You might also like
- Khazanah Announces 12-Point MAS Recovery PlanDocument5 pagesKhazanah Announces 12-Point MAS Recovery Planiskandar027No ratings yet
- Singapore Dental Claim Form Interactive M003 60E 010115Document5 pagesSingapore Dental Claim Form Interactive M003 60E 010115Nazim SalehNo ratings yet
- SFA+SmartMedi+2 0+principalDocument34 pagesSFA+SmartMedi+2 0+principalNazim SalehNo ratings yet
- PHM MediSavers 2015 BrochureDocument4 pagesPHM MediSavers 2015 BrochureNazim SalehNo ratings yet
- Ikhlas Value Term TakafulDocument5 pagesIkhlas Value Term TakafulNazim SalehNo ratings yet
- SFA SmartMedi 2.0 (15-03-2016)Document71 pagesSFA SmartMedi 2.0 (15-03-2016)Nazim SalehNo ratings yet
- MediLife LeafletDocument2 pagesMediLife LeafletNazim SalehNo ratings yet
- Archipelago Pre Authorisation FormDocument3 pagesArchipelago Pre Authorisation FormNazim SalehNo ratings yet
- MediSafe Infinite PDFDocument21 pagesMediSafe Infinite PDFNazim SalehNo ratings yet
- PHM Medisavers 2015 Insurance Policy SampleDocument24 pagesPHM Medisavers 2015 Insurance Policy SampleNazim Saleh100% (1)
- SmartMedi 2.0 Leaflet - PDF - A4Document4 pagesSmartMedi 2.0 Leaflet - PDF - A4Nazim SalehNo ratings yet
- Sok7355734 A 4 PDFDocument6 pagesSok7355734 A 4 PDFNazim SalehNo ratings yet
- SmartMedi EPP/FULL Payment Form PDFDocument4 pagesSmartMedi EPP/FULL Payment Form PDFNazim SalehNo ratings yet
- SmartMedi 2.0 Leaflet - PDF - A3Document2 pagesSmartMedi 2.0 Leaflet - PDF - A3Nazim SalehNo ratings yet
- PHM MediSavers 2015 BrochureDocument4 pagesPHM MediSavers 2015 BrochureNazim SalehNo ratings yet
- Magnus Life BrochureDocument8 pagesMagnus Life BrochureNazim SalehNo ratings yet
- Flow Serve AccordRG-SeriesBrochureDocument8 pagesFlow Serve AccordRG-SeriesBrochureNazim SalehNo ratings yet
- PRJM6004 Project Procurement Management Trimester 2 2017 Miri Sarawak Campus INTDocument7 pagesPRJM6004 Project Procurement Management Trimester 2 2017 Miri Sarawak Campus INTNazim SalehNo ratings yet
- Bettis NG SeriesDocument2 pagesBettis NG SeriesNazim SalehNo ratings yet
- 10 OXLER VW Scotch Yoke Actuator 2Document2 pages10 OXLER VW Scotch Yoke Actuator 2DachyiNo ratings yet
- Ikhlas Preferred Term TakafulDocument5 pagesIkhlas Preferred Term TakafulNazim SalehNo ratings yet
- Tyco Mormc 0133 UsDocument2 pagesTyco Mormc 0133 UsNazim SalehNo ratings yet
- ESD DiscussionDocument4 pagesESD DiscussionNazim SalehNo ratings yet
- Rotork ESD CapabilitiesDocument12 pagesRotork ESD CapabilitiesNazim SalehNo ratings yet
- Bettis EHO ESD ActuatorDocument12 pagesBettis EHO ESD ActuatorNazim SalehNo ratings yet
- Air Torque Scotch Yoke at-HD SeriesDocument8 pagesAir Torque Scotch Yoke at-HD SeriesNazim SalehNo ratings yet
- Module 6Document17 pagesModule 6Nazim SalehNo ratings yet
- Module 4Document11 pagesModule 4Nazim SalehNo ratings yet
- Module 5Document13 pagesModule 5Nazim SalehNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Religious Marriage in A Liberal State Gidi Sapir & Daniel StatmanDocument26 pagesReligious Marriage in A Liberal State Gidi Sapir & Daniel StatmanR Hayim BakaNo ratings yet
- 11 Days Banner Advertising Plan for Prothom AloDocument4 pages11 Days Banner Advertising Plan for Prothom AloC. M. Omar FaruqNo ratings yet
- Rubric for Evaluating Doodle NotesDocument1 pageRubric for Evaluating Doodle NotesMa. Socorro HilarioNo ratings yet
- Science Club-6Document2 pagesScience Club-6Nguyễn Huyền Trang100% (1)
- Fil 01 Modyul 7Document30 pagesFil 01 Modyul 7Jamie ann duquezNo ratings yet
- Clia & Cap Regulatory TrainingDocument23 pagesClia & Cap Regulatory TrainingWilliam David HommelNo ratings yet
- Sunrise Conveyors Maintenance OfferDocument3 pagesSunrise Conveyors Maintenance OfferRampwalker ConveyorNo ratings yet
- Online Applicaiton Regulations Under CQ (MBBS&BDS) ChangedDocument23 pagesOnline Applicaiton Regulations Under CQ (MBBS&BDS) Changedyamini susmitha PNo ratings yet
- Mobile Pixels v. Schedule A - Complaint (D. Mass.)Document156 pagesMobile Pixels v. Schedule A - Complaint (D. Mass.)Sarah BursteinNo ratings yet
- Surface Chemistry Literature List: Literature On The SubjectDocument5 pagesSurface Chemistry Literature List: Literature On The SubjectMasih SuryanaNo ratings yet
- A Post-Neoliberal Ecopolitics (Philosophy Today) by Thomas NailDocument12 pagesA Post-Neoliberal Ecopolitics (Philosophy Today) by Thomas NailEugeneLangNo ratings yet
- IEC 60050-151-2001 Amd2-2014Document8 pagesIEC 60050-151-2001 Amd2-2014mameri malekNo ratings yet
- Chapter 16 Study GuideDocument2 pagesChapter 16 Study GuideChang Ho LeeNo ratings yet
- Working While Studying in Higher Education: The Impact of The Economic Crisis On Academic and Labour Market Success (Preprint Version)Document22 pagesWorking While Studying in Higher Education: The Impact of The Economic Crisis On Academic and Labour Market Success (Preprint Version)Vexie Monique GabolNo ratings yet
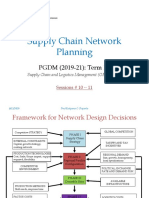
- Network Design Decisions FrameworkDocument26 pagesNetwork Design Decisions Frameworkaditya nemaNo ratings yet
- Fe en Accion - Morris VendenDocument734 pagesFe en Accion - Morris VendenNicolas BertoaNo ratings yet
- TallerDocument102 pagesTallerMarie RodriguezNo ratings yet
- Effecting Organizational Change PresentationDocument23 pagesEffecting Organizational Change PresentationSvitlanaNo ratings yet
- Applied Crypto HardeningDocument111 pagesApplied Crypto Hardeningadr99No ratings yet
- Solar Power Is The Last Energy Resource That Isn't Owned Yet - Nobody Taxes The Sun Yet.Document5 pagesSolar Power Is The Last Energy Resource That Isn't Owned Yet - Nobody Taxes The Sun Yet.Norhanifa HADJI AMERNo ratings yet
- Week 1 and 2 Literature LessonsDocument8 pagesWeek 1 and 2 Literature LessonsSalve Maria CardenasNo ratings yet
- Vivarium - Vol 37, Nos. 1-2, 1999Document306 pagesVivarium - Vol 37, Nos. 1-2, 1999Manticora VenerabilisNo ratings yet
- Day 16. The 10th ScoringDocument8 pagesDay 16. The 10th ScoringWahyu SaputraNo ratings yet
- Cover Letter For Post of Business Process Improvement CoordinatorDocument3 pagesCover Letter For Post of Business Process Improvement Coordinatorsandeep salgadoNo ratings yet
- Words and Lexemes PDFDocument48 pagesWords and Lexemes PDFChishmish DollNo ratings yet
- Dorfman v. UCSD Ruling - California Court of Appeal, Fourth Appellate DivisionDocument20 pagesDorfman v. UCSD Ruling - California Court of Appeal, Fourth Appellate DivisionThe College FixNo ratings yet
- Comillas Elementary Class Program Modular Distance LearningDocument24 pagesComillas Elementary Class Program Modular Distance Learningbaldo yellow4No ratings yet
- Pride & Prejudice film sceneDocument72 pagesPride & Prejudice film sceneha eunNo ratings yet
- History of Cisco and IBMDocument1 pageHistory of Cisco and IBMSven SpenceNo ratings yet