You might also like
- PLE 2019 - Medicine Questions and Answer KeyDocument24 pagesPLE 2019 - Medicine Questions and Answer KeydicksonNo ratings yet
- 8 Part Eye Exam RevisedDocument17 pages8 Part Eye Exam RevisedpasambalyrradjohndarNo ratings yet
- 8 Part Eye Exam RevisedDocument17 pages8 Part Eye Exam RevisedpasambalyrradjohndarNo ratings yet
- Laboratory Handbook PDFDocument184 pagesLaboratory Handbook PDFReymi Then50% (2)
- Pre-Surgical Hand WashDocument2 pagesPre-Surgical Hand WashRatna LamaNo ratings yet
- Accuracy of Observations and MeasurementsDocument5 pagesAccuracy of Observations and MeasurementsJoher MendezNo ratings yet
- Activity 2 Study Guide Questions WEEK 6 CHN 2 FERRER JOHN DENVER A.Document7 pagesActivity 2 Study Guide Questions WEEK 6 CHN 2 FERRER JOHN DENVER A.Novelyn PuaNo ratings yet
- Ebm Quiz March 2023Document39 pagesEbm Quiz March 2023Mark KerrNo ratings yet
- The Concept of Sensitivity and Specificity in Relation To Two Types of Errors and Its Application in Medical ResearchDocument6 pagesThe Concept of Sensitivity and Specificity in Relation To Two Types of Errors and Its Application in Medical ResearchNurul FadliaNo ratings yet
- 4310 Exam 2Document11 pages4310 Exam 2Hung PhanNo ratings yet
- NVS ScriptDocument2 pagesNVS ScriptisaacpapicaNo ratings yet
- Ethics and Biostats Uworld NotesDocument9 pagesEthics and Biostats Uworld NotesNada AK100% (1)
- Prijono Satya Bakti Epidemiology Department University of AirlanggaDocument29 pagesPrijono Satya Bakti Epidemiology Department University of AirlanggapuskesmasNo ratings yet
- WEEK 10: Strategies in Epidemiology Measurements and Measurement of Errors Assessing Evidence of Disease CausationDocument3 pagesWEEK 10: Strategies in Epidemiology Measurements and Measurement of Errors Assessing Evidence of Disease CausationKezia MadeloNo ratings yet
- Epidemiology Strategies for Disease PreventionDocument3 pagesEpidemiology Strategies for Disease Preventiongene2693No ratings yet
- CASE-FORMAT-2024-REVISEDDocument10 pagesCASE-FORMAT-2024-REVISEDGave gonzalesNo ratings yet
- EBM QUIZ Oct 2023Document41 pagesEBM QUIZ Oct 2023Mark KerrNo ratings yet
- Scientific Method PowerpointDocument27 pagesScientific Method PowerpointKemoy FrancisNo ratings yet
- ST NDDocument9 pagesST NDOtiosse MyosotisNo ratings yet
- BIOE Week 13Document3 pagesBIOE Week 13FelicityNo ratings yet
- 2.01 Measures of Disease FrequencyDocument6 pages2.01 Measures of Disease Frequencygene2693No ratings yet
- IDC 213 02 Workshop On Appraisal of Articles On TherapyDocument4 pagesIDC 213 02 Workshop On Appraisal of Articles On TherapyFort SalvadorNo ratings yet
- 16a Permenkes No 75 Lampiran TTG PuskesmasDocument26 pages16a Permenkes No 75 Lampiran TTG PuskesmasDesak PratiwiNo ratings yet
- Epidemiology and The NurseDocument26 pagesEpidemiology and The NurseCris Melric Palanog100% (3)
- 2.3 Cohort StudiesDocument6 pages2.3 Cohort StudiesMiguel C. Dolot100% (1)
- Lecture 4 & 5. Epidemiological StudiesDocument58 pagesLecture 4 & 5. Epidemiological StudiesHaneen Al-HajjNo ratings yet
- STUDENT NOTES: Biostatistics and Epidemiology: Davao Doctors College Medical Laboratory Science DepartmentDocument5 pagesSTUDENT NOTES: Biostatistics and Epidemiology: Davao Doctors College Medical Laboratory Science Departmentghost criticNo ratings yet
- Quiz PR2Document3 pagesQuiz PR2Renz Ferrer100% (1)
- Analytical EpidemiologyDocument7 pagesAnalytical EpidemiologySamridhi SrivastavaNo ratings yet
- (EPI) 1.01 - Overview of Epidemiology & Descriptive Epidemiology - Dr. ButacanDocument5 pages(EPI) 1.01 - Overview of Epidemiology & Descriptive Epidemiology - Dr. Butacanpasambalyrradjohndar0% (1)
- Scientific Method-StudDocument14 pagesScientific Method-StudCoco BelarminoNo ratings yet
- Sample:: Based On The HPI Alone, The Physician Should Already Have An Initial Impression and Differential DiagnosisDocument13 pagesSample:: Based On The HPI Alone, The Physician Should Already Have An Initial Impression and Differential DiagnosisNorman Vryne CaduaNo ratings yet
- Q3, Week 4Document2 pagesQ3, Week 4Lea LaceNo ratings yet
- EPI 2.05 Overview of Analytic Observational StudiesDocument7 pagesEPI 2.05 Overview of Analytic Observational StudiesJoher MendezNo ratings yet
- Methods and Data: An SEO-Optimized TitleDocument4 pagesMethods and Data: An SEO-Optimized TitleJesus Manuel NavidadNo ratings yet
- EPI 1.02 Common Health Indices in The CommunityDocument9 pagesEPI 1.02 Common Health Indices in The CommunityJoher MendezNo ratings yet
- DAVC Medical Lab Science Student Notes on Biostatistics and EpidemiologyDocument5 pagesDAVC Medical Lab Science Student Notes on Biostatistics and Epidemiologysilvestre bolosNo ratings yet
- Specificity 100 X No - of Dse Individual WithDocument4 pagesSpecificity 100 X No - of Dse Individual WithmarianNo ratings yet
- Critical Appraisal ChecklistDocument9 pagesCritical Appraisal Checklisttias nurainiNo ratings yet
- Scientific Method PowerPointDocument26 pagesScientific Method PowerPointMark Francis HernandezNo ratings yet
- Lecture 7 Study DesignsDocument86 pagesLecture 7 Study DesignsKhalil UllahNo ratings yet
- OutbreakDocument5 pagesOutbreakMohammed Atif AbdulghafarNo ratings yet
- Ranibizumab vs Laser Therapy for Very Low Birthweight Infants with ROPDocument2 pagesRanibizumab vs Laser Therapy for Very Low Birthweight Infants with ROPDaihachi DaimeNo ratings yet
- IDC 213 06 Workshop 3 Critical Appraisal On Studies About HarmDocument5 pagesIDC 213 06 Workshop 3 Critical Appraisal On Studies About HarmFort SalvadorNo ratings yet
- Research DesignsDocument5 pagesResearch DesignsMark Vincent SahagunNo ratings yet
- Epi-Lessons 5Document44 pagesEpi-Lessons 5Najeeb haiderNo ratings yet
- Activity in Practical Research 2Document2 pagesActivity in Practical Research 2Aimee ArcillaNo ratings yet
- Nursing Process EBN Format OB PEDIADocument5 pagesNursing Process EBN Format OB PEDIAAnn Nicole UlitNo ratings yet
- FSS 102Document21 pagesFSS 102molayomoradekeNo ratings yet
- Nursing Process EBN Format OB PEDIADocument5 pagesNursing Process EBN Format OB PEDIAChezka Orton Swift BolintiamNo ratings yet
- Research Methods in Psychology: Deduction vs InductionDocument11 pagesResearch Methods in Psychology: Deduction vs Inductiondewani mastaniNo ratings yet
- Epidemiology and Biostatistics CourseDocument7 pagesEpidemiology and Biostatistics CourseDehnzel de LeonNo ratings yet
- Acute PainDocument4 pagesAcute PainRuffy AbdulazisNo ratings yet
- 2: Measurement: 2.1 Types of Variables and Measurement ScalesDocument14 pages2: Measurement: 2.1 Types of Variables and Measurement ScalesJuan Sebastián Galindo SánchezNo ratings yet
- Disease Outbreak InvestigationDocument4 pagesDisease Outbreak Investigationkoass100% (1)
- Ha 1Document4 pagesHa 1Alyssa MontimorNo ratings yet
- Communicable Disease Prevention at San Juan NationalDocument7 pagesCommunicable Disease Prevention at San Juan NationalAiza May RosasNo ratings yet
- QMMDocument54 pagesQMMgladwin thomasNo ratings yet
- Administrative Round PHC - SummarizedDocument36 pagesAdministrative Round PHC - SummarizedTAREQ MOHAMMEDNo ratings yet
- 453 FullDocument8 pages453 FullRandriamiharyNo ratings yet
- Chapter 4Document11 pagesChapter 4Oneng IfayaniNo ratings yet
- Dr. Faryal Razzaq DR - Faryal@szabist-Isb - Edu.pk: Advance Research Methods Lecture 5Document18 pagesDr. Faryal Razzaq DR - Faryal@szabist-Isb - Edu.pk: Advance Research Methods Lecture 5IAmAbdullahNo ratings yet
- SPTH1202 Seminar 4 - Rapid AppraisalDocument10 pagesSPTH1202 Seminar 4 - Rapid AppraisalTuong KhueNo ratings yet
- Lecture 5Document32 pagesLecture 5Emeraldo Sabit Jr.No ratings yet
- Principles of Epidemiology: A Self-Teaching GuideFrom EverandPrinciples of Epidemiology: A Self-Teaching GuideRating: 5 out of 5 stars5/5 (2)
- Psych Osce Reviewer 1Document10 pagesPsych Osce Reviewer 1pasambalyrradjohndarNo ratings yet
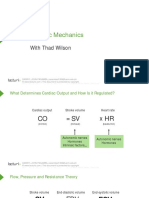
- Cardiac Mechanics: With Thad WilsonDocument26 pagesCardiac Mechanics: With Thad WilsonpasambalyrradjohndarNo ratings yet
- (PHA) 2.01 Anti-Muscarinics-Dr - ReyesDocument8 pages(PHA) 2.01 Anti-Muscarinics-Dr - ReyespasambalyrradjohndarNo ratings yet
- (EPI) 2nd LE Cup Noodles 2021C PDFDocument5 pages(EPI) 2nd LE Cup Noodles 2021C PDFpasambalyrradjohndarNo ratings yet
- Gastric CancerDocument15 pagesGastric Cancerisaco1531012No ratings yet
- (PHA) 2.12 Anti-Fungal Agents - Dr. Cabreros PDFDocument7 pages(PHA) 2.12 Anti-Fungal Agents - Dr. Cabreros PDFpasambalyrradjohndarNo ratings yet
- (PHA) 2.13 Immunopharmacology - Dr. Marbella PDFDocument10 pages(PHA) 2.13 Immunopharmacology - Dr. Marbella PDFpasambalyrradjohndarNo ratings yet
- OSCE Must Knows For All SubjectsDocument8 pagesOSCE Must Knows For All SubjectsPrincess Jeanne Roque GairanodNo ratings yet
- UERM Academic RecordsDocument1 pageUERM Academic RecordspasambalyrradjohndarNo ratings yet
- Cardiology An Introduction: 12 Cardiomyopathy With Joseph S. Alpert, M.DDocument36 pagesCardiology An Introduction: 12 Cardiomyopathy With Joseph S. Alpert, M.DpasambalyrradjohndarNo ratings yet
- (PHA) 2.10c Anti-Hansens Agents - Dr. Macaraig PDFDocument3 pages(PHA) 2.10c Anti-Hansens Agents - Dr. Macaraig PDFpasambalyrradjohndarNo ratings yet
- EBM and CAT - General Instructions For 2019-2020Document2 pagesEBM and CAT - General Instructions For 2019-2020pasambalyrradjohndarNo ratings yet
- (PHA) 4.01 Respiratory Antimicrobials - Dr. de La Cruz v3Document16 pages(PHA) 4.01 Respiratory Antimicrobials - Dr. de La Cruz v3pasambalyrradjohndarNo ratings yet
- (PHA) 2.11 Anti-Viral Drugs - Dr. Cacayorin PDFDocument15 pages(PHA) 2.11 Anti-Viral Drugs - Dr. Cacayorin PDFpasambalyrradjohndar0% (1)
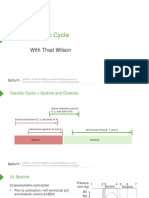
- Cardiac Cycle: With Thad WilsonDocument25 pagesCardiac Cycle: With Thad WilsonpasambalyrradjohndarNo ratings yet
- Loop Diuretics: Producers of The Greatest Diuresis With Rhonda LawesDocument23 pagesLoop Diuretics: Producers of The Greatest Diuresis With Rhonda LawespasambalyrradjohndarNo ratings yet
- OSCE Must Knows For All SubjectsDocument8 pagesOSCE Must Knows For All SubjectsPrincess Jeanne Roque GairanodNo ratings yet
- Monthly Blood Glucose Diary PDFDocument1 pageMonthly Blood Glucose Diary PDFpasambalyrradjohndarNo ratings yet
- Psych Osce Reviewer 1Document10 pagesPsych Osce Reviewer 1pasambalyrradjohndarNo ratings yet
- Psych Osce Reviewer 1Document10 pagesPsych Osce Reviewer 1pasambalyrradjohndarNo ratings yet
- Cpm15th Dengue Fever (Doh)Document18 pagesCpm15th Dengue Fever (Doh)Jeanne Marie ValesNo ratings yet
- (CLINPATH) 2.02 Transfusion II - Dr.-VillamayorDocument7 pages(CLINPATH) 2.02 Transfusion II - Dr.-VillamayorpasambalyrradjohndarNo ratings yet
- Working With Children With Cleft Lip and PalateDocument27 pagesWorking With Children With Cleft Lip and PalateMarcus Skookumchuck VanniniNo ratings yet
- Recording The Medical HistoryDocument8 pagesRecording The Medical HistorypasambalyrradjohndarNo ratings yet
- Cis 2018 PDFDocument3 pagesCis 2018 PDFTara Oliveros Dela CruzNo ratings yet
- Cis 2018Document1 pageCis 2018pasambalyrradjohndarNo ratings yet
- (MICRO) 2.03 Acid Fast StainingDocument2 pages(MICRO) 2.03 Acid Fast Stainingpasambalyrradjohndar0% (1)
- A Cross-Sectional Study On The Association Between Screen Time Exposure and Concentration Among Undergraduate University Students of UermmmciDocument3 pagesA Cross-Sectional Study On The Association Between Screen Time Exposure and Concentration Among Undergraduate University Students of UermmmcipasambalyrradjohndarNo ratings yet
- Plant Disease ResistanceDocument35 pagesPlant Disease ResistanceAnuraj DaheriyaNo ratings yet
- Toxins: Use of Botulinum Toxin in Orofacial Clinical PracticeDocument16 pagesToxins: Use of Botulinum Toxin in Orofacial Clinical PracticeAfiliado LendárioNo ratings yet
- Management of The Urologic Sepsis SyndromeDocument10 pagesManagement of The Urologic Sepsis SyndromeNur Syamsiah MNo ratings yet
- OB Case Presentation Inforgraphic Garcia-GumbeDocument2 pagesOB Case Presentation Inforgraphic Garcia-GumbeLara GeeNo ratings yet
- Comparative Study of Hepatoprotective Activity of Proprietary Polyherbal Preparations Against paraDocument5 pagesComparative Study of Hepatoprotective Activity of Proprietary Polyherbal Preparations Against paraassemNo ratings yet
- CL (Mr. Von) Mathematics (Mr. Ryan) : Trivia QuestionsDocument2 pagesCL (Mr. Von) Mathematics (Mr. Ryan) : Trivia QuestionsRichard Andrew Abratique DandanNo ratings yet
- Glossary of EMTDocument5 pagesGlossary of EMTErnan BaldomeroNo ratings yet
- Organ Systems ComparisonDocument12 pagesOrgan Systems ComparisonJeffrey YumangNo ratings yet
- Clsi 2012Document50 pagesClsi 2012niluh suwasanti100% (1)
- Chapter 33 Prescott Innate Immunity PDFDocument7 pagesChapter 33 Prescott Innate Immunity PDFneeru.bhagatNo ratings yet
- Fetal Blood Sampling: 1. PurposeDocument7 pagesFetal Blood Sampling: 1. PurposeMuathNo ratings yet
- (Lecture) Approach To AscitesDocument48 pages(Lecture) Approach To AscitesJirayu Puthhai100% (1)
- Nutrients: Anemia of Chronic Diseases: Wider Diagnostics-Better Treatment?Document17 pagesNutrients: Anemia of Chronic Diseases: Wider Diagnostics-Better Treatment?Gufront MustofaNo ratings yet
- Blood LossDocument23 pagesBlood LossSatriya DharmaNo ratings yet
- Yes, it hurts here.Roxana: I'm going to give you an injection to numb the area. Now I'm going to check the tooth with the probe again. Does it still hurtDocument5 pagesYes, it hurts here.Roxana: I'm going to give you an injection to numb the area. Now I'm going to check the tooth with the probe again. Does it still hurtCristian IugaNo ratings yet
- NCMB316 Rle 2-10-7addison's DiseaseDocument4 pagesNCMB316 Rle 2-10-7addison's DiseaseMaica LectanaNo ratings yet
- Abdominoperineal Resection MilesDocument17 pagesAbdominoperineal Resection MilesHugoNo ratings yet
- Reading Task 1-Breast Cancer and The ElderlyDocument6 pagesReading Task 1-Breast Cancer and The ElderlyJats_Fru_1741100% (5)
- Biology 1610 E-Portfolio Assignment PDFDocument4 pagesBiology 1610 E-Portfolio Assignment PDFapi-437601454No ratings yet
- Emergency Medical Technician CPGs PDFDocument121 pagesEmergency Medical Technician CPGs PDFAnonymous OdW7ev100% (1)
- Tara's Intro To Critical CareDocument6 pagesTara's Intro To Critical CareTara McNeillNo ratings yet
- Developing Biocompatibility For Medical DevicesDocument30 pagesDeveloping Biocompatibility For Medical DevicesNagula Naresh100% (1)
- ThesisDocument5 pagesThesisVictoria ManeboNo ratings yet
- USMLE Images For The BoardsDocument297 pagesUSMLE Images For The BoardsMulham Etki100% (3)
- Name_Naw Aung_La Mai Patient Focused ProceduresDocument2 pagesName_Naw Aung_La Mai Patient Focused ProceduresEileenNo ratings yet
- Peyronies DiseaseDocument6 pagesPeyronies Diseaseapi-255601700No ratings yet
- Efects of Inspiratory Muscle Training in Older AdultsDocument10 pagesEfects of Inspiratory Muscle Training in Older AdultsMaría Camila Zuluaga AriasNo ratings yet