Professional Documents
Culture Documents
Diffusion-Weighted Imaging and Demyelinating Diseases: New Aspects of An Old Advanced Sequence
Uploaded by
aditOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Diffusion-Weighted Imaging and Demyelinating Diseases: New Aspects of An Old Advanced Sequence
Uploaded by
aditCopyright:
Available Formats
N e u r o r a d i o l o g y / H e a d a n d N e c k I m a g i n g • R ev i ew
Rueda-Lopes et al.
Diffusion-Weighted Imaging of Demyelinating Diseases
Neuroradiology/Head and Neck Imaging
Review
Downloaded from www.ajronline.org by KAGOSHIMA UNIVERSITY on 12/08/15 from IP address 163.209.223.17. Copyright ARRS. For personal use only; all rights reserved
Diffusion-Weighted Imaging
and Demyelinating Diseases:
FOCUS ON:
New Aspects of an Old
Advanced Sequence
Fernanda C. Rueda-Lopes1 OBJECTIVE. The purpose of this article is to discuss classic applications in diffusion-
Luiz C. Hygino da Cruz, Jr. weighted imaging (DWI) in demyelinating disease and progression of DWI in the near future.
Thomas M. Doring CONCLUSION. DWI is an advanced technique used in the follow-up of demyelinating
Emerson L. Gasparetto disease patients, focusing on the diagnosis of a new lesion before contrast enhancement. With
technical advances, diffusion-tensor imaging; new postprocessing techniques, such as tract-
Rueda-Lopes FC, Hygino da Cruz LC Jr, Doring TM, based spatial statistics; new ways of calculating diffusion, such as kurtosis; and new applica-
Gasparetto EL tions for DWI and its spectrum are about to arise.
D
iffusion-weighted imaging (DWI), imaging (DTI) with its various parameters,
one of the first advanced MRI including axial and radial diffusion, has al-
techniques, has rapidly ascended lowed the description of intrinsic white mat-
on the basis of its applicability in ter (WM) damage [8, 9]. The demyelination
strokes and some infectious diseases [1–4]. process and neuronal loss are now part of the
Restricted diffusion is significant informa- context of imaging findings. Postprocessing
tion in the context of vascular ischemia, help- techniques, such as tract-based spatial statis-
ing to delimit the brain-damaged area [5]. tics (TBSS) [10], have provided new research
Nonetheless, the utility of DWI in assessing opportunities, including mapping normal-
demyelinating disease has always been ques- appearing WM damage, reflecting its greater
tionable, and the main clinical utility of this sensitivity for detecting initial WM lesions
sequence could be in helping with the differ- compared with conventional MRI [11].
ential diagnosis [1–5]. The most described A new era of diffusion is about to begin.
aspect of demyelinating disease in DWI is fa- Diffusion kurtosis imaging (DKI) is a new
cilitated diffusion [5, 6]. However, restricted DWI approach considered even more sensi-
diffusion may occur at early stages of lesion tive than DTI and TBSS for microscopic WM
Keywords: demyelinating, diffusion-tensor imaging, progression [6]. The apparent diffusion coef- lesion detection. Some reports are appearing
diffusion-weighted imaging, kurtosis, tract-based spatial ficient (ADC), a map calculated from DWI on this topic, and DKI seems to be better than
statistics (TBSS) data, has also been extensively investigated DWI in assessing WM [12, 13]. Taking into
DOI:10.2214/AJR.13.11400
to establish a connection with disease severi- account all this advancement of DWI and its
ty and clinical correlation. Another applica- related aspects, we will discuss the main ap-
Received June 17, 2013; accepted after revision tion for DWI is its capacity to evaluate tissue plications for clinical aspects and research.
August 25, 2013. characteristics in patients with demyelinating
1 disease. Conventional T2-weighted images Diffusion-Weighted Imaging
All authors: Department of Radiology, Federal University
of Rio de Janeiro, Clinica de Diagnostico por imagem– are highly sensitive in depicting focal demy- Principles and Acquisition
CDPI/DASA, Rua: Eneida de Morais, 141/203. Ilha do elinating lesions but lack histopathologic Diffusion describes the transfer of water
Governador, Rio de Janeiro, RJ, Brazil, CEP 21920-230. specificity, such as inflammation, edema, gli- molecules from one spatial location to other
Address correspondence to F. C. Rueda-Lopes osis, and axonal loss, which are all represent- locations, increased by thermal agitation in-
(frueda81@hotmail.com).
ed as areas of high signal intensity. Because side a sample of biologic tissue [8, 9]. Random
WEB of this lack of specificity, T2-weighted imag- movement, or Brownian motion, is the result
This is a web exclusive article. ing does not provide information that can be of a movement without a preferred direction,
reliably associated with the pathologic sub- in which molecules collide randomly, typical
AJR 2014; 202:W34–W42
strate and clinical status of the patient, which of diffusion in pure water. This nondirected
0361–803X/14/2021–W34 can be determined using DWI [7]. movement is also called “isotropic diffusion”
Over the past decade, new insight has been in which water molecules move equally in all
© American Roentgen Ray Society gained into DWI. The use of diffusion tensor directions. In biologic tissue, especially brain
W34 AJR:202, January 2014
Diffusion-Weighted Imaging of Demyelinating Diseases
tissue in which the WM tracts may serve as including intramyelinic edema (cytotoxic oli- gies, which are quick, efficient, and insensi-
pathways that the water molecules are able godendroglia edema) or myelin vacuolation tive to small motion, with the incorporation
to follow, a directed movement occurs. This and reversible reduced vascular input. Myelin of a diffusion-sensitized module [8]. This
property is called “anisotropic diffusion.” breakdown and inflammatory cell infiltration sensitization scheme can be achieved by a bi-
Downloaded from www.ajronline.org by KAGOSHIMA UNIVERSITY on 12/08/15 from IP address 163.209.223.17. Copyright ARRS. For personal use only; all rights reserved
The diffusion of water in biologic tissues oc- may reduce water movement in the extracel- polar gradient waveform before and after the
curs inside, outside, around, and through cel- lular space because of reduced fiber tract or- 180° refocusing radiofrequency pulse. The
lular structures [8]. Nonetheless, when water ganization. Likewise, this inflammatory influx first gradient pulse dephases the magnetiza-
molecules encounter structures, such as mye- can lead to disturbances of energy metabolism, tion across the sample and the second pulse
lin sheaths, axonal membranes, or subcellular namely mitochondrial dysfunction, notably rephases the magnetization. For nondiffusing
organelles, their continued motion in a partic- in acute lesions [5, 6, 15, 16]. The presence of molecules representing restricted diffusion,
ular direction can be impeded [14]. iron-laden macrophages in this inflammatory the phases induced by both gradients will be
Reduction of the motion along pathways re- process can result in an overall lack of DWI completely canceled, the magnetization will
flects the interaction between the water mole- signal because of very rapid T2* relaxation, be maximally coherent, and there will be no
cules and the damaged structures, called “re- the same as seen in the center of an abscess [5]. signal attenuation from diffusion, represent-
stricted diffusion.” There are many causes for DWI is acquired most commonly with sin- ing the high signal intensity on a classic DWI
restricted diffusion in demyelinating diseases, gle-shot echo-planar imaging (EPI) strate- map [8, 9].
30
15
4 3 2 1
A B C
D E F
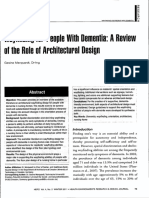
Fig. 1—Tumefactive demyelinating plaque in 41-year-old man.
A–C, FLAIR (A) and contrast-enhanced T1-weighted (B) images show expansive lesion with hypersignal intensity on FLAIR and irregular rim of contrast enhancement
located in right centrum semiovale. Notice increased choline peak on spectroscopy image (C).
D and E, Enhancing ring corresponds with area of restricted diffusion on trace image (D) and apparent diffusion coefficient map (E).
F, Susceptibility weighted image shows many small venosus vessels penetrating lesion.
AJR:202, January 2014 W35
Rueda-Lopes et al.
The sensitization profile of the gradient is such as lymphoma and small cell carcino- T2-weighted image alterations, in the course
determined by the b factor. The higher the b ma of the lung; and hyperacute hemorrhage of disease (Fig. 2). ADC reduction may be a
factor, the more diffusion weighted the im- can have restricted diffusion [2–4]. Howev- transient alteration in the hyperacute phase
age will be. A typical DWI sequence for rou- er, DWI findings may vary from normal to of a demyelinating lesion. To depict such an
Downloaded from www.ajronline.org by KAGOSHIMA UNIVERSITY on 12/08/15 from IP address 163.209.223.17. Copyright ARRS. For personal use only; all rights reserved
tine brain MRI protocols includes a b factor facilitated diffusibility within neoplastic le- abnormality, MRI should be performed in
of 1000 s/mm2 (ideal between 700 and 1300 sions [2–4]. Intracerebral abscesses usually the early phase after clinical symptom onset
s/mm2). At high b values, the signal intensi- have restricted diffusion centrally after com- (from hours up to 2 days) or even before the
ty will be reduced. A b value of zero means plete formation. In the early stages, abscesses symptoms [6]. By this time, T2-weighted im-
application of the normal single-shot EPI se- may have peripheral restricted diffusion [1]. aging abnormalities are not yet significant and
quence without diffusion weighting. In prac- Diffusion restriction is found throughout the the lack of contrast enhancement reflects that
tice, it is denominated as a b 0 image and is ischemic tissue, with the lowest ADC values the increased permeability of the blood-brain
similar to a T2-weighted image. To evalu- detected in the infarct core [5]. There is no es- barrier and the edematous tissue changes are
ate diffusion properties of the tissue, the se- tablished diffusion pattern for demyelinating not fully developed. Within gradual develop-
quences have to be sensitized in three dif- plaques, but variable ADC patterns in a sin- ment of signals of prominent inflammatory
ferent dimensions. The diffusion coefficient gle MRI study (representing different stages edematous changes, which enlarge the extra-
generated is proportional to the displacement of lesion progression) and rapid changes in cellular space, ADC reaches a brief pseudo-
of water molecules (which may be tortuous such patterns on previous reports are high- normalization and subsequent increase of val-
depending on membrane barriers) and is di- ly suggestive of demyelinating disease. The ues, usually 3–7 days after symptom onset
vided by the number of dimensions, usual- most common ADC finding is homogeneous- [15]. Different case descriptions confirm the
ly three. Trace diffusion imaging and ADC ly facilitated because of vasogenic edema [5, changing pattern of ADC within a demyelin-
maps, representing the magnitude of the dif- 6, 17]. However, homogeneous restriction, ating lesion. Acute disseminated encephalo-
fusion and the trace divided by three, are cal- peripheral restriction with a partial or com- myelitis and relapsing-remitting MS patients
culated from the raw diffusion images of the plete dark ring surrounding a bright center, or may have acute lesions showing decreased
scanner. In practice, the restricted diffusion central facilitation with an isointense periph- ADC values, which become facilitated dur-
represents a decrease in the apparent diffu- eral ring or homogeneously isointense can ing the subacute stage [16, 18].
sivity of water [8, 17]. also be seen [5]. In our practice, the incom- ADC is a potential marker for disease se-
plete peripheral restriction ring usually en- verity. Low signal intensity on ADC, which
Clinical Applications hances with contrast administration, notably represents restricted diffusion, is associated
An important clinical application for DWI in the medial zone of an acute lesion (Fig. 1). with higher expanded disability status scale
in demyelinating disease is in establishing a Thin slices of sagittal FLAIR sequences, (EDSS) score at the index attack. Moreover,
differential diagnosis with other pathologies. including the corpus callosum are useful for neurologic deterioration may be accompanied
In some circumstances, tumefactive inflam- early diagnosis of multiple sclerosis (MS) with ADC variation from homogeneously fa-
matory lesions may mimic a cerebral neo- [17]. But in some specific and rare situations, cilitated to a dark or isointense ring pattern.
plasm, infectious abscess, or vascular isch- restricted diffusion can be the first marker This restricted diffusion could reflect a great-
emia. Most high-grade gliomas; metastases; for a demyelinating lesion, preceding con- er extent of inflammation and tissue dam-
tumors with high nuclear-cytoplasmic ratios, trast enhancement and associated with subtle age in such patients [5]. The damage severity
A B C
Fig. 2—25-year-old woman with demyelinating lesion.
A–C, Demyelinating plaque is seen in left middle cerebellar peduncle (green circle) showing restricted diffusion with hypointense signal intensity on apparent diffusion
coefficient (ADC) map (A) and hyperintense signal intensity on trace image (B). Notice no contrast enhancement is seen in that location on contrast-enhanced T1-
weighted image (C), reflecting hyperacute demyelinating plaque. On same contrast-enhanced T1-weighted image, there is another focus of enhancement (blue circle, C),
located in right cerebellar peduncle close to fourth ventricle wall, with hyperintense signal on trace image (blue circle, B) and isointense signal on ADC map (blue circle,
A), representing most common demyelinating lesion behavior on diffusion-weighted imaging.
W36 AJR:202, January 2014
Diffusion-Weighted Imaging of Demyelinating Diseases
Downloaded from www.ajronline.org by KAGOSHIMA UNIVERSITY on 12/08/15 from IP address 163.209.223.17. Copyright ARRS. For personal use only; all rights reserved
A B C
Fig. 3—37-year-old man with spinal cord demyelinating lesions.
A, Sagittal STIR image of dorsal spinal cord shows demyelinating plaque in inferior dorsal segment (red circle) and normal-appearing white matter (WM) damage in
superior segment (green circle).
B and C, Fractional anisotropy colored map (B) of dorsal spinal cord and corresponding apparent diffusion coefficient (ADC) map (C) show dorsal WM tracts are highly
anisotropic and main diffusion direction is in head-to-foot orientation (blue, B). Notice that fractional anisotropy value is lower in plaque (0.56 ± 0.11) and mean diffusivity
(1.30 ± 0.17 × 10 −3 mm2 /s) compared with normal-appearing WM damage fractional anisotropy (0.83 ± 0.28) and mean diffusivity (0.84 ± 0.05 × 10 −3 mm2 /s), and opposite
holds true for ADC value.
and ADC value correlation was confirmed by ty, including on the parallel and perpendicu- the number of averages is increased, DTI ac-
comparison between low-signal-intensity le- lar axes. The diffusion tensor may be visu- curacy will improve, but the scanning time
sions on T1-weighted imaging and ADC val- alized as an ellipsoid, with the eigenvectors will increase [8]. The use of 3-T scanners,
ues on secondary progressive MS patients. defining the directions of the principal axis with a higher signal-to-noise ratio, may also
The lower the signal intensity on T1-weighted and the eigenvalues (ג1, ג2, ג3) the diffusion improve the sequence acquisition. DTI tech-
imaging, the higher ADC tends to be, repre- coefficients in the main directions. To char- nique also should be position-invariant but
senting the so-called “black holes,” which are acterize diffusion as anisotropic, the eigen- only for a voxel with the size of a point; for
related to significant tissue destruction, prob- values are different in magnitude along dif- all other applications, head angulation does
ably secondary to axonal loss [7]. ferent axes, and the eigenvector parallel to matter and should be standardized. The pa-
the WM tracts is the principal eigenvector. rameters provided by DTI using the eigen-
Diffusion Tensor Imaging This magnitude may be affected by local tis- vectors and eigenvalues are mean diffusivi-
Principles and Acquisition sue injury, modifying the diffusion param- ty, which is quite similar to ADC, fractional
In WM, water diffusion is relatively un- eter values and thus helping to characterize anisotropy, radial diffusivity, and axial dif-
impeded parallel to the fiber orientation and abnormal microstructure [8, 9, 19, 20]. fusivity. The mean diffusivity gives an over-
relatively restricted perpendicular to its fi- To perform DTI, a minimum of six noncol- all measure of the water diffusion in a vox-
bers, defined as anisotropism. DTI will allow linear diffusion-encoding directions is neces- el or region, whereas fractional anisotropy is
the measurement of orientation of diffusivi- sary. If the number of encoding directions or a measure of the degree of anisotropy. Frac-
AJR:202, January 2014 W37
Rueda-Lopes et al.
tional anisotropy ranges from 1 (anisotropic
diffusion) to 0 (isotropic diffusion). The radial
diffusivity [(ג2 + ג3) / 2] and axial diffusivity
(ג1) are measures of the orthogonal and paral-
Downloaded from www.ajronline.org by KAGOSHIMA UNIVERSITY on 12/08/15 from IP address 163.209.223.17. Copyright ARRS. For personal use only; all rights reserved
lel diffusivities, respectively, to the main dif-
fusion directions [8, 9, 19, 20]. Radial diffu-
sivity is modulated by myelin in white matter,
whereas axial diffusivity is more specific to
axonal degeneration [8, 19, 21]. When applied
together, these DTI parameters will evaluate
the WM tracts, indicating areas of lesions not
detected on conventional MRI and identifying
damage in the normal-appearing WM [9, 20]. Fig. 4—Tract-based spatial statistics. Corrected p maps overlaid on skeleton (green) and mean fractional
anisotropy image (gray scale). Skeleton shows main tracts where statistical analysis was carried out. Orange
Clinical and Research Applications areas show fractional anisotropy is significantly reduced (p < 0.05) in one group compared with another.
The investigation of the normal-appear-
ing WM damage using DWI and DTI tech- spiratory movement artifacts. Some articles in The results are significant maps correct-
niques gave a new direction to the radiologic this field reflect the same brain findings. There ed for multiple comparisons, which can show
approach concerning demyelinating disease. is extensive damage of the normal-appearing significant alterations in diffusion param-
As previously mentioned, in clinical prac- WM, reflected by decreased fractional anisotro- eters between groups of study. All DTI pa-
tice, DWI can be helpful in identifying ac- py values and increased mean diffusivity values rameters are analyzed, including fractional
tive demyelinating lesions [5, 17, 18] and for [30, 31], including in patients with NMO [31]. anisotropy, mean diffusivity, axial diffusiv-
differential diagnosis with some conditions The majority of previous studies assessing ity, and radial diffusivity [10].
that can mimic demyelinating disease [1–5]. DTI findings in demyelinating disease have
DTI application clarified the general under- used region of interest (ROI)-based analysis. Research Applications
standing about some histopathologic aspects Standard limitations of the ROI approach are TBSS is a postprocessing technique pre-
of the structural WM damage in demyelinat- that the method is subjective, presents diffi- dominantly used for research purposes. TBSS
ing disease [19, 20]. DTI can identify a broad culties in reapplication, and is necessarily hy- allows group analysis of all major WM tracts,
area of a WM lesion not identified by conven- pothesis driven; thus, the entire WM is not providing an overview of WM damage, in-
tional MRI techniques and that could only assessed [28, 29, 32]. A new approach, vox- cluding normal-appearing WM damage. In-
be accessed by histopathologic examination. el-based analysis, is more general and robust; deed, TBSS is helping in the identification
In general, MS lesions have decreased frac- the statistical analysis is more reliable; and of the histopathogenesis behind all structural
tional anisotropy values and increased mean the total brain tissue is evaluated, which is damage in a noninvasive manner, contributing
diffusivity values compared with the con- proportioned by TBSS [10]. toward the general knowledge of demyelinat-
tralateral normal-appearing WM damage ing disease evolution. With this technique, dif-
and healthy control subjects [17]. Reduced Tract-Based Spatial Statistics ferent groups of diseases can be studied and
fractional anisotropy values in the normal- Postprocessing Principles compared, highlighting the differences be-
appearing WM damage surrounding demy- TBSS is an observer-independent and hy- tween phenotypes, clinical course, age of on-
elinating plaques reflect wide involvement pothesis-free method that provides the abil- set, and so on [32–34].
because the lesion is greater than it seems to ity to spatially locate group differences in Studies using TBSS have revealed that WM
be on conventional sequences [9, 14, 22–26]. the DTI data. In such a technique, fraction- damage is already widespread when detected
Within other DTI parameters, such as ra- al anisotropy data for individual subjects are in pediatric MS onset (patients younger than
dial diffusivity and axial diffusivity, the con- projected on a common space in a way that 18 years at onset). The most common plac-
tribution of demyelination and axonal loss does not depend on perfect nonlinear record- es for fractional anisotropy reduction are the
for this damage may be estimated. The cor- ing, differing from the other voxel analysis splenium of the corpus callosum and parietal
pus callosum has been extensively studied by tool. This is achieved through the use of an areas, which correlate with disease duration
DTI parameters [27, 28], and the results may initial approximate nonlinear recording, fol- [33]. But pediatric onset itself is also a predic-
also be used as a tool to differentiate MS lowed by projection on an alignment-invari- tor of WM damage. The premature beginning
from other demyelinating diseases, such as ant tract representation (the ‘‘mean fractional of MS is worse, and such patients have exten-
neuromyelitis optica (NMO) [29]. However, anisotropy skeleton’’). The skeleton repre- sive lower fractional anisotropy when com-
more effort is needed in this field to make sents the centers of all fiber bundles that are pared with groups of patients matched for age
DTI a useful technique for demyelinating generally common to the subject involved in and disease duration [34].
disease follow-up. a study. Each subject’s fractional anisotropy Clinically isolated syndrome patients are an-
DTI parameters have also been evaluated data are then projected on the mean fractional other important group for analysis by TBSS.
in the spinal cord [30, 31] (Fig. 3). There are anisotropy skeleton in such a way that each Decreased fractional anisotropy values in-
many technical issues regarding DTI acquisi- skeleton voxel takes the fractional anisotropy volving the most significant WM pathways,
tion in the cord because there is extensive bone value from the local center of the nearest rel- including the corticospinal tracts, corpus cal-
structure surrounding the neural tissue and re- evant tract [10] (Fig. 4). losum, and longitudinal fasciculi, when com-
W38 AJR:202, January 2014
Diffusion-Weighted Imaging of Demyelinating Diseases
Downloaded from www.ajronline.org by KAGOSHIMA UNIVERSITY on 12/08/15 from IP address 163.209.223.17. Copyright ARRS. For personal use only; all rights reserved
A B C
D E F
Fig. 5—Parametric DKI maps. Values of parameters
are described in Table 1.
A–D, Proton density image (A) shows hypersignal
intensity representing demyelinating lesion on the
ROI located in right frontal side. ROI in left side
represents NAWM. Other maps are axial diffusivity
(B), radial diffusivity (C) and mean diffusivity (D)
maps.
E–H, Fractional anisotropy map (E) and diffusion
kurtosis imaging maps of axial kurtosis (F), radial
kurtosis (G), and mean kurtosis (H).
aspects, mostly cognition impairment [11, 38–
40]. Since the first descriptions of MS, the cor-
pus callosum has been described as the center
of demyelinating lesions, and good judgment
for radiologic MS diagnosis includes consid-
ering lesions in this location highly sugges-
G H tive of MS [27, 28]. But corpus callosum le-
sions or any other lesions are not necessarily
pared with control subjects are described in year of conversion [37], but they definitely in- evident as causes for disturbances in MS, re-
clinically isolated syndrome [35]. These struc- crease during disease progression [11, 36]. flecting the contribution of normal-appearing
tural changes may not be significant at the be- The detection of microstructure damage is WM damage in cognitive abnormality [11,
ginning of the disease [36] or during the next also important in the correlation with clinical 38]. Fractional anisotropy variations in the
AJR:202, January 2014 W39
Rueda-Lopes et al.
normal-appearing WM damage of the corpus mains is predicted [39]. Again, corpus cal- sion barriers, thus causing water diffusion to
callosum have already been detected by ROI losum damage may result in a disconnection deviate from gaussianity. So, DKI is theoreti-
analysis [27, 28], but its correlation with cog- syndrome that contributes to long-term MS cally better able to characterize microstructur-
nitive impairment is mostly described using disability [39]. al brain tissue [44]. One main difference with
Downloaded from www.ajronline.org by KAGOSHIMA UNIVERSITY on 12/08/15 from IP address 163.209.223.17. Copyright ARRS. For personal use only; all rights reserved
a voxel-based analysis method [11, 38–40]. In NMO patients, TBSS revealed a new facet DTI is that the signal decay is not monolog-
The corpus callosum is one of the main impor- of brain involvement [32, 43]. Widespread WM arithmic but includes a logarithmic extension
tant structures connecting both cerebral hemi- damage was detected in the normal-appearing that incorporates diffusion kurtosis [13, 45],
spheres, and its disconnection may be a po- WM damage, including the corpus callosum, a unitless quantitative measure of the devia-
tential mechanism for physical and cognitive internal and external capsules, and both longi- tion from the gaussian distribution (in other
disability in MS [38, 39]. Different cognitive tudinal fasciculi. Typically, this damage is not words, the degree of restricted diffusion). Not
domains are impaired in MS patients, includ- merely affecting visual and motor pathways only six—as necessary in DTI—but at least 15
ing processing speed, which is correlated with secondary to Wallerian degeneration from op- independent diffusion directions (gradients)
abnormal fractional anisotropy in the corpus tical neuritis and spinal cord affection, but also within three different b values have to be ac-
callosum [11]. This same domain is correlat- this in situ WM lesion, mostly correlated with quired to completely calculate diffusion kur-
ed with fractional anisotropy reduction main- demyelination, provides significant new infor- tosis parameters. Unlike DTI, the maximum b
ly associated with variations in radial diffusiv- mation about such a condition [32]. value is higher in DKI, therefore commonly
ity and reflecting myelin disarrangement as With improvements in TBSS and continu- used b values are 0, 1000, and 2000 s/mm2. In
a significant contributor to the damage [40]. ous evaluation of different demyelinating dis- a typical DKI acquisition, besides the com-
Sustained attention, working memory, visu- ease cohorts, it will be possible to map the mon diffusion parameters, such as mean dif-
al working memory, and verbal learning and most common areas of normal-appearing WM fusivity, axial diffusivity, radial diffusivity,
recall are associated with differential patterns damage lesions and the way in which the dam- and fractional anisotropy, diffusion kurtosis
of fractional anisotropy reduction. Likewise, age progresses over the years, and it may be parameters are estimated, including the mean
these damaged tracts interconnect cortical re- possible to use this technique for radiologic kurtosis and the two directional kurtosis pa-
gions thought to be involved with processing follow-up of patients and medication trials. rameters, radial kurtosis and axial kurtosis [13,
in these cognitive domains or even in possible 45] (Fig. 5 and Table 1).
compensatory pathways [38]. Diffusion Kurtosis Imaging
Correlations between TBSS parameters Principles and Differences Between DTI Interpretation of Diffusion Kurtosis Imaging
and motor index are also possible. Increasing and DKI Parameters and Main Applications
EDSS scores and decreasing fractional an- Diffusion kurtosis imaging (DKI) is a novel Mean kurtosis gives an overall measure-
isotropy values can be found in the splenium imaging technique and an extension of the DTI ment of diffusion kurtosis in the ROI. When
of the corpus callosum and along the cortico- model that allows simultaneous estimation of anisotropic diffusion occurs—for example
spinal tract. The correlation of changes with diffusion and kurtosis parameters [12]. DKI within the nerve fibers—the directional kurto-
radial diffusivity points toward the myelin enables a more accurate description of pro- sis parameters, such as radial kurtosis and ax-
process as the major participant in damage ton diffusion than DTI, considering that diffu- ial kurtosis, can respectively describe the dif-
[41, 42]. TBSS parameters may serve as pre- sion occurs differently from that described by fusion kurtosis perpendicular to and along the
dictors for motor outcome in primary pro- a gaussian diffusion probability distribution main eigenvector. In a previous study apply-
gressive MS. Lower fractional anisotropy in for free diffusion. Actually, gaussian diffusion ing DKI to correlate kurtosis parameters with
the splenium of the corpus callosum predicts of the water is only seen in homogeneous so- brain maturation and the myelination process
a greater progression of disability in 5 years lutions. Water diffusibility in biologic tissues, in rat brains, the authors showed that the diffu-
of follow-up. When the fractional anisotro- such as brain, often shows nongaussian behav- sion kurtosis parameters, especially radial kur-
py reduction of the entire corpus callosum is ior [13] because neurologic tissue is more mi- tosis, showed higher sensitivity to the degree
noted, worsening of the major cognitive do- crostructurally complex and has more diffu- of myelination [46]. This is reflected by an in-
TABLE 1: Values for Diffusion Tensor Imaging and Diffusion Kurtosis Imaging for Lesions Described on Proton Density
Image and Contralateral Normal-Appearing White Matter Damage
Region of Fractional
Interest Anisotropy Mean Diffusivity Mean Kurtosis Axial Diffusivity Axial Kurtosis Radial Diffusivity Radial Kurtosis
Lesion
a 0.296 1.155 0.665 1.524 0.736 0.955 0.678
std 0.09 0.085 0.041 0.220 0.155 0.073 0.081
Contralateral
a 0.535 0.907 0.851 1.528 0.776 0.597 0.804
std 0.05 0.03 0.037 0.107 0.080 0.026 0.086
Note—Fractional anisotropy values are lower in the lesion compared with contralateral ROI. The mean kurtosis and radial kurtosis values vary in an opposite
manner. There are increased mean diffusivity and radial diffusivity values and decreased mean kurtosis and radial kurtosis values within the lesion, as
described in the text. Axial diffusivity and axial kurtosis values are not different between lesion and normal-appearing WM damage, probably reflecting
predominance of demyelination in such lesions. a = average, std = standard deviation.
W40 AJR:202, January 2014
Diffusion-Weighted Imaging of Demyelinating Diseases
crease in radial kurtosis because the diffusion tions than DTI, giving more stability and re- and it appears to be more useful for provid-
is more restricted perpendicular to the axon liability to the tensor. Boundaries between dif- ing cortex diffusion measurements.
due to the growing myelin shell. Inversely, ferent tissue types, crossing WM pathways and In the near future, radiologic and thera-
during the demyelination process, commonly fiber orientation distribution, axon diameter, peutic trial follow-up techniques and pat-
Downloaded from www.ajronline.org by KAGOSHIMA UNIVERSITY on 12/08/15 from IP address 163.209.223.17. Copyright ARRS. For personal use only; all rights reserved
seen in demyelinating diseases, radial kurto- and density are better analyzed by high-angu- terns of diffuse WM involvement may be es-
sis decreases because diffusion occurs more lar-resolution diffusion imaging than DTI. For tablished using these advanced techniques to
freely, and DTI radial diffusivity will increase. cortex tissue evaluation, where the dominant highlight the damage that is not revealed by
An advantage of DKI over DTI in the as- orientation varies widely, Q-Ball orientation conventional sequences.
sessment of demyelinating disease is the eval- distribution function may be a better choice.
uation of fiber crossing regions. Mean kur- This feature is independent of orientation and References
tosis values are relatively preserved in these so is able to associate voxels with similar mi- 1. Guo AC, Provenzale JM, Cruz LC Jr, Petrella JR.
regions, whereas fractional anisotropy values crostructure but different orientation [49]. Cerebral abscesses: investigation using apparent
are mistakenly lower in crossing fibers com- diffusion coefficient maps. Neuroradiology 2001;
pared with the surrounding normal WM [47]. Conclusion 43:370–374
This DKI advantage might be useful in the DWI is an interesting technique for evaluat- 2. Cruz LC Jr, Sorensen AG. Diffusion tensor mag-
evaluation of normal-appearing WM damage ing demyelinating disease. Although it is fre- netic resonance imaging of brain tumors. Neuro-
because the kurtosis values are less affected by quently used in brain MRI protocols, with its surg Clin N Am 2005; 16:115–134
the influence of crossing fibers. new applications, postprocessing techniques, 3. Cruz LC Jr, Sorensen AG. Diffusion tensor mag-
Another application for DKI in demyelinat- and future promises, DWI and other parame- netic resonance imaging of brain tumors. Magn
ing disease is the evaluation of normal-appear- ters will reveal many different aspects of de- Reson Imaging Clin N Am 2006; 14:183–202
ing gray matter (GM). Because GM has more myelinating disease. 4. Hygino da Cruz LC Jr, Vieira IG, Domingues RC.
free space for diffusion, measurement of frac- The most significant clinical application Diffusion MR imaging: an important tool in the
tional anisotropy is more difficult. Because of for DWI in demyelinating disease is to estab- assessment of brain tumors. Neuroimaging Clin N
this tissue property, evaluating the nongauss- lish a differential diagnosis with other abnor- Am 2011; 21:27–49
ian probability of diffusion could be a better malities, such as neoplasms, infectious dis- 5. Abou Zeid N, Pirko I, Erickson B, et al. Diffusion-
method to explain cortical diffusion [48]. eases, and ischemic lesions. Although there weighted imaging characteristics of biopsy-prov-
Our group (Doring TM, et al., presented at is no established diffusion pattern for demy- en demyelinating brain lesions. Neurology 2012;
2013 annual meeting of the Radiological Soci- elinating plaques, variable ADC patterns in 78:1655–1662
ety of North America) evaluated the benefits of a single MRI and rapid changes in such pat- 6. Balashov KE, Aung LL, Dhib-Jalbut S, Keller IA.
DKI in the assessment of patients with NMO. terns from previous reports are highly sug- Acute multiple sclerosis lesion: conversion of re-
Using an ROI-based analysis, DKI showed gestive of demyelinating disease. A second stricted diffusion due to vasogenic edema. J Neu-
sensitivity in detecting normal-appearing WM clinical application is related to the early di- roimaging 2011; 21:202–204
damage in two parameters, radial kurtosis and agnosis because restricted diffusion can be 7. Castriota Scanderbeg A, Tomaiuolo F, Sabatini U,
mean kurtosis. We found that radial kurtosis the first marker for a demyelinating lesion, Nocentini U, Grasso MG, Caltagirone C. Demye-
was significantly reduced (p < 0.05) in the cor- preceding contrast enhancement, associat- linating plaques in relapsing-remitting and second-
pus callosum and there was a tendency toward ed with subtle T2-weighted imaging altera- ary-progressive multiple sclerosis: assessment with
reduction in the right optic radiation (p < 0.1). tions. The third most significant DWI clini- diffusion MR imaging. AJNR 2000; 21:862–868
These same areas were evaluated by DTI pa- cal application is the ADC potential marker 8. Alexander AL, Lee JE, Lazar M, Field AS. Diffu-
rameters, and radial diffusivity was increased, for disease severity because restricted diffu- sion tensor imaging of the brain. Neurotherapeu-
corroborating the idea that radial kurtosis and sion is associated with a higher EDSS score tics 2007; 4:316–329
radial diffusivity strongly correlate negatively at the index attack. Moreover, ADC variation 9. Guo AC, MacFall JR, Provenzale JM. Multiple
(r = −0.797, Pearson correlation coefficient). from a homogeneously facilitated pattern to a sclerosis: diffusion tensor MR imaging for evalu-
The mean kurtosis was significantly increased dark-isointense ring pattern is correlated with ation of normal-appearing white matter. Radiolo-
in the right corticospinal tract (p = 0.004), but neurologic deterioration. DTI parameters gy 2002; 222:729–736
no alterations were found in the DTI param- contribute to the evaluation of normal-ap- 10. Smith SM, Jenkinson M, Johansen-Berg H, et al.
eters. This may reflect that DKI variations are pearing WM damage, which has previously Tract-based spatial statistics: voxelwise analysis
detected earlier than DTI variations. Thus, we only been investigated using histopatholog- of multi-subject diffusion data. Neuroimage
infer that in this preliminary study, DKI was ic intervention. An evolution from the ROI 2006; 31:1487–1505
more sensitive in depicting abnormalities in analysis to group analysis was performed by 11. Roosendaal SD, Geurts JJ, Vrenken H, et al. Re-
the normal-appearing brain parenchyma in de- TBSS. This group analysis of all major WM gional DTI differences in multiple sclerosis pa-
myelinating processes. tracts provides an overview of WM dam- tients. Neuroimage 2009; 44:1397–1403
age, including normal-appearing WM damage. 12. Tabesh A, Jensen JH, Ardekani BA, Helpern JA.
Other Techniques Thus, it is a robust way to investigate demye- Estimation of tensors and tensor-derived mea-
Continuous technical improvement is nec- linating disease in groups of patients. DKI is a sures in diffusional kurtosis imaging. Magn Re-
essary to solve the common problems already new technique that measures the nongaussian son Med 2011; 65:823–836
described in the previous topics. High-angu- behavior of diffusivity, which mostly occurs 13. Jensen JH, Helpern JA, Ramani A, Lu H, Kaczyn-
lar-resolution diffusion imaging acquisitions in the brain. It is more accurate than DTI pa- ski K. Diffusional kurtosis imaging: the quantifi-
collect DWI with many more gradient direc- rameters for evaluating fiber-crossing areas cation of non-gaussian water diffusion by means
AJR:202, January 2014 W41
Rueda-Lopes et al.
of magnetic resonance imaging. Magn Reson Med Mukherji SK, Maly P, Welsh R. Diffusion tensor 38. Dineen RA, Vilisaar J, Hlinka J, et al. Disconnec-
2005; 53:1432–1440 imaging of the brain: review of clinical applica- tion as a mechanism for cognitive dysfunction in
14. Filippi M, Iannucci G, Cercignani M, Rocca MA, tions. Neuroradiology 2004; 46:339–350 multiple sclerosis. Brain 2009; 132:239–249
Pratesi A, Comi G. A quantitative study of water 27. Andrade RE, Gasparetto EL, Cruz LC Jr, et al. 39. Bodini B, Cercignani M, Khaleeli Z, et al. Corpus
Downloaded from www.ajronline.org by KAGOSHIMA UNIVERSITY on 12/08/15 from IP address 163.209.223.17. Copyright ARRS. For personal use only; all rights reserved
diffusion in multiple sclerosis lesions and normal Evaluation of white matter in patients with multi- callosum damage predicts disability progression
appearing white matter using echo-planar imag- ple sclerosis through diffusion tensor magnetic and cognitive dysfunction in primary-progressive
ing. Arch Neurol 2000; 57:1017–1021 resonance imaging. Arq Neuropsiquiatr 2007; MS after five years. Hum Brain Mapp 2013;
15. Eisele P, Szabo K, Griebe M, et al. Reduced diffu- 65(3A):561–564 34:1163–1172
sion in a subset of acute MS lesions: a serial mul- 28. Rueda F, Hygino LC Jr, Domingues RC, Vascon- 40. Yu HJ, Christodoulou C, Bhise V, et al. Multiple
tiparametric MRI study. AJNR 2012; 33:1369– celos CC, Papais-Alvarenga RM, Gasparetto EL. white matter tract abnormalities underlie cogni-
1373 Diffusion tensor MR imaging evaluation of the tive impairment in RRMS. Neuroimage 2012;
16. Balasubramanya KS, Kovoor JM, Jayakumar PN, corpus callosum of patients with multiple sclero- 59:3713–3722
et al. Diffusion-weighted imaging and proton MR sis. Arq Neuropsiquiatr 2008; 66(3A):449–453 41. Giorgio A, Palace J, Johansen-Berg H, et al. Rela-
spectroscopy in the characterization of acute dis- 29. Yu CS, Zhu CZ, Li KC, et al. Relapsing neuromy- tionship of brain white matter microstructure with
seminated encephalomyelitis. Neuroradiology elitis optica and relapsing-remitting multiple scle- clinical and MR measures in relapsing-remitting
2007; 49:177–183 rosis: differentiation at diffusion-tensor MR im- multiple sclerosis. J Magn Reson Imaging 2010;
17. Hygino da Cruz LC Jr, Batista RR, Domingues aging of corpus callosum. Radiology 2007; 31:309–316
RC, Barkhof F. Diffusion magnetic resonance im- 244:249–256 42. Onu M, Roceanu A, Sboto-Frankenstein U, et al.
aging in multiple sclerosis. Neuroimaging Clin N 30. Cruz LC Jr, Domingues RC, Gasparetto EL. Dif- Diffusion abnormality maps in demyelinating dis-
Am 2011; 21:71–88 [vii-viii.] fusion tensor imaging of the cervical spinal cord ease: correlation with clinical scores. Eur J Radi-
18. Rovira A, Pericot I, Alonso J, et al. Serial diffu- of patients with relapsing-remising multiple scle- ol 2012; 81:e386–e391
sion-weighted MR imaging and proton MR spec- rosis: a study of 41 cases. Arq Neuropsiquiatr 43. Liu Y, Duan Y, He Y, et al. A tract-based diffusion
troscopy of acute large demyelinating brain le- 2009; 67(2B):391–395 study of cerebral white matter in neuromyelitis
sions: case report. AJNR 2002; 23:989–994 31. Pessoa FM, Lopes FC, Costa JV, Leon SV, optica reveals widespread pathological altera-
19. Melhem ER, Mori S, Mukundan G, et al. Diffu- Domingues RC, Gasparetto EL. The cervical spinal tions. Mult Scler 2012; 18:1013–1021
sion tensor imaging of the brain and white matter cord in neuromyelitis optica patients: a comparative 44. Helpern JA, Adisetiyo V, Falangola MF, et al. Pre-
tractography. AJR 2002; 178:3–16 study with multiple sclerosis using diffusion tensor liminary evidence of altered gray and white mat-
20. Schmierer K, Wheeler-Kingshott CA, Boulby PA, et imaging. Eur J Radiol 2012; 81: 2697–2701 ter microstructural development in the frontal
al. Diffusion tensor imaging of post mortem multiple 32. Rueda Lopes FC, Doring T, Martins C, et al. The lobe of adolescents with attention-deficit hyperac-
sclerosis brain. Neuroimage 2007; 35:467–477 role of demyelination in neuromyelitis optica tivity disorder: a diffusional kurtosis imaging
21. Song SK, Sun SW, Ramsbottom MJ, Chang C, Rus- damage: diffusion-tensor MR imaging study. Ra- study. J Magn Reson Imaging 2011; 33:17–23
sell J, Cross AH. Dysmyelination revealed through diology 2012; 263:235–242 45. Lu H, Jensen JH, Ramani A, Helpern JA. Three-
MRI as increased radial (but unchanged axial) diffu- 33. Blaschek A, Keeser D, Müller S, et al. Early white dimensional characterization of non-gaussian wa-
sion of water. Neuroimage 2002; 17:1429–1436 matter changes in childhood multiple sclerosis: a ter diffusion in humans using diffusion kurtosis
22. Tievsky AL, Ptak T, Farkas J. Investigation of ap- diffusion tensor imaging study. AJNR [Epub 2013 imaging. NMR Biomed 2006; 19:236–247
parent diffusion coefficient and diffusion tensor May 6] 46. Cheung MM, Hui ES, Chan KC, Helpern JA, Qi L,
anisotropy in acute and chronic multiple sclerosis 34. Aliotta R, Cox JL, Donohue K, et al. Tract-based Wu EX. Does diffusion kurtosis imaging lead to
lesions. AJNR 1999; 20:1491–1499 spatial statistics analysis of diffusion-tensor im- better neural tissue characterization? A rodent brain
23. Werring DJ, Clark CA, Barker GJ, et al. Diffusion aging data in pediatric- and adult-onset multiple maturation study. Neuroimage 2009; 45:386–392
tensor imaging of lesions and normal-appearing sclerosis. Hum Brain Mapp [Epub 2012 Aug 30] 47. Lazar M, Jensen JH, Xuan L, Helpern JA. Estima-
white matter in multiple sclerosis. Neurology 35. Raz E, Cercignani M, Sbardella E, et al. Clinically tion of the orientation distribution function from
1999; 52:1626–1632 isolated syndrome suggestive of multiple sclerosis: diffusional kurtosis imaging. Magn Reson Med
24. Kealey SM, Kim YJ, Whiting WL, Madden DJ, voxelwise regional investigation of white and gray 2008; 60:774–781
Provenzale JM. Determination of multiple sclero- matter. Radiology 2010; 254:227–234 48. Hori M, Fukunaga I, Masutani Y, et al. Visualizing
sis plaque size with diffusion-tensor MR imaging: 36. Roosendaal SD, Schoonheim MM, Hulst HE, et non-gaussian diffusion: clinical application of q-
comparison study with healthy volunteers. Radi- al. Resting state networks change in clinically iso- space imaging and diffusional kurtosis of the brain
ology 2005; 236:615–620 lated syndrome. Brain 2010; 133:1612–1621 and spine. Magn Reson Med Sci 2012; 11:221–233
25. Sundgren PC. Diffusion tensor imaging of the 37. Raz E, Cercignani M, Sbardella E, et al. Gray- 49. Nagy Z, Alexander DC, Thomas DL, Weiskopf N,
brain: background and review of clinical applica- and white-matter changes 1 year after first clinical Sereno ML. Using high angular resolution imag-
tions. Imaging Decisions 2005; 1:2–15 episode of multiple sclerosis: MR imaging. Radi- ing data to discriminate cortical regions. PLoS
26. Sundgren PC, Dong Q. Gomez-Hassan D, ology 2010; 257:448–454 ONE 2013; 8:e63842
W42 AJR:202, January 2014
You might also like
- Schema Therapy For Dissociative Identity Disorder (DID) Rationale and StudyDocument12 pagesSchema Therapy For Dissociative Identity Disorder (DID) Rationale and StudyprematellieNo ratings yet
- Nursing Care of CHF (Congestive Heart Failure)Document25 pagesNursing Care of CHF (Congestive Heart Failure)Irwan100% (2)
- Advanced Hemodynamic Monitoring: Basics and New Horizons: Mikhail Y. Kirov Vsevolod V. Kuzkov Bernd SaugelDocument289 pagesAdvanced Hemodynamic Monitoring: Basics and New Horizons: Mikhail Y. Kirov Vsevolod V. Kuzkov Bernd SaugelIda Katarina75% (4)
- Scale For Ranking Health Conditions and Problems According To PrioritiesDocument9 pagesScale For Ranking Health Conditions and Problems According To Prioritiescnvfiguracion100% (1)
- Pressure Ulcer Assessment Chart & Body MapDocument2 pagesPressure Ulcer Assessment Chart & Body MapWidfdsafdsaNo ratings yet
- Diagnosis, Differential Diagnosis, And.5Document25 pagesDiagnosis, Differential Diagnosis, And.5Rahul RaiNo ratings yet
- Chronic Limb Ischaemia: MR Hanif Hussein Consultant Vascular Surgeon, HKLDocument35 pagesChronic Limb Ischaemia: MR Hanif Hussein Consultant Vascular Surgeon, HKLZulzaire ZulkefliNo ratings yet
- Malabsorption SyndromeDocument7 pagesMalabsorption SyndromeHassan.shehri100% (4)
- Regional AnesDocument36 pagesRegional AnesMay Anne BuenafeNo ratings yet
- Trombosis Imagenes Fuente de ErrorDocument9 pagesTrombosis Imagenes Fuente de ErrorHumbertoHurtadoNo ratings yet
- Diffusion-Weighted MR Imaging in Brain TumorDocument9 pagesDiffusion-Weighted MR Imaging in Brain TumorZe PushNo ratings yet
- Boosted Cascaded Convnets For Multilabel Classification of Thoracic Diseases in Chest RadiographsDocument5 pagesBoosted Cascaded Convnets For Multilabel Classification of Thoracic Diseases in Chest RadiographsDeepti SinghNo ratings yet
- A Genetic Cause of Alzheimer Disease Source Nat Rev Neurosci So 2015 Sep 16 9 564 74 (PMIDT26243569)Document11 pagesA Genetic Cause of Alzheimer Disease Source Nat Rev Neurosci So 2015 Sep 16 9 564 74 (PMIDT26243569)dai shujuanNo ratings yet
- Radiographic Evaluation of Scoliosis 2010 MalfairDocument15 pagesRadiographic Evaluation of Scoliosis 2010 Malfairfebyan yohanesNo ratings yet
- Artificial Intelligence in Diabetic Eye Disease ScreeningDocument7 pagesArtificial Intelligence in Diabetic Eye Disease Screeningmarlon GarcíaNo ratings yet
- CT Scan PDFDocument12 pagesCT Scan PDFBunga alaraafNo ratings yet
- Diagnosis of Diabetic Retinopathy Using Deep Neural NetworksDocument11 pagesDiagnosis of Diabetic Retinopathy Using Deep Neural NetworksFahad RazaNo ratings yet
- Adult GliomasDocument24 pagesAdult GliomasSofía UrbinaNo ratings yet
- Transplantology 02 00011Document9 pagesTransplantology 02 00011giant nitaNo ratings yet
- Meiryndra Syaira Putri, Farina Pramanik, Lusi EpsilawatiDocument5 pagesMeiryndra Syaira Putri, Farina Pramanik, Lusi EpsilawatinadiaNo ratings yet
- MRI of Tuberculous TBDocument4 pagesMRI of Tuberculous TBZehna NzNo ratings yet
- Depression in Dialysis: ReviewDocument13 pagesDepression in Dialysis: ReviewDoc RuthNo ratings yet
- D-Dimer Tests in The Emergency Department: Current Insights: Open Access Emergency Medicine DoveDocument15 pagesD-Dimer Tests in The Emergency Department: Current Insights: Open Access Emergency Medicine Doveucdavisma713No ratings yet
- Locating The Fovea Center Position in Digital Fundus Images Using Thresholding and Feature Extraction TechniquesDocument8 pagesLocating The Fovea Center Position in Digital Fundus Images Using Thresholding and Feature Extraction TechniquesMitcheel Lanas SozaNo ratings yet
- Management of Acute and Traumatic Wounds With.8-2Document11 pagesManagement of Acute and Traumatic Wounds With.8-2GRAÇA ISABEL MATOS SIMÕESNo ratings yet
- Advanced MRI in Pediatric Brain TM Lequin2017Document24 pagesAdvanced MRI in Pediatric Brain TM Lequin2017jesusgonzalezapNo ratings yet
- Sensors: Diabetic Retinopathy Fundus Image Classification and Lesions Localization System Using Deep LearningDocument22 pagesSensors: Diabetic Retinopathy Fundus Image Classification and Lesions Localization System Using Deep LearningAdnan KhanNo ratings yet
- Detection of Severity Level of Diabetic Retinopathy Using Bag of Features ModelDocument8 pagesDetection of Severity Level of Diabetic Retinopathy Using Bag of Features ModelaaNo ratings yet
- Diabetic Retinopathy Detection Using MatlabDocument7 pagesDiabetic Retinopathy Detection Using MatlabMani Narayana K TNo ratings yet
- JCM 12 00385Document12 pagesJCM 12 00385Anugerah Galang PersadaNo ratings yet
- JCM 12 00453Document15 pagesJCM 12 00453AndreiMunteanuNo ratings yet
- A Deep Learning Ensemble Approach For Diabetic RetDocument10 pagesA Deep Learning Ensemble Approach For Diabetic RetMuhammad Junaid AliNo ratings yet
- Classification of Diabetic Maculopathy Based On Optical Coherence Tomography Images Using A Vision Transformer Model Bmjophth-2023-001423Document8 pagesClassification of Diabetic Maculopathy Based On Optical Coherence Tomography Images Using A Vision Transformer Model Bmjophth-2023-001423MarioNo ratings yet
- Artificial Intelligence and Deep Learning in OphthalmologyDocument9 pagesArtificial Intelligence and Deep Learning in OphthalmologySilvia Rossa MuisNo ratings yet
- 2019 IEEE TMI CANet Cross-Disease Attention Network For Joint Diabetic Retinopathy and Diabetic Macular Edema GradingDocument11 pages2019 IEEE TMI CANet Cross-Disease Attention Network For Joint Diabetic Retinopathy and Diabetic Macular Edema GradingTushirNo ratings yet
- Automated Classification of Diabetic Retinopathy Through Reliable Feature SelectionDocument19 pagesAutomated Classification of Diabetic Retinopathy Through Reliable Feature SelectionSangeethaNo ratings yet
- Indiana University Foundation DermatogramDocument3 pagesIndiana University Foundation DermatogramGenji AyyahNo ratings yet
- Gihepjune22lowres DigitalDocument30 pagesGihepjune22lowres DigitalMohamed AtefNo ratings yet
- Wayfinding For People With Dementia - A Review of The Role of Architectural DesignDocument17 pagesWayfinding For People With Dementia - A Review of The Role of Architectural Design梁婉莹No ratings yet
- Peripheral Nerve.10Document27 pagesPeripheral Nerve.10Novanda RizkyNo ratings yet
- Jurnal CR ImageDocument7 pagesJurnal CR ImageEsa AldiNo ratings yet
- Prognostic Value of Intermediate Age-Related Macular Degeneration Phenotypes For Geographic Atrophy ProgressionDocument7 pagesPrognostic Value of Intermediate Age-Related Macular Degeneration Phenotypes For Geographic Atrophy ProgressionqisthiNo ratings yet
- Dayananda Sagar University: Department of Computer Science and Engineering Machine Learning Mini ProjectDocument12 pagesDayananda Sagar University: Department of Computer Science and Engineering Machine Learning Mini Projectmanoj998620No ratings yet
- Enhancing Ocular Healthcare Deep Learning-Based Multi-Class Diabetic Eye Disease Segmentation and ClassificationDocument18 pagesEnhancing Ocular Healthcare Deep Learning-Based Multi-Class Diabetic Eye Disease Segmentation and Classificationyt HehkkeNo ratings yet
- Current Clinical Brain Tumor Imaging: Neuroradiology Review SeriesDocument19 pagesCurrent Clinical Brain Tumor Imaging: Neuroradiology Review Seriesalih jenjang2021No ratings yet
- Spie2013 DownDocument8 pagesSpie2013 Downnegri negriNo ratings yet
- 21 Ijisae SKM MJ PC AaDocument7 pages21 Ijisae SKM MJ PC AaSandeep MathariyaNo ratings yet
- Jurding RadioDocument11 pagesJurding RadioMutiara Sri WidyastutiNo ratings yet
- Ghribi 2014Document5 pagesGhribi 2014Ines NjehNo ratings yet
- Morales 2015Document8 pagesMorales 2015José Micael Delgado BarbosaNo ratings yet
- Diabetic Retinopathy Classification Using Deep Learning Techniques To Enhance The Finding Using Color Neutralization TechniquesDocument6 pagesDiabetic Retinopathy Classification Using Deep Learning Techniques To Enhance The Finding Using Color Neutralization TechniquesgauravchauNo ratings yet
- (IJCST-V7I2P21) :C.Sunitha RamDocument8 pages(IJCST-V7I2P21) :C.Sunitha RamEighthSenseGroupNo ratings yet
- 9 Enfermedades Desmielinizantes II PDFDocument20 pages9 Enfermedades Desmielinizantes II PDFRodrigoMendozaNo ratings yet
- Aging Changes of The Midfacial Fat Compartments A.45Document11 pagesAging Changes of The Midfacial Fat Compartments A.45Juliana BrunettoNo ratings yet
- 068 - Wound Central - 2021 - 5!4!336 - Jose Contreras-Ruiz 19 150921 LsDocument4 pages068 - Wound Central - 2021 - 5!4!336 - Jose Contreras-Ruiz 19 150921 LsAnonymous 1nMTZWmzNo ratings yet
- How Can Students Diagnostic Competence Benefit.32Document7 pagesHow Can Students Diagnostic Competence Benefit.32Carlos Roberto Pires de Oliveira LimaNo ratings yet
- Research Article: Ensemble Framework of Deep Cnns For Diabetic Retinopathy DetectionDocument11 pagesResearch Article: Ensemble Framework of Deep Cnns For Diabetic Retinopathy Detectionasma khanNo ratings yet
- 1 s2.0 S1877050918308068 MainDocument9 pages1 s2.0 S1877050918308068 MainRaksheet JainNo ratings yet
- Using Neural Networks For Differential Diagnosis of Alzheimer Disease and Vascular DementiaDocument7 pagesUsing Neural Networks For Differential Diagnosis of Alzheimer Disease and Vascular DementiaDiego MedinaNo ratings yet
- Ajr 12 8629Document12 pagesAjr 12 8629YAŞAR TÜRKNo ratings yet
- RG 2019180055Document23 pagesRG 2019180055drgaganwahi1971No ratings yet
- Two Year Visual Outcomes After Photodynamic.9Document6 pagesTwo Year Visual Outcomes After Photodynamic.9maleticjNo ratings yet
- Imaging of Traumatic Brain Injury: A Review of The Recent Medical LiteratureDocument4 pagesImaging of Traumatic Brain Injury: A Review of The Recent Medical LiteratureasfwegereNo ratings yet
- Tugas Telaah Jurnal Fetal DistressDocument2 pagesTugas Telaah Jurnal Fetal Distressdwii purwatiiNo ratings yet
- Evaluation of Facial Nerve Function Following Preauricular and Submandibular Approaches by Using The Housebrackmann FaciDocument7 pagesEvaluation of Facial Nerve Function Following Preauricular and Submandibular Approaches by Using The Housebrackmann FaciMohammedNo ratings yet
- State of the Art Techniques in Critical Care Echocardiography: 3D, Tissue, ContrastFrom EverandState of the Art Techniques in Critical Care Echocardiography: 3D, Tissue, ContrastKonstantin YastrebovNo ratings yet
- "The Effects of Interpersonal Crime On Victims": Reporter: Michel O. Espinosa Bs-Psychology Code: 3175Document6 pages"The Effects of Interpersonal Crime On Victims": Reporter: Michel O. Espinosa Bs-Psychology Code: 3175Ezri Mariveles Coda Jr.No ratings yet
- The Sketch of Indonesia Medicine: Sugma AP, MD, MARSDocument42 pagesThe Sketch of Indonesia Medicine: Sugma AP, MD, MARSRaja Friska YulandaNo ratings yet
- CBD Spinal Infection: by Neoh Zhong NingDocument26 pagesCBD Spinal Infection: by Neoh Zhong NingJoni NeohNo ratings yet
- ISMP Voluume 15 No 10 Oct 2017-NurseAdviseERR201710Document4 pagesISMP Voluume 15 No 10 Oct 2017-NurseAdviseERR201710uss uusNo ratings yet
- SWAN Parkinson MRIDocument9 pagesSWAN Parkinson MRIulfi yunitaNo ratings yet
- DrainsDocument19 pagesDrainspaulineNo ratings yet
- Cost Per Test PC400 2020Document10 pagesCost Per Test PC400 2020fischaNo ratings yet
- Endocrine PancreasDocument21 pagesEndocrine Pancreaslacafey741No ratings yet
- 2014 @nucproflib Helen Ryder, GiorgioDocument128 pages2014 @nucproflib Helen Ryder, Giorgioe'Rfan k'AguyaNo ratings yet
- Fitzpatricks Dermatology in General Medicine 8ed 1Document10 pagesFitzpatricks Dermatology in General Medicine 8ed 1ANTINNo ratings yet
- Emergency Viva (Full)Document48 pagesEmergency Viva (Full)ashokarathnasingheNo ratings yet
- File, 14991, enDocument20 pagesFile, 14991, enAdimNo ratings yet
- 2 Bachelor of Optometry (B Optom) 1Document7 pages2 Bachelor of Optometry (B Optom) 1Rehana ThapaNo ratings yet
- Re-Test SUBJECT-English Core Class - Xi Time: 2 Hrs. M.M: 50 General InstructionsDocument8 pagesRe-Test SUBJECT-English Core Class - Xi Time: 2 Hrs. M.M: 50 General InstructionsSunilDwivediNo ratings yet
- Evaluasi Usg Dan Tatalaksana Pada Varises Vena Tungkai - DR RamziDocument31 pagesEvaluasi Usg Dan Tatalaksana Pada Varises Vena Tungkai - DR RamziMohamad ZulfikarNo ratings yet
- Patient Case PresentationDocument7 pagesPatient Case Presentationapi-613861196No ratings yet
- Acne Keloidalis NuchaeDocument16 pagesAcne Keloidalis NuchaejalalfaizNo ratings yet
- 683 2Document15 pages683 2M Noaman AkbarNo ratings yet
- Women The Skilled Architect of The SocietyDocument4 pagesWomen The Skilled Architect of The SocietyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Antimicrobial Effect of Aqueous Banana Peel Extract, IraqDocument4 pagesAntimicrobial Effect of Aqueous Banana Peel Extract, IraqLilis KhusnulNo ratings yet
- Test Bank For Health Psychology 7th Edition TaylorDocument21 pagesTest Bank For Health Psychology 7th Edition Taylorwoodwardpunction2vq46zNo ratings yet
- Chemical Toxicity Summit Day 6Document5 pagesChemical Toxicity Summit Day 6Paul Ioan PopescuNo ratings yet
- First Aid Maxilofacl SurgeryDocument94 pagesFirst Aid Maxilofacl SurgerydoctorniravNo ratings yet