You might also like
- Diuretics: Generic and Brand NamesDocument22 pagesDiuretics: Generic and Brand NamesKish GabrielNo ratings yet
- Brat Er 2000Document13 pagesBrat Er 2000Carla MantillaNo ratings yet
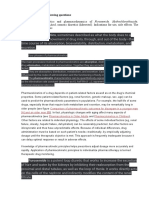
- Pharmacokinetics and Pharmacodynamics of DiureticsDocument21 pagesPharmacokinetics and Pharmacodynamics of DiureticsFaheem MusthafaNo ratings yet
- Renal SystemDocument39 pagesRenal SystemJhennie Rose PalaganasNo ratings yet
- Diuretic and Urinary Alkalizes-Dr - Jibachha Sah, M.V.SC (Vet - Pharmacology)Document23 pagesDiuretic and Urinary Alkalizes-Dr - Jibachha Sah, M.V.SC (Vet - Pharmacology)jibachha sahNo ratings yet
- Jigar Patel Et Al, 2007. Optimal Use of Diuretics in HFDocument11 pagesJigar Patel Et Al, 2007. Optimal Use of Diuretics in HFMuhammad Isnaini ZuhriNo ratings yet
- DiureticsDocument3 pagesDiureticsCarl Simon CalingacionNo ratings yet
- Pcol Exp 9Document18 pagesPcol Exp 9windgazer07No ratings yet
- Unit 04: Drugs Acting On The Renal System Diuretic Agents: Thiazide and Thiazide-Like DiureticsDocument8 pagesUnit 04: Drugs Acting On The Renal System Diuretic Agents: Thiazide and Thiazide-Like DiureticsDental LecturesMMQNo ratings yet
- Diuretic Drug: First Semester 2019-2020 College of Dentistry University of HailDocument5 pagesDiuretic Drug: First Semester 2019-2020 College of Dentistry University of HailMaha NoorNo ratings yet
- Diuretic Drugs: Prof - Dr.M.Aydın BarlasDocument10 pagesDiuretic Drugs: Prof - Dr.M.Aydın Barlasnasan shehadaNo ratings yet
- DiureticsDocument61 pagesDiureticsJoyce WacukaNo ratings yet
- 10 3 2020 Diuretics Clinical Practice PDFDocument16 pages10 3 2020 Diuretics Clinical Practice PDFtupuNo ratings yet
- Topic - Diuretics: Submitted By, Group - 07Document28 pagesTopic - Diuretics: Submitted By, Group - 07Arvi KhanNo ratings yet
- Loop diuretics: Dosing and major side effects (uptodate)Document15 pagesLoop diuretics: Dosing and major side effects (uptodate)kabulkabulovich5No ratings yet
- Diuretics and Anti Diuretics: Year Iii Pharm.D Dr. V. ChitraDocument49 pagesDiuretics and Anti Diuretics: Year Iii Pharm.D Dr. V. ChitranikithaNo ratings yet
- DiureticsDocument3 pagesDiureticsarshu98172No ratings yet
- DiureticsDocument2 pagesDiureticsClophia LidresNo ratings yet
- DiureticsDocument21 pagesDiureticsShathawe BrgNo ratings yet
- Herbal Plants Used As Diuretics: A Comprehensive ReviewDocument6 pagesHerbal Plants Used As Diuretics: A Comprehensive ReviewNoviiaayulestariiNo ratings yet
- Diuretici U Bubrežnoj InsuficijencijiDocument5 pagesDiuretici U Bubrežnoj InsuficijencijiBastaDaninocNo ratings yet
- Journal 3 Diuretic in Heart FailureDocument6 pagesJournal 3 Diuretic in Heart FailureClara Nur RamadhaniNo ratings yet
- Diuretics: By: Prof. A. AlhaiderDocument33 pagesDiuretics: By: Prof. A. AlhaiderNina KerafNo ratings yet
- Candidate - Renal Mechanisms of Diuretic Resistance in CongestiveDocument17 pagesCandidate - Renal Mechanisms of Diuretic Resistance in CongestiveBhanu KumarNo ratings yet
- Diuretic: Hazha S. Ameen MSCDocument17 pagesDiuretic: Hazha S. Ameen MSCAhmed MohamadNo ratings yet
- Diuretics: BY-DR. Saurabh Kansal Dept. of Pharmacology Msy Medical College MeerutDocument33 pagesDiuretics: BY-DR. Saurabh Kansal Dept. of Pharmacology Msy Medical College MeerutPrakhar GoelNo ratings yet
- Final 1journal Publication Matter Sameer - Copy PrintDocument25 pagesFinal 1journal Publication Matter Sameer - Copy PrintVaibhav ShendeNo ratings yet
- Diuretics: Sumolly Anak DavidDocument29 pagesDiuretics: Sumolly Anak Davidfarmasi_hmNo ratings yet
- Diuretics: Basic Pharmacology Block Pdnt/Pmed - PMSC/PPHR - 213Document19 pagesDiuretics: Basic Pharmacology Block Pdnt/Pmed - PMSC/PPHR - 213JedoNo ratings yet
- Diuretics1 (Autosaved)Document19 pagesDiuretics1 (Autosaved)Pharmanic By Ruttaba FatimaNo ratings yet
- Therapeutic Uses of Diuretic Agents - StatPearls - NCBI BookshelfDocument30 pagesTherapeutic Uses of Diuretic Agents - StatPearls - NCBI Bookshelfbook ideaNo ratings yet
- Drug Therapy: Review ArticleDocument9 pagesDrug Therapy: Review ArticleMuhammad Halil GibranNo ratings yet
- Urinary Physiology Assignment - EditedDocument4 pagesUrinary Physiology Assignment - EditedDavis KobiaNo ratings yet
- DiureticsDocument6 pagesDiureticsJihad AnadNo ratings yet
- DiureticsDocument83 pagesDiureticsKarami BrutusNo ratings yet
- RRR Pharma- Part 2Document402 pagesRRR Pharma- Part 2archana singhNo ratings yet
- Diuretics and Their Mechanism of Action in the NephronDocument52 pagesDiuretics and Their Mechanism of Action in the NephronKulgaurav RegmiNo ratings yet
- ABC of Heart Failure Management Diruretics ACE Inhibitors and NotratesDocument4 pagesABC of Heart Failure Management Diruretics ACE Inhibitors and Notratesgroup38No ratings yet
- PHAR406 PHARMACEUTICAL CHEMISTRY IV DIURETICSDocument74 pagesPHAR406 PHARMACEUTICAL CHEMISTRY IV DIURETICSYousef AhmedNo ratings yet
- Diuretics 1Document34 pagesDiuretics 1ياسمين مجديNo ratings yet
- Renal Note On DiureticsDocument12 pagesRenal Note On DiureticsLilian EdeniNo ratings yet
- DiureticsDocument1 pageDiureticslilipop_xtream91No ratings yet
- For The Clinician: Clinical Pharmacology in Diuretic UseDocument10 pagesFor The Clinician: Clinical Pharmacology in Diuretic UseSrinivas PingaliNo ratings yet
- Diuretics: A. Overview of The Clinical Use of Diuretics B. Classification of DiureticsDocument22 pagesDiuretics: A. Overview of The Clinical Use of Diuretics B. Classification of DiureticsSteven GonzalesNo ratings yet
- DiureticsDocument42 pagesDiureticsKeziah TampusNo ratings yet
- Diureticos y El RiñonDocument8 pagesDiureticos y El RiñonIrving MeraNo ratings yet
- DiureticsDocument18 pagesDiureticsChantal CarnesNo ratings yet
- Diuretics and Drugs Affecting Renal Function, Water, and Electrolyte MetabolismDocument4 pagesDiuretics and Drugs Affecting Renal Function, Water, and Electrolyte MetabolismWaqar HassanNo ratings yet
- Everything You Need to Know About Loop DiureticsDocument6 pagesEverything You Need to Know About Loop DiureticsNabila AfiliaNo ratings yet
- Art EvaDocument5 pagesArt EvaarmanitoNo ratings yet
- Gastrointestinal Drugs: Prof. Dr. Muhammad Ashraf Dean FBS Professor of Pharmacology and Toxicology UVAS, LahoreDocument33 pagesGastrointestinal Drugs: Prof. Dr. Muhammad Ashraf Dean FBS Professor of Pharmacology and Toxicology UVAS, LahoreMuhammad Shahid BilalNo ratings yet
- Thiazide-Induced Hyponatremia: ReviewDocument7 pagesThiazide-Induced Hyponatremia: ReviewFabio ParadaNo ratings yet
- DiureticsDocument1 pageDiureticsMa Cristina MirandaNo ratings yet
- Drugs Acting On: Renal SystemDocument75 pagesDrugs Acting On: Renal SystemCarlojay IniegoNo ratings yet
- DiureticsDocument2 pagesDiureticsArnel Leonard TungbabanNo ratings yet
- Diuretics MergedDocument727 pagesDiuretics MergedRinkiNo ratings yet
- Diuretics: An Overview of How They Work and Their ClassificationDocument74 pagesDiuretics: An Overview of How They Work and Their Classificationm1k0e100% (1)
- Diuretics PCMDocument8 pagesDiuretics PCMAnuj panditNo ratings yet
- 1 - Renal Excretion of DrugsDocument18 pages1 - Renal Excretion of DrugsKashar SaeedNo ratings yet
- Paliative CareDocument402 pagesPaliative CarewardahNo ratings yet
- Metabolic Acidosis: Irish Grace A. Dayao Dra. RamosDocument14 pagesMetabolic Acidosis: Irish Grace A. Dayao Dra. RamosBing DayaoNo ratings yet
- Peripheral Retinal Degenerations and Their ManagementDocument32 pagesPeripheral Retinal Degenerations and Their Managementmanognaaaa100% (1)
- Case Study On EpilepsyDocument2 pagesCase Study On Epilepsyabirami pNo ratings yet
- 2021 The Enigma of Persistent Symptoms in Hypothyroid PatientsDocument8 pages2021 The Enigma of Persistent Symptoms in Hypothyroid PatientsPeter Albeiro Falla CortesNo ratings yet
- Enzymes For Health and LongevityDocument118 pagesEnzymes For Health and LongevitydieBiene100% (2)
- ENGLISH 6 - Q1 - W5 - Mod5 - Make Connection Between Information ViewDocument15 pagesENGLISH 6 - Q1 - W5 - Mod5 - Make Connection Between Information Viewerma rose hernandezNo ratings yet
- Family-Oriented Primary CareDocument16 pagesFamily-Oriented Primary CareMwanja MosesNo ratings yet
- FengShui Inspection IDocument52 pagesFengShui Inspection IDavid Hu100% (3)
- CDHO Factsheet Rheumatoid ArthritisDocument3 pagesCDHO Factsheet Rheumatoid ArthritisHenry MandalasNo ratings yet
- Rectovagina FistulaDocument13 pagesRectovagina FistulaNurul HikmahNo ratings yet
- American Thoracic Society Cigarette Smoking and Health 2Document5 pagesAmerican Thoracic Society Cigarette Smoking and Health 2miftahul masruriNo ratings yet
- History TakingDocument13 pagesHistory TakingSirajum MuneeraNo ratings yet
- Lecture III-1 Laws of Inheritance Patterns of InheritanceDocument18 pagesLecture III-1 Laws of Inheritance Patterns of InheritanceJÜnn BatacNo ratings yet
- Airline Ground Safety Panel: Toolbox TalkDocument3 pagesAirline Ground Safety Panel: Toolbox TalkRohit SinghNo ratings yet
- CCC 18Document322 pagesCCC 18Thiru Navukarasu100% (1)
- Profesional AnamnesisDocument2 pagesProfesional AnamnesisAna MariaNo ratings yet
- Preventing Non-Communicable Diseases Through Lifestyle ChangesDocument12 pagesPreventing Non-Communicable Diseases Through Lifestyle ChangesMeycauayan NHS (Region III - Meycauayan City)No ratings yet
- Social Anxiety Disorder 1.editedDocument4 pagesSocial Anxiety Disorder 1.editedmoureenNo ratings yet
- Journal Reading Ilmu Penyakit DalamDocument15 pagesJournal Reading Ilmu Penyakit DalamSeffia riandiniNo ratings yet
- Datafortress 2020 - Interlock Unlimited - Drug Lab UnlimitedDocument13 pagesDatafortress 2020 - Interlock Unlimited - Drug Lab UnlimitedSokoliak 010010110No ratings yet
- Management of Breast FeedingDocument17 pagesManagement of Breast FeedingUday KumarNo ratings yet
- Community PDFDocument12 pagesCommunity PDFJaja D. JimenezNo ratings yet
- Positive Language Guide - 0Document22 pagesPositive Language Guide - 0Xristos BeretisNo ratings yet
- PAFP Consensus Guidelines On Preparation and Resumption of Clinic Services - FINALDocument17 pagesPAFP Consensus Guidelines On Preparation and Resumption of Clinic Services - FINALPatricia Franco-VillaNo ratings yet
- Roxithromycin TabletDocument13 pagesRoxithromycin Tabletno debedeNo ratings yet
- CARDIOLOGY PHYSICAL EXAM GUIDEDocument4 pagesCARDIOLOGY PHYSICAL EXAM GUIDEAxinte Catalina PaulaNo ratings yet
- Peripheral Vascular DiseaseDocument53 pagesPeripheral Vascular DiseaseShenbagam Mahalingam100% (1)
- World Hunger Web QuestDocument5 pagesWorld Hunger Web Questapi-313403351No ratings yet
- Complications of DiabetesDocument3 pagesComplications of Diabetesa7wfNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)