You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- National Health Programmes For Children in IndiaDocument79 pagesNational Health Programmes For Children in IndiashahnazNo ratings yet
- 4 Ways To Get Higher Marks in Exams - Wikihow PDFDocument6 pages4 Ways To Get Higher Marks in Exams - Wikihow PDFNAGU2009No ratings yet
- My Rights, My Voice Afghanistan Project OverviewDocument4 pagesMy Rights, My Voice Afghanistan Project OverviewOxfamNo ratings yet
- Baruya High School: Reports Called For Date Submitted Recorded byDocument1 pageBaruya High School: Reports Called For Date Submitted Recorded byLiezl SabadoNo ratings yet
- Presidential Decree No. 603, The Child and Youth Welfare CodeDocument62 pagesPresidential Decree No. 603, The Child and Youth Welfare CodeRonna Lamac-Ador100% (1)
- HSE-001 HSE MS Rev1.0 EngDocument12 pagesHSE-001 HSE MS Rev1.0 EngMIGUEL MIGUEL RIVAS SALCEDONo ratings yet
- Ass2 - Prefixes Suffixes - Lesson Plan 2Document3 pagesAss2 - Prefixes Suffixes - Lesson Plan 2api-267904090No ratings yet
- The Self From Various Perspective PsychologyDocument36 pagesThe Self From Various Perspective PsychologyRhea Dela CruzNo ratings yet
- ScratchDocument33 pagesScratchYordanka Stoyanova100% (1)
- Mathematics: Quarter 2 - Module 9: Solve Equations Involving Radical ExpressionsDocument24 pagesMathematics: Quarter 2 - Module 9: Solve Equations Involving Radical ExpressionsKitkattyNo ratings yet
- AMERICAN Education SystemDocument28 pagesAMERICAN Education SystemMOHAMMAD JALAL UDDIN RUMINo ratings yet
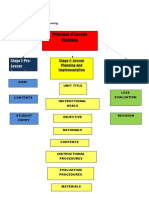
- Principal of Lesson Planning: Stage 1: Pre-Lesson PreparationDocument6 pagesPrincipal of Lesson Planning: Stage 1: Pre-Lesson Preparationjaysel86No ratings yet
- Bucal National High School-ShsDocument21 pagesBucal National High School-ShsJohn Carlo Colipat80% (5)
- Personal Trainer Certification, 2019Document1 pagePersonal Trainer Certification, 2019Amira ElshandidiNo ratings yet
- The MatsDocument3 pagesThe MatsReyniel VergaraNo ratings yet
- Annette Youngkin - Curriculum Overview - First DraftDocument4 pagesAnnette Youngkin - Curriculum Overview - First Draftapi-326132451No ratings yet
- Professional Nurse PractitionerDocument8 pagesProfessional Nurse PractitionerDanily Faith VillarNo ratings yet
- Ogunbiyi - ThesisDocument149 pagesOgunbiyi - ThesisOgunbiyi David OluwabukunmiNo ratings yet
- March 15 CuFDocument2 pagesMarch 15 CuFelkashien.mendoza001No ratings yet
- My Interpersonal Communication Plan-Adrián Arias A01451234Document2 pagesMy Interpersonal Communication Plan-Adrián Arias A01451234Adrian Arias MarínNo ratings yet
- IPlan Present ContinuousDocument2 pagesIPlan Present ContinuousJai-jaiNo ratings yet
- URICA ChangeDocument3 pagesURICA Changeclaudiaolareanu100% (1)
- Orca Share Media1682387604713 7056445059999513745Document54 pagesOrca Share Media1682387604713 7056445059999513745ALUNDAY, MELODY S.No ratings yet
- ThoughtsDocument651 pagesThoughtsOdoricoNo ratings yet
- The Impact of Physical Facilities On Students' Level of Motivation and Academic Performance in Senior Secondary Schools in South West NigeriaDocument5 pagesThe Impact of Physical Facilities On Students' Level of Motivation and Academic Performance in Senior Secondary Schools in South West NigeriaLeo NardoNo ratings yet
- TPR Lesson PlanDocument4 pagesTPR Lesson Planapi-310070697100% (1)
- B. Sc. CSIT Final Year Project Work:: Structuring Report, Presentation and EvaluationDocument41 pagesB. Sc. CSIT Final Year Project Work:: Structuring Report, Presentation and EvaluationDhiraj JhaNo ratings yet
- GPFS Frequently Asked Questions and AnswersDocument44 pagesGPFS Frequently Asked Questions and AnswersBrianSeungminHwangNo ratings yet
- The Use of Non-Verbal Communication in The ClassroomDocument4 pagesThe Use of Non-Verbal Communication in The ClassroomWak EncikNo ratings yet
- Kalle Miller - Prometheus Camps As An Alternative To Finnish Confirmation CampsDocument7 pagesKalle Miller - Prometheus Camps As An Alternative To Finnish Confirmation CampsconstantinecartmanNo ratings yet