You might also like
- Cosmetics Lect.09Document6 pagesCosmetics Lect.09على الجارحىNo ratings yet
- Facial Scar Revision: Suzan Obagi, MD Angela S. Casey, MDDocument8 pagesFacial Scar Revision: Suzan Obagi, MD Angela S. Casey, MDchaeraniNo ratings yet
- Dermaplaning Benefits for Younger Looking SkinDocument2 pagesDermaplaning Benefits for Younger Looking SkinDaniel CalderonNo ratings yet
- Granactive Retinoid (Grant Industries)Document19 pagesGranactive Retinoid (Grant Industries)Rizqi AmaliyahNo ratings yet
- Sun Protection in Acne, Dr. Dwi Retno Adi WinarniDocument29 pagesSun Protection in Acne, Dr. Dwi Retno Adi WinarniAdi Sutriwanto PasaribuNo ratings yet
- Dermatrix - Radiofrequency Facial Rejuvenation Evidence-Based Effect IraildesDocument12 pagesDermatrix - Radiofrequency Facial Rejuvenation Evidence-Based Effect IraildesTatiane MouraNo ratings yet
- PeelingDocument30 pagesPeelingAkiko LeeNo ratings yet
- Skin Diseases Affecting The VulvaDocument7 pagesSkin Diseases Affecting The VulvaNoraNo ratings yet
- Sothys, The Professional DifferenceDocument29 pagesSothys, The Professional DifferenceNazihCosmeticsNo ratings yet
- Chemical Peel PublishedDocument7 pagesChemical Peel PublishedkkNo ratings yet
- Aesthetic Durable Forehead Contouring in Asians With Fat Grafting and Botulinum ToxinDocument7 pagesAesthetic Durable Forehead Contouring in Asians With Fat Grafting and Botulinum ToxinAnonymous LnWIBo1GNo ratings yet
- BB Glow TreatmentDocument19 pagesBB Glow TreatmentDrAmit Gaba MdsNo ratings yet
- Acne Vulgaris (Or Acne) Is A CommonDocument21 pagesAcne Vulgaris (Or Acne) Is A CommonNia YuniarNo ratings yet
- Chemical Peels Deep, Medium, and LightDocument9 pagesChemical Peels Deep, Medium, and LightDeborah DobieszNo ratings yet
- AntiAging TherapiesDocument4 pagesAntiAging TherapiesRavvaNo ratings yet
- Chemical Peels - Principles, Peeling Agents, and Pretreatment Assessment - UpToDateDocument16 pagesChemical Peels - Principles, Peeling Agents, and Pretreatment Assessment - UpToDateMichelle Caracas Aponte100% (1)
- Acne and Niacinamide 2017 dth.12481Document7 pagesAcne and Niacinamide 2017 dth.12481Vita BūdvytėNo ratings yet
- Presentación Gama Mesohyal - en v1.1Document26 pagesPresentación Gama Mesohyal - en v1.1Niculae Bogdan DimitrieNo ratings yet
- Post Inflammatory HyperpigmentationDocument5 pagesPost Inflammatory HyperpigmentationnoviantykusumoNo ratings yet
- Cosmeceuticals - Practical ApplicationsDocument16 pagesCosmeceuticals - Practical ApplicationsTuyenHHCNo ratings yet
- AHA in Treatment of Signs of AgingDocument10 pagesAHA in Treatment of Signs of AgingChamomillaeFlosNo ratings yet
- Chemical Peels - Procedures and Complications - UpToDateDocument23 pagesChemical Peels - Procedures and Complications - UpToDateMichelle Caracas AponteNo ratings yet
- Combination of Microneedling and Glycolic Acid Peels For TheDocument7 pagesCombination of Microneedling and Glycolic Acid Peels For Thealejandrogonzalez89No ratings yet
- What Are The Benefits of Dermaplaning and How Much Does It Cost?Document2 pagesWhat Are The Benefits of Dermaplaning and How Much Does It Cost?Daniel CalderonNo ratings yet
- Hyperpigmentation Guide- Types, Tips & TreatmentsDocument10 pagesHyperpigmentation Guide- Types, Tips & TreatmentsN SubhashNo ratings yet
- Peeling and Microdermabrasion Changes HystologicalsDocument6 pagesPeeling and Microdermabrasion Changes HystologicalsBrian MacíaNo ratings yet
- Why Say No To Emulsifiers - Virtual BeautyDocument4 pagesWhy Say No To Emulsifiers - Virtual BeautyShahid YousafNo ratings yet
- FOTONA New Skin Treatment Possibilities With Piano Mode On An Nd-YAGDocument11 pagesFOTONA New Skin Treatment Possibilities With Piano Mode On An Nd-YAGLucia Regina Cavalcanti TeixeiraNo ratings yet
- M.pen Pro Brochure (ENG)Document12 pagesM.pen Pro Brochure (ENG)Nanda Apeldoorn (beautywithjoy)No ratings yet
- MELASMA: Etiology, Clinical Features, Differential Diagnoses and Treatment OptionsDocument20 pagesMELASMA: Etiology, Clinical Features, Differential Diagnoses and Treatment OptionsAndi Firman MubarakNo ratings yet
- Basic Model User'S ManualDocument4 pagesBasic Model User'S ManualDokterYolanda100% (1)
- Viral skin diseases and common wartsDocument4 pagesViral skin diseases and common wartsFatima Al MarzouqiNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument22 pagesSee Full Prescribing Information For Complete Boxed WarningTracy PopeNo ratings yet
- Philoderm Professional Peeling GuideDocument60 pagesPhiloderm Professional Peeling GuideNiculae Bogdan Dimitrie100% (1)
- Treatment Guide and ProtocolsDocument14 pagesTreatment Guide and ProtocolsViany MartinezNo ratings yet
- New Generation of Sun Care: Pat McdermottDocument39 pagesNew Generation of Sun Care: Pat McdermottCielo Dela Cruz100% (1)
- Facial Vascular Danger Zones For Filler Injections: Uwe Wollina - Alberto GoldmanDocument8 pagesFacial Vascular Danger Zones For Filler Injections: Uwe Wollina - Alberto GoldmanLuis Fernando WeffortNo ratings yet
- Dermatology BookDocument13 pagesDermatology BookYezenashNo ratings yet
- Dermaroller FaqsDocument9 pagesDermaroller Faqsjp516No ratings yet
- Ultrasound Skin Facial TreatmentDocument3 pagesUltrasound Skin Facial TreatmentRaphaela JimenesNo ratings yet
- Basic Skin Care ProtocolsDocument16 pagesBasic Skin Care ProtocolsCarmi Bolivar CodotcoNo ratings yet
- 13-TCA Directions PDFDocument2 pages13-TCA Directions PDFPurUjit BanSalNo ratings yet
- Niumee Price List 2018Document26 pagesNiumee Price List 2018Anonymous XiZx8SbQBNo ratings yet
- Jett Plasma Lift Medical Manual ENG - Akt - .9.9.15 PDFDocument27 pagesJett Plasma Lift Medical Manual ENG - Akt - .9.9.15 PDFMichaely Natali100% (1)
- Medik8 - HyperpigmentationDocument8 pagesMedik8 - HyperpigmentationMustika Dwi SusilowatiNo ratings yet
- Acne Treatment Strategies and TherapiesDocument32 pagesAcne Treatment Strategies and TherapiesdokterasadNo ratings yet
- Issues Solution Active Ingredient: Beta-Hydroxy Acid (Salicylic Acid)Document3 pagesIssues Solution Active Ingredient: Beta-Hydroxy Acid (Salicylic Acid)Jesabel Delas PenasNo ratings yet
- HIFU-Client-Pre-and-After-Care - 2Document4 pagesHIFU-Client-Pre-and-After-Care - 2Hanan AnsariNo ratings yet
- 2 Merz Institute Skin Laxity LU 2summary PDFDocument5 pages2 Merz Institute Skin Laxity LU 2summary PDFMafer ArizaNo ratings yet
- Acne ScarsDocument8 pagesAcne Scarsjp516No ratings yet
- Wholesale Dr. Stretch Marks Oil Use Microneedling Import Removal Stretch Marks New Project For Beauty Salon Effective Stretch Ma PDFDocument1 pageWholesale Dr. Stretch Marks Oil Use Microneedling Import Removal Stretch Marks New Project For Beauty Salon Effective Stretch Ma PDFGlen EstrellaNo ratings yet
- Cosmeticsandtoiletries201506 DL PDFDocument68 pagesCosmeticsandtoiletries201506 DL PDFtmlNo ratings yet
- HIFU KL02 User ManualDocument11 pagesHIFU KL02 User ManualRita Godoy100% (1)
- Calcium Hydroxylapatite Combined With Microneedling and Ascorbic Acid Is Effective For Treating Stretch MarksDocument9 pagesCalcium Hydroxylapatite Combined With Microneedling and Ascorbic Acid Is Effective For Treating Stretch Marks郭先薈No ratings yet
- Microdermabrasion Manual SFMCDocument13 pagesMicrodermabrasion Manual SFMCji76100% (1)
- Filler Course MaterialDocument106 pagesFiller Course MaterialFiras HamidehNo ratings yet
- Cidesco Case Histories BookletDocument11 pagesCidesco Case Histories Bookletmatina papaspyrouNo ratings yet
- A Simple Guide to Hyperhidrosis, (Excessive Sweating) diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hyperhidrosis, (Excessive Sweating) diagnosis, Treatment and Related ConditionsNo ratings yet
- Formasi CPNS - PESAWARAN2019 PDFDocument30 pagesFormasi CPNS - PESAWARAN2019 PDFNafiahEmaSuryaniNo ratings yet
- Colon Cancer PDFDocument88 pagesColon Cancer PDFGemma GarciaNo ratings yet
- Nausea and Vomiting: NCCN Guidelines For PatientsDocument46 pagesNausea and Vomiting: NCCN Guidelines For Patientsmuhamad anwariNo ratings yet
- Tugas Bu DaniaDocument12 pagesTugas Bu DaniaNafiahEmaSuryaniNo ratings yet
- Nafiah Ema, Nadya Amalia, Wahyu Tirta - FKKBDocument5 pagesNafiah Ema, Nadya Amalia, Wahyu Tirta - FKKBNafiahEmaSuryaniNo ratings yet
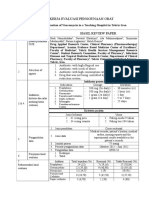
- Drug utilization evaluation of vancomycin in IranDocument2 pagesDrug utilization evaluation of vancomycin in IranNafiahEmaSuryaniNo ratings yet
- Acute Diare WHO 2005Document50 pagesAcute Diare WHO 2005Boby Abdul RahmanNo ratings yet
- Nafiah Ema, Nadya Amalia, Wahyu Tirta - FKKBDocument5 pagesNafiah Ema, Nadya Amalia, Wahyu Tirta - FKKBNafiahEmaSuryaniNo ratings yet
- Tugas Bu DaniaDocument12 pagesTugas Bu DaniaNafiahEmaSuryaniNo ratings yet
- Dextromethorphan and Codeine Objective AssessmentDocument10 pagesDextromethorphan and Codeine Objective AssessmentNafiahEmaSuryaniNo ratings yet
- Lam Gambar Fts p3Document3 pagesLam Gambar Fts p3NafiahEmaSuryaniNo ratings yet
- Topical AntibioticsDocument2 pagesTopical AntibioticsMusfirah HattaNo ratings yet
- Tugas1 Nafiah Ema Suryani - 1400023171 - VBDocument29 pagesTugas1 Nafiah Ema Suryani - 1400023171 - VBNafiahEmaSuryaniNo ratings yet
- Mucoadhesive PDFDocument9 pagesMucoadhesive PDFNafiahEmaSuryaniNo ratings yet
- Form Critical AppraisalDocument2 pagesForm Critical AppraisalNafiahEmaSuryaniNo ratings yet
- Tips Writing2013 - DyDocument31 pagesTips Writing2013 - DyNafiahEmaSuryaniNo ratings yet
- IniDocument1 pageIniNafiahEmaSuryaniNo ratings yet
- Banana Skin Acne GelDocument4 pagesBanana Skin Acne GelNafiahEmaSuryaniNo ratings yet
- Analisis Darah Ke 2Document15 pagesAnalisis Darah Ke 2NafiahEmaSuryaniNo ratings yet
- Mechanical Ventilator CareDocument9 pagesMechanical Ventilator CareAnusha Verghese100% (2)
- (Faringita Streptococica:copii: 250 MG de 2-3 Ori Pe Zi Adolescenţi Şi Adulţi: 250 MG de 4 Ori Pe Zi Sau 500 MG de 2 Ori Pe Zi Timp de 10 ZileDocument5 pages(Faringita Streptococica:copii: 250 MG de 2-3 Ori Pe Zi Adolescenţi Şi Adulţi: 250 MG de 4 Ori Pe Zi Sau 500 MG de 2 Ori Pe Zi Timp de 10 ZileAlina C100% (1)
- Pharmaceutical Contracts and NDC NumbersDocument1,752 pagesPharmaceutical Contracts and NDC NumbersSaul RuizNo ratings yet
- Chemistry Drug Metabolism Q-5Document6 pagesChemistry Drug Metabolism Q-5Drishya BioplannetNo ratings yet
- Notes in PharmacologyDocument96 pagesNotes in Pharmacologydmd_2dd50% (2)
- Beta Blockers and AsthmaDocument8 pagesBeta Blockers and AsthmaAzmachamberAzmacareNo ratings yet
- Types of AntidotesDocument1 pageTypes of AntidotesAprilVivienCuNo ratings yet
- Detailed Lesson Plan in Health 9Document6 pagesDetailed Lesson Plan in Health 9marvierose0% (1)
- Drug MetronidazoleDocument1 pageDrug MetronidazoleSrkocherNo ratings yet
- Medical Masterclass 2-Scientific Background To Medicine 2 PDFDocument136 pagesMedical Masterclass 2-Scientific Background To Medicine 2 PDFAnonymous oQtve4oNo ratings yet
- Curriculum Vitae MTDocument6 pagesCurriculum Vitae MTapi-273097827No ratings yet
- Warfarin Patient Education and Adherence StrategiesDocument5 pagesWarfarin Patient Education and Adherence StrategiesJayson TrajanoNo ratings yet
- Drug Study Silver SulfadiazineDocument1 pageDrug Study Silver SulfadiazineMaica Lectana100% (1)
- Clonazepam AJPDocument4 pagesClonazepam AJPDian GbligNo ratings yet
- RKO 2019 Dan SO 31 Nov 2018.fixDocument14 pagesRKO 2019 Dan SO 31 Nov 2018.fixjihanNo ratings yet
- Case Study on Chronic Pain and DepressionDocument5 pagesCase Study on Chronic Pain and DepressionClinton MandelaNo ratings yet
- Dietary SupplementsDocument4 pagesDietary SupplementsSORENI SORENINo ratings yet
- PLACEBO EFFECTS EXPLAINEDDocument11 pagesPLACEBO EFFECTS EXPLAINEDTaufik Ghockil ZlaluwNo ratings yet
- RanppppDocument15 pagesRanppppFarmasi MTohaNo ratings yet
- SuperDrugs! Simon's Short Drug SummaryDocument5 pagesSuperDrugs! Simon's Short Drug Summarybriancripe100% (2)
- 12 - Ocular Pharmacology - 343 - 64Document37 pages12 - Ocular Pharmacology - 343 - 64ณัฐ มีบุญNo ratings yet
- Ekstravasation AssesmentDocument2 pagesEkstravasation AssesmentHelena Christy100% (1)
- British Thoracic Society Guidelines: Initial Empirical Treatment Regimens For Community-Acquired Pneumonia (CAP) in AdultsDocument2 pagesBritish Thoracic Society Guidelines: Initial Empirical Treatment Regimens For Community-Acquired Pneumonia (CAP) in AdultslorenzorabbiNo ratings yet
- Evidence-based Injection Practice: To Aspirate or NotDocument1 pageEvidence-based Injection Practice: To Aspirate or NotElsion Goleci0% (1)
- 27 Juli 22 LKDocument144 pages27 Juli 22 LKhasib unigaNo ratings yet
- Key chemotherapy drugs and their mechanismsDocument7 pagesKey chemotherapy drugs and their mechanismsNoelani-Mei AscioNo ratings yet
- Naso Gastric Tubes QuestionsDocument5 pagesNaso Gastric Tubes QuestionsjhonNo ratings yet
- Nebu&CPTDocument32 pagesNebu&CPTAbigail Bantayan100% (1)
- Pharma Syllabus PDFDocument27 pagesPharma Syllabus PDFSheryhan Tahir BayleNo ratings yet
- Guideline On Setting Health Based Exposure Limits For Use 5 in Risk IdentificationDocument9 pagesGuideline On Setting Health Based Exposure Limits For Use 5 in Risk IdentificationhuynhhaichauchauNo ratings yet