You might also like
- Nnewfile 2Document2 pagesNnewfile 2mahariyaNo ratings yet
- A Look at Bipolar Disorder in Michael ClaytonDocument9 pagesA Look at Bipolar Disorder in Michael ClaytonRichard Moore0% (1)
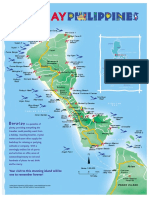
- Boracay Brochure PDFDocument2 pagesBoracay Brochure PDFmolesag100% (1)
- Rheumatoid Arthritis Diagnosis and ManagementDocument53 pagesRheumatoid Arthritis Diagnosis and ManagementamereNo ratings yet
- Understanding Toxic Goiter and Its Nursing CareDocument22 pagesUnderstanding Toxic Goiter and Its Nursing CareJohn Matley Caampued100% (2)
- Capillary Blood Glucose Monitoring or CBG MonitoringDocument5 pagesCapillary Blood Glucose Monitoring or CBG MonitoringRonilyn Mae Alvarez100% (1)
- Major Rail Routes in IndonesiaDocument1 pageMajor Rail Routes in Indonesianna_husnaNo ratings yet
- Green Knowledge ActivityDocument12 pagesGreen Knowledge ActivityAgung Nugroho ZainiNo ratings yet
- Chapter 2: Context of The StudyDocument14 pagesChapter 2: Context of The StudyMounir Mc MounirNo ratings yet
- Chapter 2: Context of The StudyDocument14 pagesChapter 2: Context of The StudyMounir Mc MounirNo ratings yet
- The State of Children in Indonesia 2020Document78 pagesThe State of Children in Indonesia 2020firda FibrilaNo ratings yet
- Trans Sumatera RailwayDocument1 pageTrans Sumatera Railwayesun faizNo ratings yet
- Bahan Capaian Ispa KalbarDocument8 pagesBahan Capaian Ispa KalbarEva NurZalinaNo ratings yet
- Important Class NotesDocument7 pagesImportant Class NotesJatinNo ratings yet
- Bagus Agro Pelaga PresentationDocument20 pagesBagus Agro Pelaga Presentationivon carolineNo ratings yet
- General - Indonesia IndonesiaDocument72 pagesGeneral - Indonesia Indonesiawaleed yehia100% (1)
- OCHA-PHL-MARAWI4 Brgy MapDocument1 pageOCHA-PHL-MARAWI4 Brgy MapDisoma RashidahNo ratings yet
- APRON MANAGEMENT FOCUS GROUPDocument33 pagesAPRON MANAGEMENT FOCUS GROUPajeng putriNo ratings yet
- FY20FactBookJuly 2021 VFDocument38 pagesFY20FactBookJuly 2021 VFPrateek PandeyNo ratings yet
- Carte 2018-19Document1 pageCarte 2018-19XimeNo ratings yet
- GGGGG: LegendDocument1 pageGGGGG: LegendAkhmad Hata EfendiNo ratings yet
- Indonesia: Map ofDocument5 pagesIndonesia: Map ofLung KinNo ratings yet
- Indonesia: Map ofDocument5 pagesIndonesia: Map ofnasar adenNo ratings yet
- HTLS DDW ACEF 2015 16 June 2015Document19 pagesHTLS DDW ACEF 2015 16 June 2015Sube OhNo ratings yet
- Perak PMR 2016 PDFDocument118 pagesPerak PMR 2016 PDFNURAIN HANIS BINTI ARIFFNo ratings yet
- An Economic Research Project On ASEAN Nations: Brunei DarussalamDocument30 pagesAn Economic Research Project On ASEAN Nations: Brunei DarussalamGerard JuntillaNo ratings yet
- Rfi Workshop Presentation PDFDocument47 pagesRfi Workshop Presentation PDFFatan WikramaNo ratings yet
- Draf Report SDocument1 pageDraf Report SfahmiieNo ratings yet
- Map of Indonesia in 40 charactersDocument5 pagesMap of Indonesia in 40 charactersAlan FassetNo ratings yet
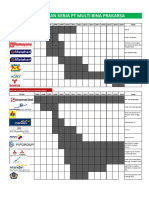
- Pengalam Kerja PT Multi Bina PrakarsaDocument5 pagesPengalam Kerja PT Multi Bina PrakarsaYanuar DwiputrantoNo ratings yet
- Bird Watching in MalaysiaDocument44 pagesBird Watching in MalaysiaEvert De Wolf100% (1)
- B2B Proposal DeckDocument23 pagesB2B Proposal Deckdhika asahimasNo ratings yet
- Beads in Lembah BujangDocument12 pagesBeads in Lembah BujangManjeetNo ratings yet
- C - 1054 - Aang Dwi Atma Nugraha PDFDocument3 pagesC - 1054 - Aang Dwi Atma Nugraha PDFDens AndrianNo ratings yet
- Pemodelan Sistem Panas Bumi - Ailimaxpem AkamigasDocument9 pagesPemodelan Sistem Panas Bumi - Ailimaxpem AkamigascitraNo ratings yet
- Bali Toll Road Innovation Case StudyDocument40 pagesBali Toll Road Innovation Case StudyBagus Sukma Putra100% (1)
- Challenges and Future of Indonesian PortsDocument47 pagesChallenges and Future of Indonesian PortsHerdy Pratama PutraNo ratings yet
- RSPO-certified Padang Halaban MillDocument2 pagesRSPO-certified Padang Halaban MillTai AnjingNo ratings yet
- Corporate Presentation INVESTORDocument15 pagesCorporate Presentation INVESTORHenry So E DiarkoNo ratings yet
- Bab 0 IndexDocument14 pagesBab 0 IndexChing Fu ChooiNo ratings yet
- Malaysia Islands & Beaches 2019-CompressedDocument40 pagesMalaysia Islands & Beaches 2019-CompressedMaria VidalNo ratings yet
- Delivery Service For IKEA Tebrau: Zones Delivery Locations FeesDocument1 pageDelivery Service For IKEA Tebrau: Zones Delivery Locations FeesNurul Nadiah Binti ZulkipliNo ratings yet
- Indonesian Container Port NetworkDocument3 pagesIndonesian Container Port NetworkTania Edna Bhakty SoetjiptoNo ratings yet
- Hostel Checklist: Brand New!Document11 pagesHostel Checklist: Brand New!Nikhil JainNo ratings yet
- ISP FiberstarDocument11 pagesISP FiberstarAhmad AfandiNo ratings yet
- EVCuzz Customer Gathering PresentationDocument25 pagesEVCuzz Customer Gathering PresentationMuhamad DimasyqiNo ratings yet
- A Profile of Central VisayasDocument6 pagesA Profile of Central VisayasiamfrancoiseNo ratings yet
- Lahan PadiDocument23 pagesLahan PadiSimon32 TooNo ratings yet
- 2nd Anti-Piracy Patrol in The Gulf of GuineaDocument3 pages2nd Anti-Piracy Patrol in The Gulf of GuineaWhite TigerNo ratings yet
- Master plan for developing Tanjung Lesung coastal areaDocument2 pagesMaster plan for developing Tanjung Lesung coastal areaCynthia HerisnayanNo ratings yet
- The Government of Central Java Province Health OfficeDocument50 pagesThe Government of Central Java Province Health OfficeSarma Verawaty SilalahiNo ratings yet
- The Government of Central Java Province Health OfficeDocument50 pagesThe Government of Central Java Province Health OfficeRia Septiyani CloudsYesungNo ratings yet
- The Government of Central Java Province Health OfficeDocument50 pagesThe Government of Central Java Province Health OfficeAbu AzaimarNo ratings yet
- FINAL REPORT - Tanjung Pandan Master Plan+LA - HRDocument177 pagesFINAL REPORT - Tanjung Pandan Master Plan+LA - HRTomy Hastomo ArdhiNo ratings yet
- CorridorAcquisition InformationforInvestor VFDocument12 pagesCorridorAcquisition InformationforInvestor VFAdi HamdanNo ratings yet
- MA004 StormPath 300dpi PDFDocument1 pageMA004 StormPath 300dpi PDFPia QuillopeNo ratings yet
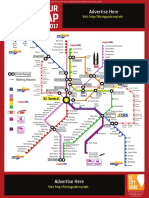
- Kuala Lumpur Train Map July 2017Document1 pageKuala Lumpur Train Map July 2017Mustafidzul MustaphaNo ratings yet
- Psau Scicat RoadmapDocument1 pagePsau Scicat RoadmapPSAU ICTRDNo ratings yet
- ENG DivingDocument20 pagesENG DivingWIRATNA WIRATNANo ratings yet
- Sarawak TourismEventCalendar 2022Document2 pagesSarawak TourismEventCalendar 2022Izzah Nazatul Nazihah Binti EjapNo ratings yet
- Map Sanur 2022Document1 pageMap Sanur 2022hpr eventsNo ratings yet
- SSP Presentation Rev1Document19 pagesSSP Presentation Rev1Le BreuNo ratings yet
- Lap. Curah Hujan 2012Document44 pagesLap. Curah Hujan 2012Rizki SaefulNo ratings yet
- English Assignment Group 7Document11 pagesEnglish Assignment Group 7Agus JunaidiNo ratings yet
- Bahan Aplikasi TADocument20 pagesBahan Aplikasi TAAgus JunaidiNo ratings yet
- Jumlah Penjaringan Kesehatan Telinga Sekolah Dasar Tahun 2016 Puskesmas Se-Kelurahan Tanjung PriokDocument11 pagesJumlah Penjaringan Kesehatan Telinga Sekolah Dasar Tahun 2016 Puskesmas Se-Kelurahan Tanjung PriokAgus JunaidiNo ratings yet
- English Assignment: Group 7Document11 pagesEnglish Assignment: Group 7Agus JunaidiNo ratings yet
- Daftar Bahan Lab 2014 (Adendum)Document2 pagesDaftar Bahan Lab 2014 (Adendum)Agus JunaidiNo ratings yet
- History of shingles rehabilitationDocument1 pageHistory of shingles rehabilitationTrixter GarciaNo ratings yet
- MH Guideline For Web v2Document1 pageMH Guideline For Web v2FilbertaNo ratings yet
- Integumentary SystemDocument22 pagesIntegumentary SystemEunice Angela FulguerasNo ratings yet
- MedVantage - Fellowship Program in Diabetes MillitusDocument2 pagesMedVantage - Fellowship Program in Diabetes MillitusmedvantageNo ratings yet
- Bilateral Variation in The Branching Pattern of The Axillary Artery - A Case ReportDocument5 pagesBilateral Variation in The Branching Pattern of The Axillary Artery - A Case ReportIJAR JOURNALNo ratings yet
- Cga - 1Document19 pagesCga - 1Kenji Tolero100% (1)
- Frequency of Hyponatraemia and Hypokalaemia in Malnourished Children With Acute DiarrhoeaDocument4 pagesFrequency of Hyponatraemia and Hypokalaemia in Malnourished Children With Acute DiarrhoeaRaja Bajak LautNo ratings yet
- DKD and Sglt2iDocument61 pagesDKD and Sglt2iماكريلا المصريNo ratings yet
- Artículo 7000 PalabrasDocument8 pagesArtículo 7000 PalabrasEmalaith BlackburnNo ratings yet
- Personality DisordersDocument43 pagesPersonality DisordersJeanette Klaber100% (2)
- Gestational Trophoblastic Disease Causes, Symptoms and TreatmentDocument10 pagesGestational Trophoblastic Disease Causes, Symptoms and TreatmentAnggie Pradetya MaharaniNo ratings yet
- KP 1 Dasar-Dasar Kedokteran Gaya Hidup - Prof. Dr. Dr. Gusbakti SP - KKLPDocument19 pagesKP 1 Dasar-Dasar Kedokteran Gaya Hidup - Prof. Dr. Dr. Gusbakti SP - KKLPacalNo ratings yet
- HPNDocument32 pagesHPNkaren GoNo ratings yet
- Balance and Fall Prevention: By, Sankari Nedunsaliyan Physiotherapist Dip in PT (MAL), BSC Hons Applied Rehab (UK)Document63 pagesBalance and Fall Prevention: By, Sankari Nedunsaliyan Physiotherapist Dip in PT (MAL), BSC Hons Applied Rehab (UK)Ali ImranNo ratings yet
- Common Side Effects of OtezlaDocument57 pagesCommon Side Effects of OtezlaMica JeremijevicNo ratings yet
- Cetirizine drug study summaryDocument1 pageCetirizine drug study summaryArthur Christopher Corpuz100% (1)
- Case Pre - Rhd+capDocument61 pagesCase Pre - Rhd+capAlexies Cassandra SasoyNo ratings yet
- Nursing Assessment: Gastrointestinal System (Chapter 39) : Structures and FunctionsDocument4 pagesNursing Assessment: Gastrointestinal System (Chapter 39) : Structures and FunctionsPrince K. TaileyNo ratings yet
- Chapter 31 Dyslipidemia UpdatedDocument37 pagesChapter 31 Dyslipidemia UpdatedMai TarekNo ratings yet
- Dissociation Affect Dysregulation Somatization BVDKDocument22 pagesDissociation Affect Dysregulation Somatization BVDKkanuNo ratings yet
- Illegal Drugs and Its Ill EffectsDocument83 pagesIllegal Drugs and Its Ill EffectsJAIGLO LAYNONo ratings yet
- EximiaDocument3 pagesEximiaDr skinNo ratings yet
- VO2 Max Levels Shuttle Run Test ResultsDocument10 pagesVO2 Max Levels Shuttle Run Test ResultsTri MackNo ratings yet
- Medication Therapy StudentDocument4 pagesMedication Therapy StudentНаталья МурашоваNo ratings yet
- Tumor Lysis SyndromeDocument12 pagesTumor Lysis Syndromeapi-647779956No ratings yet