You might also like
- Road Deterioration in Developing CountriesDocument74 pagesRoad Deterioration in Developing CountriesBepdjNo ratings yet
- Undp Sle EnergyprofileDocument100 pagesUndp Sle EnergyprofileBepdjNo ratings yet
- Draft Songo Moyamba Road ConceptDocument16 pagesDraft Songo Moyamba Road ConceptBepdjNo ratings yet
- CRK 2-130-13 A-W-A-AuuvDocument5 pagesCRK 2-130-13 A-W-A-AuuvBepdjNo ratings yet
- Evaluation of The Geothermal Energy Potential For South AfricaDocument8 pagesEvaluation of The Geothermal Energy Potential For South AfricaBepdjNo ratings yet
- NJH Group Profile TradingDocument30 pagesNJH Group Profile TradingBepdjNo ratings yet
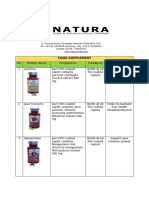
- Natura Supplement & Finished ListDocument6 pagesNatura Supplement & Finished ListBepdjNo ratings yet
- PT. Citilink Indonesia NPWP: 02.827.597.2-093.000 Jl. Raya Juanda Sawotratap Gedangan SidoarjoDocument3 pagesPT. Citilink Indonesia NPWP: 02.827.597.2-093.000 Jl. Raya Juanda Sawotratap Gedangan SidoarjoBepdjNo ratings yet
- Specification - DC FineDocument1 pageSpecification - DC FineBepdjNo ratings yet
- Specs Des Full Fat FineDocument1 pageSpecs Des Full Fat FineBepdjNo ratings yet
- Ascend Trading BrochureDocument8 pagesAscend Trading BrochureBepdjNo ratings yet
- CIBODocument16 pagesCIBOBepdjNo ratings yet
- The International Student's Guide To de La Salle University: Produced in 2016 by The Office For Strategic CommunicationsDocument22 pagesThe International Student's Guide To de La Salle University: Produced in 2016 by The Office For Strategic CommunicationsBepdjNo ratings yet
- Office of Admissions and ScholarshipsDocument7 pagesOffice of Admissions and ScholarshipsBepdjNo ratings yet
- Checklist For Visa Application Tourism and Visit To Family / FriendsDocument4 pagesChecklist For Visa Application Tourism and Visit To Family / FriendsBepdjNo ratings yet
- Syrup Liquid: Therapeutic Class Brand Name Composition Dosage Form PackDocument3 pagesSyrup Liquid: Therapeutic Class Brand Name Composition Dosage Form PackBepdjNo ratings yet
- Capsules: Therapeutic Class Brand Name Composition Dosage Form PackDocument3 pagesCapsules: Therapeutic Class Brand Name Composition Dosage Form PackBepdjNo ratings yet
- Ampoules: Therapeutic Class Brand Name Composition Dosage Form PackDocument3 pagesAmpoules: Therapeutic Class Brand Name Composition Dosage Form PackBepdjNo ratings yet
- Split Hopper Barge 1000 M: DimensionsDocument2 pagesSplit Hopper Barge 1000 M: DimensionsBepdj100% (1)
- Vials / Liquid: Therapeutic Class Brand Name Composition Dosage Form PackDocument1 pageVials / Liquid: Therapeutic Class Brand Name Composition Dosage Form PackBepdjNo ratings yet
- Gazette 2015 Mabel 2 CurrentDocument100 pagesGazette 2015 Mabel 2 CurrentBepdjNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Drug - WikipediaDocument4 pagesDrug - WikipedianightmareNo ratings yet
- Acute Asthma Paed WaniDocument16 pagesAcute Asthma Paed WaniNurul Syazwani RamliNo ratings yet
- Chapter Three: 3 .Materials and MethodsDocument33 pagesChapter Three: 3 .Materials and MethodsGobena AdebaNo ratings yet
- First Semester QuizDocument14 pagesFirst Semester Quiz11521166No ratings yet
- The Conditions of The Small-Scale Miners in Barangay Bukal, Nabunturan Compostela Valley ProvinceDocument24 pagesThe Conditions of The Small-Scale Miners in Barangay Bukal, Nabunturan Compostela Valley Provincexenos19No ratings yet
- Medical Language 3rd Edition Test Bank Susan M TurleyDocument37 pagesMedical Language 3rd Edition Test Bank Susan M Turleykatieterryrlrb100% (12)
- Final RM Mini ProjectDocument33 pagesFinal RM Mini ProjectRahul ChaudharyNo ratings yet
- Mental Health & Psychiatric NursingDocument617 pagesMental Health & Psychiatric NursingEVERYTHING TvNo ratings yet
- Nursing Process of PneumoniaDocument5 pagesNursing Process of Pneumoniatin2x061275% (8)
- EpidemiologiDocument7 pagesEpidemiologiazzaNo ratings yet
- Chapter 17 Unit IDocument23 pagesChapter 17 Unit IGlory MimiNo ratings yet
- Hemophilia and Its Treatment: Brief ReviewDocument7 pagesHemophilia and Its Treatment: Brief ReviewSalsa BillaNo ratings yet
- 978-615-5169-15-1 Physiology Anatomy PDFDocument236 pages978-615-5169-15-1 Physiology Anatomy PDFSuresh Kanna0% (1)
- SP 32434 Warm Up and Cool Down - Indd PDFDocument1 pageSP 32434 Warm Up and Cool Down - Indd PDFMylene EntionNo ratings yet
- DiphtheriaDocument10 pagesDiphtheriaAgustin IskandarNo ratings yet
- Does WiFi Affect The BrainDocument6 pagesDoes WiFi Affect The BrainrustyNo ratings yet
- Sensititre Plate Guide Booklet EN PDFDocument62 pagesSensititre Plate Guide Booklet EN PDFXuân Tài NguyễnNo ratings yet
- Pyle Et Al 1995 - Rapid Direct Count E ColiDocument7 pagesPyle Et Al 1995 - Rapid Direct Count E ColiFabio SenaNo ratings yet
- 5 Benign Febrile Convulsions Nursing Care PlansDocument19 pages5 Benign Febrile Convulsions Nursing Care Plansaaron tabernaNo ratings yet
- Proteinuria A Guide To Diagnosis and AssDocument7 pagesProteinuria A Guide To Diagnosis and AssMarcelliaNo ratings yet
- Transposons Mediated MutagenesisDocument41 pagesTransposons Mediated Mutagenesissaurabh784No ratings yet
- Antiemetic Drugs PDFDocument12 pagesAntiemetic Drugs PDFDanisha Laila100% (2)
- Bulk Forming PurgativesDocument12 pagesBulk Forming PurgativesabcdNo ratings yet
- Pressure Sore: GradingDocument2 pagesPressure Sore: GradingAnusha VergheseNo ratings yet
- Ancient Cures, Charms, and Usages of IrelandDocument282 pagesAncient Cures, Charms, and Usages of IrelandIan ThomsonNo ratings yet
- Nutrition in Neurosurgery 2Document13 pagesNutrition in Neurosurgery 2Mimakos CyberNo ratings yet
- Report 1 - History of Medical TechnologyDocument1 pageReport 1 - History of Medical TechnologyMaxine TaeyeonNo ratings yet
- AIIMS 2015 Solved PaperDocument436 pagesAIIMS 2015 Solved PaperSurya TejaNo ratings yet
- B.inggris Report TextDocument3 pagesB.inggris Report TextSeryx DoankNo ratings yet
- RCDSO Guidelines Implant Dentistry PDFDocument16 pagesRCDSO Guidelines Implant Dentistry PDFl4j0b9No ratings yet