You might also like
- Benefits and Risks of Antiretroviral TherapyDocument12 pagesBenefits and Risks of Antiretroviral TherapyAtgy Dhita AnggraeniNo ratings yet
- Ulkus Kornea Eng VerDocument15 pagesUlkus Kornea Eng VerDexter BluesNo ratings yet
- Activation of mTOR: A Culprit of Alzheimer's Disease?: Neuropsychiatric Disease and Treatment DoveDocument16 pagesActivation of mTOR: A Culprit of Alzheimer's Disease?: Neuropsychiatric Disease and Treatment Dovemr dexterNo ratings yet
- Nejmoa1606356 PDFDocument10 pagesNejmoa1606356 PDFDexter BluesNo ratings yet
- Pamj 24 182 PDFDocument5 pagesPamj 24 182 PDFDexter BluesNo ratings yet
- SDJ 2016 09 01 PDFDocument7 pagesSDJ 2016 09 01 PDFDexter BluesNo ratings yet
- Nejmoa1514762 PDFDocument12 pagesNejmoa1514762 PDFDexter BluesNo ratings yet
- PRM2016 1658172 PDFDocument7 pagesPRM2016 1658172 PDFDexter BluesNo ratings yet
- The Seven Cardinal MovementsDocument4 pagesThe Seven Cardinal MovementsDexter BluesNo ratings yet
- Childhood IQ and Bipolar Link PDFDocument9 pagesChildhood IQ and Bipolar Link PDFDexter BluesNo ratings yet
- Jurnal Anak Ririn PDFDocument10 pagesJurnal Anak Ririn PDFDexter BluesNo ratings yet
- Referat Obgyn FixDocument29 pagesReferat Obgyn FixDexter BluesNo ratings yet
- QuestionsDocument1 pageQuestionsDexter BluesNo ratings yet
- Jurnal Anak RirinDocument10 pagesJurnal Anak RirinDexter BluesNo ratings yet
- The Seven Cardinal MovementsDocument4 pagesThe Seven Cardinal MovementsDexter BluesNo ratings yet
- Fix ObgynDocument17 pagesFix ObgynDexter BluesNo ratings yet
- Unchallengeable Miracles of QuranDocument430 pagesUnchallengeable Miracles of QuranyoursincerefriendNo ratings yet
- Clinical Guidelines Acute Rehab Management 2010 InteractiveDocument172 pagesClinical Guidelines Acute Rehab Management 2010 InteractivenathanaelandryNo ratings yet
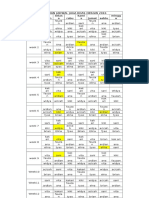
- Rincian Jadwal Jaga Koas Obsgin 2016 Senin Selas A Rabu Kami S Jumat Sabtu Mingg UDocument1 pageRincian Jadwal Jaga Koas Obsgin 2016 Senin Selas A Rabu Kami S Jumat Sabtu Mingg UDexter BluesNo ratings yet
- 1830 PDF PDFDocument5 pages1830 PDF PDFDexter BluesNo ratings yet
- TSWJ2015 803752 PDFDocument8 pagesTSWJ2015 803752 PDFDexter BluesNo ratings yet
- Childhood IQ and Bipolar Link PDFDocument9 pagesChildhood IQ and Bipolar Link PDFDexter BluesNo ratings yet
- The Seven Cardinal MovementsDocument3 pagesThe Seven Cardinal MovementsMaria Mandid0% (1)
- Referat Obgyn FixDocument29 pagesReferat Obgyn FixDexter BluesNo ratings yet
- Mood Dynamics in Bipolar Disorder: Research Open AccessDocument9 pagesMood Dynamics in Bipolar Disorder: Research Open AccesswulanfarichahNo ratings yet
- Pruritus: An Updated Look at An Old ProblemDocument7 pagesPruritus: An Updated Look at An Old ProblemThariq Mubaraq DrcNo ratings yet
- Geriatric Itch PDFDocument16 pagesGeriatric Itch PDFDexter BluesNo ratings yet
- Jurnal Elderly 2 PDFDocument3 pagesJurnal Elderly 2 PDFDexter BluesNo ratings yet
- 10 4103@0378-6323 116725 PDFDocument14 pages10 4103@0378-6323 116725 PDFDexter BluesNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Advanced Reading - Final TestsDocument9 pagesAdvanced Reading - Final TeststrandinhgiabaoNo ratings yet
- Distillery Safety Audit Report (Is 14489)Document24 pagesDistillery Safety Audit Report (Is 14489)Pankaj Goel100% (2)
- Genetically Modified Organisms and Biosafety PDFDocument47 pagesGenetically Modified Organisms and Biosafety PDFrinda78No ratings yet
- Assessing quality objectives in manufacturing through a case studyDocument13 pagesAssessing quality objectives in manufacturing through a case studyshinto LawrenceNo ratings yet
- Lesson PlanDocument1 pageLesson PlanNovah Mary A/P Guruloo IPGKTARNo ratings yet
- DepEd-Region III Schools Division of Tarlac Province Curriculum Audit Program (CAPDocument20 pagesDepEd-Region III Schools Division of Tarlac Province Curriculum Audit Program (CAPClaudine Manuel LibunaoNo ratings yet
- Introduce yourself and ask about languages in under 40 character guideDocument3 pagesIntroduce yourself and ask about languages in under 40 character guideyamileNo ratings yet
- 978 0 7503 5552 0.previewDocument22 pages978 0 7503 5552 0.previewAaiesha MohammedNo ratings yet
- Further Marking SchemeDocument17 pagesFurther Marking SchemeAreeba ImranNo ratings yet
- Learning Activity Sheet 1Document1 pageLearning Activity Sheet 1Bernadeth Dusal GuiasilonNo ratings yet
- Montessori's Four Planes of DevelopmentDocument2 pagesMontessori's Four Planes of DevelopmentDhagasol BahjaNo ratings yet
- ISO Green and Sustainable FinanceDocument9 pagesISO Green and Sustainable FinanceWilliams wamboNo ratings yet
- Rule Book Technical EventsDocument26 pagesRule Book Technical EventsGud GuyNo ratings yet
- Charts The Chart WizardDocument7 pagesCharts The Chart WizardFaishal HummamNo ratings yet
- KSCST Project ReportDocument10 pagesKSCST Project ReportGururaj Tavildar100% (3)
- Children S Functional Health Pattern Assessment Student 3Document7 pagesChildren S Functional Health Pattern Assessment Student 3Tommy PangandahengNo ratings yet
- Hilario-Marvin S - FS1 - E-PortfolioDocument5 pagesHilario-Marvin S - FS1 - E-PortfolioMARVIN HILARIONo ratings yet
- INX Future Inc Employee Performance DataDocument13 pagesINX Future Inc Employee Performance DataalfaNo ratings yet
- SURVEYING - 1 Short Answers IDocument5 pagesSURVEYING - 1 Short Answers IHarish MerugumalaNo ratings yet
- MSC Occupational Psychology Part ADocument12 pagesMSC Occupational Psychology Part Amasudur rahmanNo ratings yet
- TranslationDocument78 pagesTranslationdrmukhtiarbaigNo ratings yet
- ANALYSIS OF REHABILITATION PRIORITY FOR IRRIGATION INFRASTRUCTUREDocument8 pagesANALYSIS OF REHABILITATION PRIORITY FOR IRRIGATION INFRASTRUCTUREChristian PongsitammuNo ratings yet
- SW 1003398 NEC Article 311 Medium Voltage Conductors and Cables White Paper LODocument8 pagesSW 1003398 NEC Article 311 Medium Voltage Conductors and Cables White Paper LOwmkaneNo ratings yet
- Series Test-Ii November - 2021: Ilm College of Engineering & TechnologyDocument2 pagesSeries Test-Ii November - 2021: Ilm College of Engineering & TechnologyHOD ILM aeroNo ratings yet
- Csmgem Example ProblemsDocument8 pagesCsmgem Example Problemsh0s0No ratings yet
- Civil Engineering-CADDocument4 pagesCivil Engineering-CADjaneNo ratings yet
- Uts PDFDocument3 pagesUts PDFGiro AnthonyNo ratings yet
- Astm B571 97r08e1Document4 pagesAstm B571 97r08e1mspecsNo ratings yet
- YAS BeginnersGuidetoSwedishAcademiaDocument57 pagesYAS BeginnersGuidetoSwedishAcademiaD TTNo ratings yet
- RPMS Template - T1-T3Document29 pagesRPMS Template - T1-T3Deslene CasugayNo ratings yet