaffarzadehNo ratings yet
- Pre Mocks Y11 2023Document14 pagesPre Mocks Y11 2023Ahsan AhmedNo ratings yet
- Teardrop by Lauren KateDocument47 pagesTeardrop by Lauren KateRandom House Teens88% (16)
- New Accreditation ToolsDocument52 pagesNew Accreditation ToolsLyle Guion Paguio100% (1)
- Research Paper - Perceptions of Grade 11 STEM Students Towards ContraceptivesDocument9 pagesResearch Paper - Perceptions of Grade 11 STEM Students Towards ContraceptivesKyle BinuyaNo ratings yet
- Cape Vincent Area Events January 2019Document5 pagesCape Vincent Area Events January 2019NewzjunkyNo ratings yet
- CoWIN Portal StepsDocument23 pagesCoWIN Portal StepsU VenkateshNo ratings yet
- Sister Letty G. Kuan Retirement and Role DiscontinuitiesDocument26 pagesSister Letty G. Kuan Retirement and Role DiscontinuitiesAbigail Faith Pretesto100% (1)
- Chapter-14 - Person and CareersDocument69 pagesChapter-14 - Person and CareersMarlon SagunNo ratings yet
- Modified Micro Marsupialization in Pediatric Patients: A Minimally Invasive TechniqueDocument4 pagesModified Micro Marsupialization in Pediatric Patients: A Minimally Invasive TechniquerinahpsNo ratings yet
- 004 VSL Datasheets US-ADocument22 pages004 VSL Datasheets US-Akmabd100% (1)
- Certificate of Analysis: Ship Date: Port of Discharge: Carrier: Vessel: Voyage: Quantity (MT) : Us GallonsDocument1 pageCertificate of Analysis: Ship Date: Port of Discharge: Carrier: Vessel: Voyage: Quantity (MT) : Us GallonsMercadeo BelaraviNo ratings yet
- 30 Natural Ways To Help Treat Polycystic Ovary SyndromeDocument12 pages30 Natural Ways To Help Treat Polycystic Ovary SyndromeArun AchalamNo ratings yet
- KGMC DirectoryDocument6 pagesKGMC DirectoryFaisal KhanNo ratings yet