You might also like
- Optimal Control and Optimization of Stochastic Supply Chain SystemsFrom EverandOptimal Control and Optimization of Stochastic Supply Chain SystemsNo ratings yet
- SCM in HealthcareDocument9 pagesSCM in HealthcareAnurag GuptaNo ratings yet
- Outsourcing Technology In the Healthcare Industry: In Depth Research to Protect the Security, Technology, and Profitability of Your BusinessFrom EverandOutsourcing Technology In the Healthcare Industry: In Depth Research to Protect the Security, Technology, and Profitability of Your BusinessNo ratings yet
- INventory Management at Health CareDocument33 pagesINventory Management at Health CareishabihNo ratings yet
- Supply Chain Management in Clinical PharmacyDocument9 pagesSupply Chain Management in Clinical Pharmacyrragbir35No ratings yet
- Collaborative Implementation of E-Business Processes Within The Health-Care Supply ChainDocument10 pagesCollaborative Implementation of E-Business Processes Within The Health-Care Supply ChainEmmy SukhNo ratings yet
- Supply Chain Management in Healthcare IndustryDocument4 pagesSupply Chain Management in Healthcare IndustryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Apa AjasdsdsdsadsdsadsdadasdasdasddasdsdsadDocument15 pagesApa AjasdsdsdsadsdsadsdadasdasdasddasdsdsadIrwan WijayaNo ratings yet
- Innovative ExperienceDocument17 pagesInnovative ExperienceliliNo ratings yet
- Healthcare SCM in Malaysia - Case StudyDocument10 pagesHealthcare SCM in Malaysia - Case StudyHussain Alam100% (1)
- Important of Supply Chain Management in Healthcare OrganizationDocument3 pagesImportant of Supply Chain Management in Healthcare OrganizationAhmed KabirNo ratings yet
- Healthcare Supply Chain Management in Malaysia: A Case StudyDocument11 pagesHealthcare Supply Chain Management in Malaysia: A Case StudyPulkit BhardwajNo ratings yet
- Landry 2013Document18 pagesLandry 2013munishNo ratings yet
- Streamlining Distribution in The Pharmaceutical Industry: Life SciencesDocument16 pagesStreamlining Distribution in The Pharmaceutical Industry: Life SciencesBalaji RamasubramanianNo ratings yet
- Inventory Management Applications For Healthcare Supply ChainsDocument7 pagesInventory Management Applications For Healthcare Supply ChainsAjay tyagi IndianNo ratings yet
- Paper 8930Document5 pagesPaper 8930IJARSCT JournalNo ratings yet
- Inventory Management Issues in Health Care SupplyDocument34 pagesInventory Management Issues in Health Care SupplyYogesh ChandraNo ratings yet
- Improving healthcare supply chain efficiency in MaltaDocument11 pagesImproving healthcare supply chain efficiency in MaltanaziaNo ratings yet
- Silo - Tips - Supply Chain Management in Hospital A Case StudyDocument7 pagesSilo - Tips - Supply Chain Management in Hospital A Case Study398Rishabh RajNo ratings yet
- Health Care MGTDocument13 pagesHealth Care MGTRicha SinghNo ratings yet
- Supply Chain Management in The Healthcare IndustryDocument23 pagesSupply Chain Management in The Healthcare IndustryMohammed Al Ayoubi67% (3)
- 2023 BialasDocument11 pages2023 BialasFaradisa AyuNo ratings yet
- Information Flow in Pharma Supply ChainDocument6 pagesInformation Flow in Pharma Supply ChainPika ChuNo ratings yet
- Not Your Fathers Supply ChainDocument4 pagesNot Your Fathers Supply Chainkhadden999No ratings yet
- Vendor Managed Inventory (VMI) Evidences From Lean Deployment in HealthcareDocument18 pagesVendor Managed Inventory (VMI) Evidences From Lean Deployment in HealthcareRicardo BalauNo ratings yet
- Inventory ManagementDocument9 pagesInventory ManagementShikhaNo ratings yet
- IJPR - Volume 18 - Issue 2 - Pages 1103-1116Document14 pagesIJPR - Volume 18 - Issue 2 - Pages 1103-1116AllanNo ratings yet
- Running Head: Proposal: Use of Technology in Health Care 1Document4 pagesRunning Head: Proposal: Use of Technology in Health Care 1Evans MettoNo ratings yet
- Assignment HintDocument14 pagesAssignment HintMuhammad Anwar HussainNo ratings yet
- Supply-Chain Management and Health Care Delivery - Pursuing A System-Level Understanding - Building A Better Delivery System - NCBI BookshelfDocument4 pagesSupply-Chain Management and Health Care Delivery - Pursuing A System-Level Understanding - Building A Better Delivery System - NCBI BookshelfDennis DuNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument23 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDiahNo ratings yet
- Essentials For Information Coordination in Supply Chain SystemsDocument5 pagesEssentials For Information Coordination in Supply Chain SystemsSreejith SankarNo ratings yet
- Pharmaceutical Supply Chain and Inventory Management Strategies PDFDocument13 pagesPharmaceutical Supply Chain and Inventory Management Strategies PDFRizky AzizahNo ratings yet
- SPS Apollo Hospital Inventory Management ChallengesDocument4 pagesSPS Apollo Hospital Inventory Management ChallengesRohit KumarNo ratings yet
- Logistics in Hospitals: A Case Study of Some Singapore HospitalsDocument13 pagesLogistics in Hospitals: A Case Study of Some Singapore HospitalsSapta YudhaNo ratings yet
- Iyengar 2009Document7 pagesIyengar 2009柏元邱No ratings yet
- 1 s2.0 S1551741116300912 MainDocument4 pages1 s2.0 S1551741116300912 Mainmaryrose menderoNo ratings yet
- Basic Functions of Healthcare FieldDocument10 pagesBasic Functions of Healthcare FieldShraddha BendkhaleNo ratings yet
- An Exploratory of Healthcare Supply ChainDocument15 pagesAn Exploratory of Healthcare Supply ChainMarisa KritchanchaiNo ratings yet
- Supply Chain Management in HospitalsDocument6 pagesSupply Chain Management in HospitalsAbhra100% (10)
- Development of A Drug Inventory System ADocument20 pagesDevelopment of A Drug Inventory System AMuhammad Baba GoniNo ratings yet
- How Inventory Techniques Impact Procurement at Kenyan HospitalsDocument10 pagesHow Inventory Techniques Impact Procurement at Kenyan HospitalsElias KumeloNo ratings yet
- Effective Demand Forecasting in HealthcareDocument4 pagesEffective Demand Forecasting in HealthcareDivya v bNo ratings yet
- Strategi Operasi RUmah SakitDocument4 pagesStrategi Operasi RUmah SakituddindjmNo ratings yet
- Supply Chain Management in Health Servic PDFDocument7 pagesSupply Chain Management in Health Servic PDFSa Be MirNo ratings yet
- Johnson Johnson Supply Chain Challenges FinalDocument14 pagesJohnson Johnson Supply Chain Challenges Finalreva_radhakrish1834No ratings yet
- Inventory Management of Medical Consumables in Public Hospital: A Case StudyDocument6 pagesInventory Management of Medical Consumables in Public Hospital: A Case Studybagyi111No ratings yet
- Risks of Supply Chain Management in Pharmaceutical CompaniesDocument11 pagesRisks of Supply Chain Management in Pharmaceutical CompaniesrifatNo ratings yet
- Healthcare Logistics and Supply Chain Issues and Future ChallengesDocument4 pagesHealthcare Logistics and Supply Chain Issues and Future Challengespallavi mehraNo ratings yet
- BCI Industry ReportDocument20 pagesBCI Industry ReportVivek Prakash100% (1)
- Mathematics: Inventory Management at A Chilean Hospital Pharmacy: Case Study of A Dynamic Decision-Aid ToolDocument20 pagesMathematics: Inventory Management at A Chilean Hospital Pharmacy: Case Study of A Dynamic Decision-Aid ToolDiana CapistranoNo ratings yet
- Healthcare Supply Chain ManagementDocument3 pagesHealthcare Supply Chain ManagementRizwan AhmedNo ratings yet
- Healthcare Supply Chain and IS Strategies For Improved Outcomes David D. DobrzykowskiDocument20 pagesHealthcare Supply Chain and IS Strategies For Improved Outcomes David D. DobrzykowskisrikantNo ratings yet
- Libyan International Medical University Faculty of Business AdministrationDocument8 pagesLibyan International Medical University Faculty of Business AdministrationmariamNo ratings yet
- E-Procurement in Hospital Pharmacies: An Exploratory Multi-Case Study From SwitzerlandDocument16 pagesE-Procurement in Hospital Pharmacies: An Exploratory Multi-Case Study From SwitzerlandPrudhvinadh KopparapuNo ratings yet
- Manuscript IJBPSCMDocument14 pagesManuscript IJBPSCMSiwaporn KunnapapdeelertNo ratings yet
- Healthcare Supply ChainDocument351 pagesHealthcare Supply ChainLiêm LaNo ratings yet
- Ambrosus Pharmacy v2Document15 pagesAmbrosus Pharmacy v2cipriano2No ratings yet
- Impact of Inventory Management on Health Service DeliveryDocument11 pagesImpact of Inventory Management on Health Service DeliveryClifford OwusuNo ratings yet
- Forecasting & Inventory Control PDFDocument260 pagesForecasting & Inventory Control PDFdeepti ramdinNo ratings yet
- New Trends in Supply ChainDocument12 pagesNew Trends in Supply Chaindeepti ramdinNo ratings yet
- Information Technology in Supply Chain ManagementDocument14 pagesInformation Technology in Supply Chain Managementdeepti ramdin100% (1)
- Information Technology in Supply Chain ManagementDocument14 pagesInformation Technology in Supply Chain Managementdeepti ramdin100% (1)
- How To Evaluate A CompanyDocument15 pagesHow To Evaluate A CompanyJaanvi BhatiaNo ratings yet
- New Trends in Supply ChainDocument12 pagesNew Trends in Supply Chaindeepti ramdinNo ratings yet
- Case MethodDocument18 pagesCase MethodrohitwebNo ratings yet
- Design of Inventory Management System For Consumable Medical SuppliesDocument15 pagesDesign of Inventory Management System For Consumable Medical Suppliesdeepti ramdinNo ratings yet
- New Trends in Supply ChainDocument12 pagesNew Trends in Supply Chaindeepti ramdinNo ratings yet
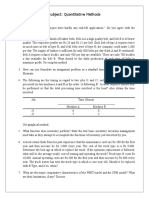
- Quantitative MethodsDocument2 pagesQuantitative Methodsdeepti ramdinNo ratings yet
- Finance ManagementDocument17 pagesFinance Managementdeepti ramdin0% (1)
- Business LawDocument1 pageBusiness Lawdeepti ramdinNo ratings yet
- Case MethodDocument18 pagesCase MethodrohitwebNo ratings yet