You might also like
- Toyota 1ZZ FE 3ZZ FE Engine Repair Manual RM1099E PDFDocument141 pagesToyota 1ZZ FE 3ZZ FE Engine Repair Manual RM1099E PDFJhorwind Requena87% (15)
- Honda S2000 (00-03) Service ManualDocument0 pagesHonda S2000 (00-03) Service Manualmcustom1No ratings yet
- Why Why Analysis Presentation-TPm-training-materialDocument43 pagesWhy Why Analysis Presentation-TPm-training-materialsaravanananusha67% (6)
- Class Valedictorian SpeechDocument3 pagesClass Valedictorian Speechoracle259No ratings yet
- Project Management ProcessDocument23 pagesProject Management ProcessMuhammad Sajid Saeed100% (2)
- Outcome Assessment in Routine Clinical Practice inDocument21 pagesOutcome Assessment in Routine Clinical Practice inicuellarfloresNo ratings yet
- Caribbean Public-Private-Partnerships - PPP - Toolkit PDFDocument400 pagesCaribbean Public-Private-Partnerships - PPP - Toolkit PDFFernando Andres Beltran100% (2)
- Self PublishingDocument84 pagesSelf PublishingFrancesco CusumanoNo ratings yet
- Key Performance Indicator For HospitalDocument15 pagesKey Performance Indicator For HospitalsaphyqNo ratings yet
- Maintenance Handbook On Bonding Earthing For 25 KV AC Traction SystemsDocument46 pagesMaintenance Handbook On Bonding Earthing For 25 KV AC Traction SystemsPavan100% (1)
- Health Systems Engineering: Building A Better Healthcare Delivery SystemFrom EverandHealth Systems Engineering: Building A Better Healthcare Delivery SystemNo ratings yet
- Quality Improvement ModelsDocument64 pagesQuality Improvement ModelsShahin Patowary100% (2)
- Operations and Maintenance Manual MAN-10000946 Elmar Grease Injection Equipment AssemblyDocument56 pagesOperations and Maintenance Manual MAN-10000946 Elmar Grease Injection Equipment AssemblyAbhinav KumarNo ratings yet
- Enablers of Smart CitiesDocument30 pagesEnablers of Smart Citiesoracle259No ratings yet
- 005 PDFDocument8 pages005 PDFGrootNo ratings yet
- Copper Wire and Cable: From Wikipedia, The Free EncyclopediaDocument16 pagesCopper Wire and Cable: From Wikipedia, The Free Encyclopediatanwar_anuj1990No ratings yet
- Improving Hospital Performance and Productivity With The Balanced Scorecard - 2Document22 pagesImproving Hospital Performance and Productivity With The Balanced Scorecard - 2Yunita Soraya HusinNo ratings yet
- 1 s2.0 S003801212200012X MainDocument22 pages1 s2.0 S003801212200012X MainrahmaNo ratings yet
- UsingImplementation 032513compDocument11 pagesUsingImplementation 032513compJames LindonNo ratings yet
- Developing A Theory-Based Instrument To Assess The Impact of Continuing Professional Development Activities On Clinical Practice: A Study ProtocolDocument6 pagesDeveloping A Theory-Based Instrument To Assess The Impact of Continuing Professional Development Activities On Clinical Practice: A Study ProtocolSjktraub PahangNo ratings yet
- Case Study 3Document11 pagesCase Study 3sheilaNo ratings yet
- 2017 Article 563Document11 pages2017 Article 563raphael boechatNo ratings yet
- An Integrated Approach For Evaluating Hospital Service Quality With Linguistic PreferencesDocument16 pagesAn Integrated Approach For Evaluating Hospital Service Quality With Linguistic PreferencestiffanyNo ratings yet
- BNS Honours Nursing Quality ImprovementDocument14 pagesBNS Honours Nursing Quality ImprovementyeapgyNo ratings yet
- Application of Lean Healthcare in Hospital ServiceDocument14 pagesApplication of Lean Healthcare in Hospital ServiceRon patelNo ratings yet
- A Systematic Literature Review of E Measurement in Nursing HomesDocument18 pagesA Systematic Literature Review of E Measurement in Nursing HomesBrian Cruz RinconNo ratings yet
- Healthcare Sustainability Evaluation Using A Hybrid Fuzzy Multi-Criteria Decision-Making ModelDocument21 pagesHealthcare Sustainability Evaluation Using A Hybrid Fuzzy Multi-Criteria Decision-Making ModelANKUSH SINHANo ratings yet
- Hospital Performance Management: A Multi-Criteria Decision-Making ApproachDocument7 pagesHospital Performance Management: A Multi-Criteria Decision-Making Approachmr kevinNo ratings yet
- Working Paper Series: College of Business Administration University of Rhode IslandDocument25 pagesWorking Paper Series: College of Business Administration University of Rhode IslandDeivid Zharatte Enry QuezNo ratings yet
- An Integrated Model For Sustainable Performance Measurement in Supply ChainDocument6 pagesAn Integrated Model For Sustainable Performance Measurement in Supply ChainphanthanhtrungNo ratings yet
- A Review of Frameworks for Implementing Telehealth ServicesDocument20 pagesA Review of Frameworks for Implementing Telehealth ServicesKartik DograNo ratings yet
- Mast Et Al-2011-Quality and Reliability Engineering InternationalDocument12 pagesMast Et Al-2011-Quality and Reliability Engineering InternationalAnonymous 3O0J2YYNo ratings yet
- Critical To Quality in Telemedicine - A Case StudyDocument6 pagesCritical To Quality in Telemedicine - A Case StudydrustagiNo ratings yet
- RoweS - 2022 (HCPPR Supervision Effectiveness)Document12 pagesRoweS - 2022 (HCPPR Supervision Effectiveness)Karen ZamboniNo ratings yet
- Assignment 1Document5 pagesAssignment 1richmond_austria7635No ratings yet
- Research ArticleDocument25 pagesResearch ArticleDanoe SoesantoNo ratings yet
- Review Article Multi-Criteria Decision Making Techniques For Healthcare Service Quality Evaluation: A Literature ReviewDocument12 pagesReview Article Multi-Criteria Decision Making Techniques For Healthcare Service Quality Evaluation: A Literature ReviewANKUSH SINHANo ratings yet
- Effective IT implementation in healthcareDocument8 pagesEffective IT implementation in healthcareSai VishnuNo ratings yet
- The Influence of Contextual Factors On Healthcare Quality Improvement Initiatives: A Realist ReviewDocument22 pagesThe Influence of Contextual Factors On Healthcare Quality Improvement Initiatives: A Realist ReviewArseniojakejr FloresNo ratings yet
- Cheung Et Al - Overview of Systematic Reviews of The Effectiveness of Reminders in Improving Healthcare Professional BehaviorDocument8 pagesCheung Et Al - Overview of Systematic Reviews of The Effectiveness of Reminders in Improving Healthcare Professional BehaviorabcNo ratings yet
- Review Paper On VSM 1Document25 pagesReview Paper On VSM 1THULASI MANOHARANNo ratings yet
- McConnel, Brendon and Vera-Hernandez (2015)Document53 pagesMcConnel, Brendon and Vera-Hernandez (2015)María Ignacia Valenzuela NavarroNo ratings yet
- Integrating New Practices: A Qualitative Study of How Hospital Innovations Become RoutineDocument12 pagesIntegrating New Practices: A Qualitative Study of How Hospital Innovations Become RoutineMas MujionoNo ratings yet
- Hospital BenchmarkingDocument11 pagesHospital BenchmarkingDana ApostolNo ratings yet
- Going Beyond Simple Sample Size Calculations: A Practitioner's GuideDocument56 pagesGoing Beyond Simple Sample Size Calculations: A Practitioner's GuideManuel BéjarNo ratings yet
- 1472-6963-6-86Document11 pages1472-6963-6-86afreenahmadNo ratings yet
- Mapping of Multiple Criteria For Priority Setting of Health Interventions: An Aid For Decision MakersDocument7 pagesMapping of Multiple Criteria For Priority Setting of Health Interventions: An Aid For Decision MakerstemesgenNo ratings yet
- Developing A Theoretical Model and Questionnaire Survey InstrumenDocument42 pagesDeveloping A Theoretical Model and Questionnaire Survey InstrumenRS UNIQUE STUDIONo ratings yet
- Mzi040 PDFDocument6 pagesMzi040 PDFselamat parminNo ratings yet
- Mzi040 PDFDocument6 pagesMzi040 PDFselamat parminNo ratings yet
- Dissertation TopicsDocument54 pagesDissertation TopicsApollo Institute of Hospital Administration50% (4)
- Quality ImprovementDocument18 pagesQuality ImprovementSyeda SanaNo ratings yet
- Management Science LettersDocument10 pagesManagement Science LettersANKUSH SINHANo ratings yet
- Strategi Operasi RUmah SakitDocument4 pagesStrategi Operasi RUmah SakituddindjmNo ratings yet
- The Role of Management Control Systems and Top Teams in Implementing Environmental Sustainability PoliciesDocument12 pagesThe Role of Management Control Systems and Top Teams in Implementing Environmental Sustainability Policiesbackup cmbmpNo ratings yet
- The Challenge of Integrating Ehealth Into Health Care - SystematicDocument23 pagesThe Challenge of Integrating Ehealth Into Health Care - Systematicgreat 9No ratings yet
- Critical Analysis of a Community Nursing Information SystemDocument5 pagesCritical Analysis of a Community Nursing Information SystemAgboola Ayobami AbiolaNo ratings yet
- B.1 Learning Objectives: System Life Cycle: at The End of The Lesson, The Student Should Be Able ToDocument73 pagesB.1 Learning Objectives: System Life Cycle: at The End of The Lesson, The Student Should Be Able ToPark Yoon AeNo ratings yet
- Key Performance Indicators in Hospital Based On Balanced Scorecard ModelDocument8 pagesKey Performance Indicators in Hospital Based On Balanced Scorecard ModelJery JsNo ratings yet
- 26 The Balanced Scorecard of Acute Setting, Development Process, Definition of 20 Strategic Objectives and ImplementationDocument13 pages26 The Balanced Scorecard of Acute Setting, Development Process, Definition of 20 Strategic Objectives and ImplementationpilardiNo ratings yet
- Smart Body Metric Measuring MachineDocument22 pagesSmart Body Metric Measuring MachineIshimwe Moise SeboNo ratings yet
- Econsort GuidelinesDocument5 pagesEconsort GuidelinesHansNo ratings yet
- Evaluation of Healthcare Enterprise Information Systems A Structural Equation ModelDocument4 pagesEvaluation of Healthcare Enterprise Information Systems A Structural Equation ModelBagus HamdaniNo ratings yet
- Molds K Red 2021Document7 pagesMolds K Red 2021putu juniNo ratings yet
- Literature Reviews Purpose of The Literature ReviewDocument12 pagesLiterature Reviews Purpose of The Literature ReviewSonali ChitalkarNo ratings yet
- MacFarlane 2010 NormalizationDocument11 pagesMacFarlane 2010 NormalizationKarina CancellaNo ratings yet
- Being Pragmatic About Healthcare Complexity Our ExDocument9 pagesBeing Pragmatic About Healthcare Complexity Our ExJ Paulo SousaNo ratings yet
- EBMgt 1Document8 pagesEBMgt 1Delelegn EmwodewNo ratings yet
- Festus Olorunniwo - Developing A Service Quality Construct A Pedagogical ApproachDocument10 pagesFestus Olorunniwo - Developing A Service Quality Construct A Pedagogical ApproachNguyen HanhNo ratings yet
- Influence of Key Performance Indicators On Healthcare Quality ImprovementDocument5 pagesInfluence of Key Performance Indicators On Healthcare Quality ImprovementahamedsahibNo ratings yet
- Evidence Based Practice in Postgraduate Healthcare EducationDocument29 pagesEvidence Based Practice in Postgraduate Healthcare EducationGab FgilzcheNo ratings yet
- Risk-Based Bridge ManagementDocument10 pagesRisk-Based Bridge Managementoracle259No ratings yet
- Guidelines For Prioritization of Bridge Replacement, Rehabilitation, and Preservation ProjectsDocument201 pagesGuidelines For Prioritization of Bridge Replacement, Rehabilitation, and Preservation Projectsoracle259No ratings yet
- EIA IrtejaHasanDocument12 pagesEIA IrtejaHasanHarini PugalNo ratings yet
- Analysis and Design of Steel Truss Bridges: January 2017Document84 pagesAnalysis and Design of Steel Truss Bridges: January 2017GILANG NUGROHONo ratings yet
- EABMDocument10 pagesEABMoracle259No ratings yet
- Congestion Adaptive Traffic Light Control and Noti PDFDocument19 pagesCongestion Adaptive Traffic Light Control and Noti PDForacle259No ratings yet
- Capital Improvements Plan DraftDocument91 pagesCapital Improvements Plan Draftoracle259No ratings yet
- Addressing Climate Change in TransportDocument2 pagesAddressing Climate Change in Transportoracle259No ratings yet
- Dwi Nur HumirasDocument8 pagesDwi Nur Humirasoracle259No ratings yet
- Road To Zero Consultation Document July2019 PDFDocument68 pagesRoad To Zero Consultation Document July2019 PDForacle259No ratings yet
- Road To Zero Consultation Document July2019 PDFDocument68 pagesRoad To Zero Consultation Document July2019 PDForacle259No ratings yet
- Risk Register Template - 2015Document3 pagesRisk Register Template - 2015oracle259No ratings yet
- Siemens Smart CityDocument14 pagesSiemens Smart Cityoracle259No ratings yet
- Congestion ReportDocument104 pagesCongestion Reportoracle259No ratings yet
- Board Report GuidanceDocument3 pagesBoard Report Guidanceoracle259No ratings yet
- Life Cycle Performance PDFDocument3 pagesLife Cycle Performance PDForacle259No ratings yet
- DB16 Full Report PDFDocument348 pagesDB16 Full Report PDForacle259No ratings yet
- CDB Country Strategy Jamaica 2014-16 FINALDocument55 pagesCDB Country Strategy Jamaica 2014-16 FINALoracle259No ratings yet
- 2135 SpeedMgmtDocument24 pages2135 SpeedMgmtoracle259No ratings yet
- 4Q13 Investor Presentation FINAL 03 03 14 V4 - tcm3171-582070Document43 pages4Q13 Investor Presentation FINAL 03 03 14 V4 - tcm3171-582070oracle259No ratings yet
- Inception Report CB2 - FinalDocument71 pagesInception Report CB2 - Finaloracle259No ratings yet
- National Planning Summit 2007Document65 pagesNational Planning Summit 2007oracle259No ratings yet
- 2011 Key Performance Indicators in Highway Design and Construction PDFDocument8 pages2011 Key Performance Indicators in Highway Design and Construction PDForacle259No ratings yet
- The Importance of Road Transport For The Competitiveness of EU Business PDFDocument9 pagesThe Importance of Road Transport For The Competitiveness of EU Business PDForacle259No ratings yet
- Mobile Phones and Economic Development in AfricaDocument45 pagesMobile Phones and Economic Development in Africaoracle259No ratings yet
- ComScore 2010 Mobile Year in ReviewDocument32 pagesComScore 2010 Mobile Year in Revieworacle259No ratings yet
- Vibration PPV EstimationDocument8 pagesVibration PPV EstimationJensen TanNo ratings yet
- Second Year Hall Ticket DownloadDocument1 pageSecond Year Hall Ticket DownloadpanditphotohouseNo ratings yet
- Wireless Sensor Network Using Zigbee: Nidhi Patel, Hiren Kathiriya, Arjav BavarvaDocument5 pagesWireless Sensor Network Using Zigbee: Nidhi Patel, Hiren Kathiriya, Arjav BavarvaDavidleonardo GalindoNo ratings yet
- ReadMe STEP7 Professional V14 enUS PDFDocument74 pagesReadMe STEP7 Professional V14 enUS PDFAndre Luis SilvaNo ratings yet
- Fpga Implementation of Ofdm Modem: Asst. Prof, Department of ECE, DBIT, Mysore Road, Bangalore-560074Document6 pagesFpga Implementation of Ofdm Modem: Asst. Prof, Department of ECE, DBIT, Mysore Road, Bangalore-560074lambanaveenNo ratings yet
- Joybook A52 Series EnglishDocument44 pagesJoybook A52 Series EnglishTudor VladNo ratings yet
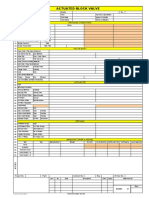
- DSS2060D Actuated Block Valve DatasheetDocument1 pageDSS2060D Actuated Block Valve Datasheetkrishna kumarNo ratings yet
- Design and analyze a non-inverting op-amp circuit with gain of 10Document7 pagesDesign and analyze a non-inverting op-amp circuit with gain of 10Mandeep KaloniaNo ratings yet
- My Dream in The Drawer English Bookdash FKB StoriesDocument19 pagesMy Dream in The Drawer English Bookdash FKB StoriesonkNo ratings yet
- BDS Maschinen MABasicDocument4 pagesBDS Maschinen MABasicJOAQUINNo ratings yet
- FS7M0680, FS7M0880: Fairchild Power Switch (FPS)Document19 pagesFS7M0680, FS7M0880: Fairchild Power Switch (FPS)Arokiaraj RajNo ratings yet
- CV Edin Fatic2Document2 pagesCV Edin Fatic2yousab creator2No ratings yet
- Psa 3000Document2 pagesPsa 3000diegoh_silvaNo ratings yet
- XCC 638Document32 pagesXCC 638Nico NicoNo ratings yet
- Proceeding 4th Ismei - FinalDocument412 pagesProceeding 4th Ismei - FinalAchmad NizarNo ratings yet
- Korea Battery Product Catalogue 2023Document8 pagesKorea Battery Product Catalogue 2023Cesar GarciaNo ratings yet
- Euref2 English PDFDocument10 pagesEuref2 English PDFbasileusbyzantiumNo ratings yet
- Candlescript IntroductionDocument26 pagesCandlescript IntroductionLucasLavoisierNo ratings yet
- Recruitment Brochure: National University of Study and Research in Law RanchiDocument15 pagesRecruitment Brochure: National University of Study and Research in Law RanchiSiddharth SinghNo ratings yet
- 0111 Tension Load Cell Datasheet enDocument2 pages0111 Tension Load Cell Datasheet enJosipaNo ratings yet
- Wind Load On Cable TraysDocument10 pagesWind Load On Cable TraysAaron EasleyNo ratings yet