You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- x2 Electric Bike ManualDocument16 pagesx2 Electric Bike ManualwroxtarNo ratings yet
- Jihad-al-Nikah or Sex Jihad: 10 Interesting FactsDocument2 pagesJihad-al-Nikah or Sex Jihad: 10 Interesting FactsShyam Dass GuptaNo ratings yet
- CONTROLDocument12 pagesCONTROLTaseen JannatNo ratings yet
- Lamal (1991) - Behavioral Analysis of Societies and Cultural PracticesDocument257 pagesLamal (1991) - Behavioral Analysis of Societies and Cultural PracticesDan Campoz100% (1)
- Design Optimization of Ice Plant Test-Rig: H. S. Salave, V. N. RaibholeDocument6 pagesDesign Optimization of Ice Plant Test-Rig: H. S. Salave, V. N. RaibholeNeeraj SamadhiyaNo ratings yet
- Surveys and InspectionDocument2 pagesSurveys and InspectionJude Herbert TacalanNo ratings yet
- Excel Containment SizingDocument7 pagesExcel Containment SizingAbraham JyothimonNo ratings yet
- HPWJ Safety Procedures RIL ARCDocument17 pagesHPWJ Safety Procedures RIL ARCvishal bailurNo ratings yet
- Sexism EssayDocument5 pagesSexism Essayd3gpmvqw100% (2)
- Connecting You to EmploymentDocument29 pagesConnecting You to EmploymenthaticeNo ratings yet
- WALLPAPER GUIDEDocument6 pagesWALLPAPER GUIDEFaiz BungkalNo ratings yet
- Easy Do-In Exercises Promote HappinessDocument15 pagesEasy Do-In Exercises Promote Happinesssale18100% (1)
- Homework Method of ImagesDocument6 pagesHomework Method of ImagesBrenda Michelle ReyesNo ratings yet
- 7 Bond and Development Length-SlightDocument47 pages7 Bond and Development Length-Slightريام الموسويNo ratings yet
- ArresterWorks Facts-001 Arrester Lead LengthDocument11 pagesArresterWorks Facts-001 Arrester Lead Lengthnshj196No ratings yet
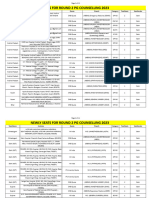
- Newly Seats For Round 2 PG Counselling 2023Document11 pagesNewly Seats For Round 2 PG Counselling 2023Manoj KumarNo ratings yet
- Final Draft Research PaperDocument6 pagesFinal Draft Research Paperapi-549464161No ratings yet
- Iagg Abstract BookDocument1,452 pagesIagg Abstract BookjclamasNo ratings yet
- PMET 885 Technical DatasheetDocument1 pagePMET 885 Technical Datasheet.xNo ratings yet
- Building HVAC RequirementsDocument111 pagesBuilding HVAC RequirementsNagarathna ShivaramNo ratings yet
- Bournvita Project ReportDocument43 pagesBournvita Project Reportlatikalatika100% (6)
- Csb601 A2 Patient Assessment (Group Assignment) Case Study 2023s2 FinalDocument2 pagesCsb601 A2 Patient Assessment (Group Assignment) Case Study 2023s2 FinalSaem HashmiNo ratings yet
- 2017, 9999, N/a-N/a 9999 : Icole Odriguez Egan Evesque Ictoria Ohrs AND Essica IemeierDocument16 pages2017, 9999, N/a-N/a 9999 : Icole Odriguez Egan Evesque Ictoria Ohrs AND Essica IemeierAndré Luíz FerreiraNo ratings yet
- Methyl T-Butyl Ether (Mtbe) Production: A Comparison of Montmorillonite-Derived Catalysts With Ion-Exchange ResinDocument7 pagesMethyl T-Butyl Ether (Mtbe) Production: A Comparison of Montmorillonite-Derived Catalysts With Ion-Exchange ResinTrà ĐáNo ratings yet
- Gsef 2021 Research Plan Project Summary InstructionsDocument1 pageGsef 2021 Research Plan Project Summary Instructionsapi-550508557No ratings yet
- Ess 6Document6 pagesEss 6api-582020074No ratings yet
- Traction ContraindicationsDocument2 pagesTraction ContraindicationslaymanzNo ratings yet
- ProjectDocument18 pagesProjectrbangaram_1No ratings yet
- IJMS - Volume 49 - Issue 1 - Pages 1-9Document9 pagesIJMS - Volume 49 - Issue 1 - Pages 1-9metaversajNo ratings yet
- 08.2279 USD2461b (1) Supor EKV BRODocument16 pages08.2279 USD2461b (1) Supor EKV BROMichał KoczorowskiNo ratings yet