Professional Documents
Culture Documents
Improving Bedside Teaching Findings From A Focus.9
Uploaded by
claimstudent3515Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Improving Bedside Teaching Findings From A Focus.9
Uploaded by
claimstudent3515Copyright:
Available Formats
Clinical Teaching
Improving Bedside Teaching: Findings from a
Focus Group Study of Learners
Keith N. Williams, MD, MSME, EdM, Subha Ramani, MBBS, MMEd, MPH,
Bruce Fraser, PhD, and Jay D. Orlander, MD, MPH
Abstract
Purpose conducted between June 2004 and autonomy, and incorporating them
Literature reviews indicate that the February 2005. Each 60- to 90-minute into the teaching process; faculty
proportion of clinical educational time discussion was audiotaped, transcribed, development; and advocating evidence-
devoted to bedside teaching ranges from and analyzed using qualitative based physical diagnosis. Students
8% to 19%. Previous studies regarding methods. focused on the physical diagnosis aspects
this paucity have not adequately of bedside teaching, whereas views of
examined the perspectives of learners. Results
residents reflected their multifaceted
The authors explored learners’ attitudes Learners believed that bedside teaching
roles as learners, teachers, and
toward bedside teaching, perceptions of is valuable for learning essential clinical
skills. They believed it is underutilized managers.
barriers, and strategies to increase
its frequency and effectiveness, as well as and described many barriers to its use:
whether learners’ stages of training lack of respect for the patient; time Conclusions
influenced their perspectives. constraints; learner autonomy; faculty Bedside teaching is valuable but
attitude, knowledge, and skill; and underutilized. Including the patient,
Method overreliance on technology. Learners collaborating with learners, faculty
Six focus group discussions with fourth- suggested a variety of strategies to development, and promoting a
year medical students and first- or mitigate barriers: orienting and including supportive institutional culture can
second-year internal medicine residents the patient; addressing time constraints redress several barriers to bedside
recruited from the Boston University through flexibility, selectivity, and teaching.
School of Medicine and Residency integration with work; providing learners
Program in Internal Medicine were with reassurance, reinforcing their Acad Med. 2008; 83:257–264.
There is a general uneasiness both in the effectiveness of bedside teaching, many to explore learners’ attitudes toward
minds of the public and also in the medical educators espouse its value in bedside teaching, perceptions of barriers,
practicing physician, that future
training physicians.1–17 It seems logical and strategies to increase its frequency
specialists in internal medicine will
become mostly reliant on laboratory, to assume that clinical skills related to and effectiveness. We included learners
computerized, nonpersonal techniques of physician–patient communication, at different stages of training to assess
management, and the patient as a human physical examination, clinical reasoning, whether experience influenced perspective.
being with emotional and psychological and professionalism are better learned
aspects will be forgotten. If such at the bedside than in a classroom.
physicians are to come into being, it must Method
Nevertheless, the proportion of clinical
be due to the kind of training and With the exception of the principal
environment to which they are exposed in
educational time devoted to bedside
teaching has ranged from 8% to 19% investigator (K.W.), all coinvestigators
their years in medical school.
since the 1960s.18 –23 Although medical had qualitative research experience
—L.H. Nahum educators have speculated on the reasons before the conduct of this study, and
Bedside teaching, clinical teaching for this paucity, few studies have
examined the issue systematically.
one (B.F.) taught a graduate course on
qualitative research. We conducted six
done in the presence of a patient, has Existing studies have had a limited scope focus group discussions between June
been a fundamental component of or have explored bedside teaching only 2004 and February 2005 with students
medical training in the United States from the perspective of teachers.24 –28 from the Boston University School of
since the institution of modern methods Although numerous guidelines Medicine and residents from the Boston
of instruction in the late 19th century. advocating specific bedside teaching University Residency Program in Internal
Although few data exist regarding the strategies have been published, it is Medicine. All prospective participants
unclear whether the perspectives of learners received an e-mail letter of invitation.
influenced their development.29 – 42 Participation was voluntary and
Please see the end of this article for information confidential, and verbal consent was
about the authors. Learners are likely to have unique obtained from all participants. We
Correspondence should be addressed to Dr. and valuable perspectives on bedside audiotaped discussions and transcribed
Williams, c/o Dr. Ramani, Boston University School of
teaching; any effort to increase or them verbatim. The institutional review
Medicine, 715 Albany St., Vose 320, Boston, MA
02118; telephone: (617) 638-7985; fax: (617) 638- improve bedside teaching should board of the Boston University Medical
7905; e-mail: (Keith.Williams@bmc.org). consider their views. Our objectives were Center approved the research protocol.
Academic Medicine, Vol. 83, No. 3 / March 2008 257
Clinical Teaching
We sought varied perspectives by Results
recruiting participants at different Thirty-three students and residents List 1
stages of training. Groups one and two participated in one of six focus group Knowledge and skills learned with
consisted of fourth-year students. Groups bedside teaching
discussions (Table 1). All residents had
three and five consisted of “first-year” attended medical school in the United • Obtaining a medical history
internal medicine (IM) residents, and States or Canada. Coded passages • Performing a physical examination
groups four and six of consisted of generated several categories: value of • Generating a differential diagnosis
“second-year” IM residents; by definition, bedside teaching, quantity and quality of • Formulating a management plan
the former had completed one year of bedside teaching, barriers to bedside
postgraduate study, and the latter had • Applying clinical reasoning
teaching, and strategies to increase and
completed two. • Communicating effectively
improve bedside teaching. Differences
between students’ and residents’ views • Exhibiting professional bedside demeanor
We defined bedside teaching as clinical were apparent and reflected differences in • Demonstrating empathy
teaching in the presence of a patient. We their roles. When applicable, we have • Performing diagnostic and therapeutic
constructed open-ended questions to noted the level of learner. Statements procedures
explore learners’ experiences and represent the views of learners and not • Acquiring knowledge about medical
opinions regarding bedside teaching. We instrumentation
the authors.
asked whether they learned from bedside
teaching and, if so, what they had Value of bedside teaching
learned. We asked about the quality and Quantity and quality of bedside
Learners believed bedside teaching is teaching
quantity of bedside teaching they
valuable, if not essential, for learning
received. Finally, we solicited their views Learners stated that bedside teaching is
skills relating to physician–patient
on barriers to bedside teaching and underutilized and that there are missed
communication, physical examination,
suggestions on strategies to increase its opportunities for bedside teaching. They
clinical reasoning, and professionalism
frequency and effectiveness. The reported that the quantity and quality of
(List 1). They reported that observing the
interviewer (K.W.) pursued relevant bedside teaching vary greatly among
resident or attending physician interact
themes and sought clarification or faculty and, for students, between
with patients is often instructive. Learners
elaboration as required. Participants had clerkships. Students noted the most
indicated that patients also benefit from
ample opportunity to express unsolicited bedside teaching during their IM
bedside teaching encounters, and they
opinions. clerkships, but even there, quantity and
emphasized that discussions of topics not
quality vary.
directly related to patient care are more
Focus group discussions were 60 to 90 appropriately taught elsewhere. We do [bedside teaching] rarely because I
minutes in duration. The principal feel like when it happens it stands out so
investigator (K.W.) conducted all It’s very powerful if you see the example much. (Second-year IM resident)
interviews and, using standard qualitative on an actual person, and especially if you
methods, coded the transcripts.43 We know more about their story, their Barriers to bedside teaching
grouped coded passages into major background, you’re more likely to take Viewing bedside teaching as the interplay
something away from that experience,
categories and identified prominent of patient, teacher, and learner in the
whether it be some kernel of knowledge
themes that emerged. We also identified about a disease or a certain way of context of the learning environment,
contrasting responses across the interacting with patients. (Fourth-year barriers were classified as personal,
experience levels of participants. medical student) interpersonal, or environmental (Table 2).
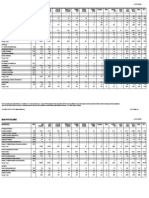
Table 1
Characteristics of 33 Volunteer Participants in Six Focus Groups on Bedside
Teaching, Boston University (BU) School of Medicine and BU Residency Program
in Internal Medicine, 2004 –2005
Students’ Residents’ specialty
Age of participants specialty plans plans
Group Type Men Women 20–25 26–30 31–35 Medicine Surgery Other Yes No Maybe
1 Fourth-year 3 3 5 1 0 1 2 3 NA NA NA
student
...................................................................................................................................................................................................................................................................................................................
2 Fourth-year 4 1 3 2 0 2 1 2 NA NA NA
student
...................................................................................................................................................................................................................................................................................................................
3 First-year resident 5 2 0 5 2 NA NA NA 5 0 2
...................................................................................................................................................................................................................................................................................................................
4 Second-year 3 2 0 2 3 NA NA NA 5 0 0
resident
...................................................................................................................................................................................................................................................................................................................
5 First-year resident 3 3 1 4 1 NA NA NA 5 0 1
...................................................................................................................................................................................................................................................................................................................
6 Second-year 3 1 0 3 1 NA NA NA 2 2 0
resident
258 Academic Medicine, Vol. 83, No. 3 / March 2008
Clinical Teaching
Table 2
Barriers to Bedside Teaching, and Strategies to Increase and Improve Bedside
Teaching, Compiled from Six Focus Groups on Bedside Teaching, Boston
University (BU) School of Medicine and BU Residency Program in Internal
Medicine, 2004 –2005
Category Barrier Strategy
Personal Low initiative for teaching Increase teaching initiative with institutional incentives
...................................................................................................................................................................................................................................................................
Low teacher/learner expectations for teaching Increase teacher/learner expectations with:
• Explicit teaching expectations for teachers
• Explicit learning objectives for students and residents
...................................................................................................................................................................................................................................................................
Inadequate bedside teaching skills Develop teaching skills through faculty development and
resident training initiatives
• Create a supportive learning environment (e.g.,
admission by teachers of own limitations/errors)
• Acknowledge learners’ needs
• Plan teaching in a flexible manner to accommodate work
schedules
• Selectively and efficiently integrate teaching with work
• Set time limits when teaching
...................................................................................................................................................................................................................................................................
Inadequate clinical knowledge and/or skills (faculty) Improve clinical knowledge and/or skills through faculty
development initiatives (e.g., advanced training in evidence-
based physical diagnosis)
Interpersonal Lack of patient cooperation • Request permission from the patient
• Orient the patient to the dual purpose of the bedside
session (i.e., patient care and teaching)
• Include the patient in discussions and answer questions
• Inform the patient about his/her care (i.e., patient
education)
...................................................................................................................................................................................................................................................................
Learners’ desire for autonomy in patient care/fear of a • Respect the learner–patient relationship
compromised relationship with the patient • Negotiate an appropriate level of autonomy with learners
• Create a supportive learning environment
• Share teaching responsibility with team members
...................................................................................................................................................................................................................................................................
Learner/patient fear of embarrassment/humiliation Learner
• Create a supportive learning environment
Patient
• Request permission from and orient the patient
• Include and inform the patient
Environmental Lack of time attributable to high patient volume and turnover • Reduce service caps on the number of patients admitted
and/or managed
• Create nonteaching services for patient overflow
...................................................................................................................................................................................................................................................................
Competing responsibilities of faculty Reduce or eliminate competing demands on faculty such as
outpatient clinical duties and research responsibilities
...................................................................................................................................................................................................................................................................
Deficient institutional expectations/incentives for teaching Increase institutional expectations/incentives for teaching
with:
• Explicit teaching expectations/incentives for
faculty/residents
• Explicit learning objectives for residents/students
...................................................................................................................................................................................................................................................................
Inadequate institutional recognition of teaching Enhance institutional recognition of teaching with
legitimate rewards for excellence in teaching
...................................................................................................................................................................................................................................................................
Devaluation of clinical skills by technology Emphasize evidence-based clinical diagnosis through faculty
development and resident training initiatives
...................................................................................................................................................................................................................................................................
Interruptions during rounds No strategy offered
...................................................................................................................................................................................................................................................................
Lack of privacy in multipatient room No strategy offered
...................................................................................................................................................................................................................................................................
Lack of space within patient room No strategy offered
...................................................................................................................................................................................................................................................................
Excessive noise No strategy offered
Personal barriers are factors attributable the learning institution as well as Lack of respect for the patient. Learners
to individuals, whereas interpersonal structural and functional aspects of the expressed concern for patients’ welfare
barriers represent aspects of the patient-care environment. Several and recognized that their own education
relationship between at least two overarching themes emerged from the is secondary to patient care. Bedside
individuals. Environmental barriers data: lack of respect for the patient; time discussion of sensitive issues, such as
denote contextual factors that influence constraints; learner autonomy; faculty substance abuse, mental health, and
bedside teaching. The learning attitude, knowledge, and skill; and sexuality-related topics, could embarrass
environment includes cultural aspects of overreliance on technology. the patient and result in the elicitation of
Academic Medicine, Vol. 83, No. 3 / March 2008 259
Clinical Teaching
inaccurate information. Discussion of bedside demonstration of deficiencies So much of medicine now with radiology
diagnostic possibilities could cause undue causes patients to lose confidence in the studies and blood tests is so algorithm
driven that a lot of this other stuff doesn’t
alarm, particularly conversations about learner as clinician, or in the advanced
matter anymore. I know what the plan’s
fatal diseases such as cancer. Bedside resident as team leader. They also feared going to be before I see the patient. A lot
deliberation of management plans that their attendings would usurp their of bedside teaching is gone away because
could lead patients to lose confidence authority to manage the team. Although of that. (First-year IM resident)
in the medical team if they witnessed many learners voiced discomfort at
disagreements. Learners attested that admitting “I don’t know” to their One intern used to call the CT scanner
patients are rarely asked permission or patients, some accepted the necessity, if the “doughnut of truth.” It’s kind of
oriented to bedside teaching. Most not inevitability, of making such an revealing. It’s like saying that you don’t
need to lay your hands on the patient, just
concerning to learners are situations in admission. Some believed that lack of plop them down on the thing. (Second-
which the patient is marginalized during harmonious team dynamics contributes year IM resident)
a bedside discussion, as manifested by a to these difficulties.
clinician’s failure to seek patient input, However, many learners believed that, in
explain medical terminology, or answer It is uncomfortable when you’re the
resident and the patient knows that
spite of technology, patients still expect
questions. dialogue with and examination by their
you’re the one that’s there all the time
and somebody’s going through this physicians and are disappointed and
I’ve seen attendings or residents exclude
the patient when they’re bedside teaching, lengthy teaching episode with you, indignant when clinical interactions are
and patients find that really offensive because I feel they want to be comforted inadequate. Some learners desired
because it’s their body, it’s their story, and by the fact that you know something, international medical experiences where
they’re marginalized while they’re being which you do, but there’s that line where
they could obtain traditional clinical
used for teaching, whereas if the patient’s it can be uncomfortable. (First-year IM
resident) teaching in the absence of the influence
included then it’s great for everybody and
of technology.
it’s a really effective learning tool. (First-
year IM resident) Ironically, some residents believed that
I don’t think we’ll ever get away from the
attendings sometimes allow excessive
physical exam. Even if you don’t have to
Time constraints. Most learners believed autonomy. In such circumstances, all listen to their lungs and learn anything,
that time constraints significantly limit teaching suffers, not just that performed the patients feel so much more of a
bedside teaching. Contributing to this at the bedside. connection to you when you do. It’s more
perception are a high resident workload than just learning the physical exam. It’s
and the observation that attendings We crave autonomy, but it’s a balance. learning patient interaction, too. (First-
often maintain significant ambulatory, I’m at the point now where I don’t want year IM resident)
as much autonomy, I actually want to
administrative, or research responsibilities
interact more with my attendings. I had
during their ward service, thus reducing an attending this past month who gave Strategies to increase and improve
time for learner interaction and bedside me too much autonomy. It was fun, it bedside teaching
teaching. Learners preferred to avoid was easier, but I didn’t learn much. Learners provided many insightful
extended teaching encounters when (Second-year IM resident)
recommendations to increase and
overwhelmed by workload or fatigue. improve bedside teaching (Table 2).
Faculty attitudes, knowledge, and skill. Strategies addressing the barrier themes
You duck out and you’re not involved in
Learners believed that all attendings have noted previously are discussed below.
the actual teaching at the bedside because
you need the computer and the phone in something to teach at the bedside. There
the hallway to get things done so that was speculation that the reluctance of Orient and include the patient. Although
things are happening earlier in the day attendings to engage in bedside teaching patients were rarely described as
and you’re not discharging someone at six derives more from lack of teaching skill uncooperative, learners emphasized the
in the afternoon. (First-year IM resident) than lack of clinical competence. need to orient patients and request
permission before teaching. Explaining
Interestingly, some learners questioned I definitely ran into some people where
the purpose of a bedside teaching
why bedside teaching should take more I’d ask them questions and I could tell
that I was making them uncomfortable, encounter and requesting permission to
time than that required for teaching in
even though they had lots to offer me. observe or examine were identified as
other settings. Such speculation led them
That was what was really strange; they important signs of respect that foster
to conclude that there is not so much a didn’t realize that I’m asking at such a trust and cooperation.
lack of time for bedside teaching, but for basic level that they have lots to teach me.
all teaching. (Fourth-year medical student) The most important thing is being able to
develop a rapport with your patients, and
Theoretically, bedside teaching shouldn’t Overreliance on technology. Given the making them feel like you’re not forcing
take any longer. What we’re actually
ever-increasing technological options for something on them, where it’s a
saying is there’s not enough time for
teaching in general, rather than for diagnosis and treatment, some learners comfortable environment. If an attending
questioned the role and importance of or resident has the ability to establish a
bedside teaching. (First-year IM resident)
proficiency in bedside diagnostic skills relationship with the patient that’s
reasonable, you can get a lot more out of
Learner autonomy. Advanced residents if further testing is done regardless of that situation because the patient is more
expressed concern that bedside teaching clinical impression. This loss of faith in willing to participate and the students will
compromises the relationship between traditional skills led to speculation about feel more comfortable in that setting, too.
learner and patient. They feared that whether efforts to learn them are futile. (Fourth-year medical student)
260 Academic Medicine, Vol. 83, No. 3 / March 2008
Clinical Teaching
Learners believed that inclusion of Learners emphasized the value of having every topic than the medical student.
patients permits clarification of historical attendings available on the ward on a (First-year IM resident)
facts and validation of exam findings. It consistent basis. Attending time on the
allows the medical team to educate ward should be “protected” from Develop faculty attitudes, knowledge,
patients about their conditions and competing responsibilities. and skill for bedside teaching. Learners
options for care. They felt that suggested faculty and resident training to
establishing rapport with patients could It really helps when the focus of that develop effective bedside teaching skills.
alleviate concerns regarding discussion person’s day is to take care of patients Such training could alleviate the anxiety
and to do teaching . . . it makes a big related to bedside teaching content, such
of sensitive topics and prevent difference . . . rather than someone who’s
misunderstandings or alarm with regard as physical examination skills. They
got their hands in so many things, their
to discussion of diagnostic possibilities or advocated a variety of bedside teaching
mind might be in as many places.
management plans. Patients might also (Fourth-year medical student) strategies, including assessment of
have the satisfaction of contributing to learners’ needs, role modeling, selective
the education of future physicians. Provide learners with reassurance, and explicit instruction, learner
reinforce their autonomy, and evaluation and feedback, and distribution
The attending did a good job of making incorporate them into the teaching of teaching responsibility. Legitimate
the patient feel we cared about her. He set process. To alleviate their anxiety at the institutional incentives for proficient
a good example of making her feel like a bedside, learners believed that simple teaching should be available.
whole person and not a specimen, in the
reassurance by the attending physician is Everything counts the minute you walk
end reassuring her about her findings:
“This isn’t new, this is something that often sufficient. They advocated the into the patient’s room. Everything
we’ve already known you have, and what establishment of a positive learning you do is being watched, whether it’s
I’m talking about here isn’t anything for environment in which acknowledgement something you say, or it’s the way you
you to worry about, and it’s consistent of deficiencies and errors is accepted as approach the patient, the way you sit by
with the diagnosis you have and nothing’s the bed, or just the way you’re ignoring
an inevitable, if not essential, aspect of
changed.” I thought that was a good what the patient’s saying. Teachers should
the learning process. In this context, be very sensitive to that issue alone. It’s
closure to the teaching. (Fourth-year
medical student)
bedside questioning is seen as a Socratic not just the verbal aspect of teaching.
exercise in learning, not as “pimping” (Second-year IM resident)
with an intent to demoralize or cause
Address time constraints through embarrassment. Some believed that Advocate evidence-based physical
flexibility, selectivity, and integration. harmonious team dynamics facilitate diagnosis. Learners believed that the
Although many time-related factors are acceptance of one’s own limitations. indifference of the medical establishment
beyond their control, learners provided towards physical diagnosis skills derives
several suggestions to address the effect of If teachers can set the tone and what the from lack of emphasis in training, and
time constraints. Faculty accommodation expectations are and say that “it is okay to they suggested that faculty and resident
of the call schedule and resident make mistakes, we all make mistakes, but
the great doctors are the ones who take
training initiatives could improve these
workload was considered paramount. skills. They encouraged participation in
those mistakes and use them to improve
Learners stated that it is senseless to themselves,” that’s the best way to learn international medical experiences in
engage in prolonged postcall teaching in that stressful environment. (Second- which technology does not play a central
rounds when the team is too fatigued and year IM resident) role in the diagnosis and treatment of
distracted to engage in a meaningful illness.
learning experience. Faculty teaching Some residents suggested that autonomy,
at the bedside should be selective and although important for professional Some things in physical exam are actually
limited in duration. Paradoxically, growth, could sometimes be useful. There’s some literature on the
prognosis implied in a certain physical
some residents suggested that faculty counterproductive in its effect on
exam finding. Us[e] that to say, “these
participate regularly in work rounds; they opportunities for learning, because things are important and it can actually
recognized the efficiency of combining autonomy often correlates inversely with guide the management.” (Second-year IM
work and learning, especially when it attending participation. They recognized resident)
obviates the need to round later with the the need to balance their roles as
attending. Residents advocated a decrease managers and learners, although it Table 2 lists these and additional
in the number of patients they manage is often difficult to negotiate the strategies to increase and improve
on the teaching ward. Considering the appropriate level of autonomy with bedside teaching.
amount of clerical work associated with attendings. They believed that
each patient, even slight reductions in distributing teaching responsibility to Contrasting student and resident
census numbers would increase the time all team members and creating a perspectives
available for teaching. collaborative learning environment could Residents’ beliefs, such as the desire for
minimize compromise of the professional autonomy in patient care and for a
[It] is very important to prioritize, to pick relationship between learner and patient. collaborative learning environment, were
one or two pearls on the patients that more pragmatic than those of students.
you’re interested in and emphasize that, One solution is to equalize the teaching
because we’re not going to remember on the team. Just because you’re ahead of
This pragmatism stemmed from two
more than that, and we usually don’t have someone else, like the attending’s above major differences between students and
time for more than that. (First-year IM you or you’re above the intern, doesn’t residents. First, residents viewed bedside
resident) mean you’re going to know more about teaching, and teaching in general, from
Academic Medicine, Vol. 83, No. 3 / March 2008 261
Clinical Teaching
the vantage points of both learner and One of our most striking findings is the year residents’ expectation for a more
teacher. Second, their views were recognition by learners that, for the collaborative approach to teaching is
influenced by work responsibilities and a patients and themselves, sensitivity in the somewhat unexpected and compelling.
desire to have a reasonable quality of life, interpersonal aspects of bedside teaching This expectation stemmed from a need
even during training. Teaching initiatives is paramount. A poorly executed bedside for autonomy as they embraced their
that fail to recognize these differences are teaching encounter disrespects patients newfound leadership role. Their desire
often unsuccessful. and compromises learners in their roles for a collaborative approach has
as clinicians and managers, thus profound implications: if given the
Students focused on the physical diminishing their perceived autonomy. opportunity to influence the timing,
diagnosis aspects of bedside teaching to a Fear of the consequences of poor content, and process of bedside teaching,
greater degree than did residents. First- interpersonal communication during residents could have a key role in
year residents were overwhelmed with the bedside teaching is prevalent. Simple promoting the regular occurrence of such
responsibilities of daily work, and thus strategies to avoid these pitfalls, such as teaching.
found bedside teaching, and perhaps all orienting patients to the process, and
teaching, to be another demand on their explicit acknowledgment of human Our findings complement previous
limited time, and they reported that they limitations, can be easily incorporated by literature reports regarding learners’
often felt too distracted to learn. In the faculty. perspectives on bedside teaching. In a
second year of residency and beyond, study by Nair et al,26 learners were found
residents recognized that their role as a Although lack of time is frequently to believe that bedside teaching is a
team leader allowed them opportunities described as a major barrier to bedside “valuable way to develop professional
to influence the frequency and form of teaching, some learners believed that this skills.” More than 90% of the learners
bedside teaching rounds. is more perception than reality. In fact, believed that bedside teaching is effective
the data suggest that when time is for learning communication, history-
There were definitely times where
somebody said the word[s] “attending limited, all teaching is compromised, not taking, and physical examination skills.
rounds” and I was ready to shoot myself. I just bedside teaching. More importantly, Between 41% and 65% stated that they
was completely disinterested and in fact learners suggested that properly executed do not receive sufficient bedside teaching.
angry that that was what somebody bedside teaching could be integrated Our findings also complement the views
wanted to do when I had a million other within typical clinical activities, such as
things, and it was only going to keep me
of teachers. In another study by Nair et
work rounds, allowing efficient time use. al,27 95% of teachers agreed that bedside
in the hospital really late. Some people
just don’t have any understanding of teaching is an effective way to develop
Autonomy was a major concern for
what’s going on around them. (First-year professional skills, and more than 80%
IM resident) residents. They avoid teaching situations
believed that it is effective for learning
that might jeopardize their role as
communication, history-taking, and
The resident’s attitude permeates the manager and the students’ or first-year
team, so you can create a local physical examination skills. Comparison
residents’ role as caregiver. A collaborative
environment of eagerness and motivation with a study by Ramani et al28 reveals
approach to teaching helps to preserve
to learn. (Second-year IM resident) a striking similarity between the
the integrity of their semiautonomous
perspectives of teachers and the views of
roles. Learners found it difficult to admit
our learners; teachers concurred with the
Discussion “I don’t know” during a bedside teaching
five overarching themes we describe in
encounter. Reassurance by attendings
Our learners confirmed faculty beliefs this paper, including learner autonomy,
and the establishment of a positive
that bedside teaching is valuable for as suggested by a “fear of undermining
learning environment and harmonious
learning essential clinical skills, such as housestaff.” They also suggested
team dynamics can alleviate these
those related to physician–patient strategies to increase and improve
concerns.
communication, physical examination, bedside teaching that are remarkably
clinical reasoning, and professionalism.27,28 Learners speculated that faculty might be consistent with those of our learners,
In the absence of studies validating the reluctant to teach at the bedside because such as orienting the patient, establishing
effectiveness of bedside teaching, this of a lack of teaching skills rather than a a positive learning environment, and
affirmation by learners is important. lack of clinical competence. In their treating the learner as primary caregiver
Their recognition that they learn by opinion, the belief that technology has for the patient. The suggestions of our
observing more experienced clinicians supplanted the medical history and learners are compatible with the bedside
interact with patients supports the use of physical examination undermines teaching recommendations of various
role modeling, an implicit form of bedside teaching. Faculty development educators.29 – 42 The “model of best
teaching, at the bedside. Although they could address both of these issues. bedside teaching practices” by Janicik and
had concerns for the patient and their Fletcher,42 which describes three domains
own psychological well-being during the The differences in the perspectives of of effective bedside teaching skills
bedside teaching encounter, they students and residents regarding bedside (attending to patient comfort, focused
identified strategies to avoid potential teaching are provocative. One could teaching, and group dynamics), addresses
harm. We are encouraged, given the predict both the tremendous appeal of several of the important findings in our
learners’ beliefs that patient inclusion and bedside teaching to students as they learn study.
faculty development could rapidly the skills of clinical medicine and the
enhance the frequency and effectiveness pragmatism of first-year residents Bedside teaching, rather than being an
of bedside teaching for the benefit of all. inundated with work. However, second- antiquated mode of clinical instruction
262 Academic Medicine, Vol. 83, No. 3 / March 2008
Clinical Teaching
from a pretechnological era, is consistent retention, skill proficiency, and 3 Hill DA, Lord RSA. Complementary value of
with modern education theory. professionalism. Meanwhile, the results traditional bedside teaching and structured
clinical teaching in introductory surgical
Specifically, it is consistent with the of this study support ongoing efforts studies. Med Educ. 1991;25:471– 474.
experiential learning principles of the to promote faculty development in 4 Osler W. The natural method of teaching the
progressive movement that began in teaching and to facilitate an institutional subject of medicine. JAMA. 1901;36:1673–
medical education during the late 19th culture and environment conducive to 1679.
century, as well as with the principles of the regular occurrence of bedside 5 Futcher TB. The importance of bed-side
study and teaching. Can Med Assoc J. 1935;
adult learning as defined by Malcolm teaching. 32:357–364.
Knowles.44,45 Most striking, however, is 6 Bedside medicine—the Oslerian reliquary.
the compatibility of bedside teaching We believe clinical education that Med J Aust. 1971;1:1251–1252.
with the modern theory of situated incorporates substantial bedside teaching 7 Linfors EW, Neelon FA. The case for bedside
cognition, or contextual learning, which is an effective approach to fulfilling the rounds. N Engl J Med. 1980;303:1230 –1233.
public interest of training intelligent, 8 Morgan WL Jr. Bedside teaching. Trans Am
states that the learning of knowledge is Clin Climatol Assoc. 1981;93:164 –171.
inherently dependent on the context in skilled, and compassionate clinicians. 9 Mazzaferri EL. Bedside teaching in the
which it is learned; that is, “knowledge is Including the patient, collaborating with preparation of physicians for the 21st
situated, being in part a product of the learners, developing faculty skills, and century. Arch Intern Med. 1986;146:1912.
activity, context, and culture in which it promoting a supportive institutional 10 St. Geme JW Jr. Can we rediscover the
culture can redress a variety of barriers to bedside? Pediatrics. 1987;79:287–288.
is developed and used.”46 William Osler4 11 Belkin BM, Neelon FA. The art of
was aware of the advantages of contextual bedside teaching. In the end, “no books, observation: William Osler and the method
learning: “In what may be called the no tapes, no audio-visual aids, no of Zadig. Ann Intern Med. 1992;116:863–
natural method of teaching, the student seminars, no avant-garde philosophy will 836.
ever be substitutes for the discipline of 12 Fitzgerald FT. Bedside teaching. West J Med.
begins with the patient, continues with 1993;158:418 – 420.
the patient, and ends his studies with the the bedside medicine—the one-to-one
13 LaCombe MA. On bedside teaching. Ann
patient, using books and lectures as tools, situation where tradition, humanity, art Intern Med. 1997;126:217–220.
as means to an end.” Our learners were and science are blended.”6 14 Thibault GE. Bedside rounds revisited.
aware of this “contextual” advantage, as N Engl J Med. 1997;336:1174 –1175.
Dr. Williams is clinical instructor of medicine,
15 Kroenke K, Omori DM, Landry FJ, Lucey CR.
demonstrated by their views regarding Boston University School of Medicine, Boston,
Bedside teaching. South Med J. 1997;90:
Massachusetts. When this research was conducted,
the value of bedside teaching. One may 1069 –1074.
he was a general internal medicine clinician– educator
logically ask, how else is a student of fellow, Boston University School of Medicine MET 16 Langlois JP, Thach S. Teaching at the bedside.
medicine to become a professional, let Program, Boston, Massachusetts. Fam Med. 2000;32:528 –530.
alone learn the appropriate manner of 17 El-Bagir M, Ahmed K. What is happening to
Dr. Ramani is associate professor of medicine and bedside clinical teaching? Med Educ. 2002;36:
speaking with, touching, and comforting director of clinical skills development, Internal 1185–1188.
a patient, if not in the context of the Medicine Residency Program, Boston University 18 Payson HE, Barchas JD. A time study of
School of Medicine, Boston, Massachusetts.
bedside teaching encounter? medical teaching rounds. N Engl J Med. 1966;
Dr. Fraser is professor of linguistics and education, 273:1468 –1471.
Boston University Applied Linguistics Program and 19 Collins GF, Cassie JM, Daggett CJ. The role of
This study has several limitations. We
School of Education, Boston, Massachusetts. the attending physician in clinical training.
recruited students from only one school J Med Educ. 1978;53:429 – 431.
of medicine, and residents from only one Dr. Orlander is associate professor of medicine, 20 Tremonti LP, Biddle WB. Teaching behaviors
Boston University School of Medicine, and associate
specialty at a single academic medical chief medical service, VA Boston Health Care System,
of residents and faculty members. J Med
center. Our study explored learners’ Educ. 1982;57:854 – 859.
Boston, Massachusetts.
21 Shankel SW, Mazzaferri EL. Teaching the
opinions about bedside teaching but did resident in internal medicine. JAMA. 1986;
not address whether increasing or 256:725–729.
improving bedside teaching would lead Acknowledgments 22 Miller M, Johnson B, Greene HL, Baier M,
to better learning outcomes or enhanced This research was supported in part by the HRSA Nowlin S. An observational study of
Faculty Development Training Grant attending rounds. J Gen Intern Med. 1992;7:
patient care. Although there is always the # D55HP00215. 646 – 648.
potential for interviewer bias to influence 23 Elliot DL, Hickam DH. Attending rounds on
the views of participants during focus in-patient units: Differences between medical
group discussions, we attempted to Disclaimer and non-medical services. Med Educ. 1993;
reduce this possibility by limiting the Preliminary results of this research were 27:503–508.
presented orally at the 2005 New England SGIM 24 Wang-Cheng RM, Barnas GP, Sigmann P,
interviewer’s dialogue to questions and
Regional Meeting, Hanover, New Hampshire, Riendl PA, Young MJ. Bedside case
clarifications and by avoiding expression presentations: Why patients like them but
and by poster at the 2005 SGIM Annual Meeting,
of opinion. We also avoided asking learners don’t. J Gen Intern Med. 1989;4:
New Orleans, Louisiana, and the 2005 AAMC
whether learners “liked” bedside Annual Meeting, Boston, Massachusetts.
284 –287.
teaching; we focused instead on questions 25 Kroenke K, Simmons JO, Copley JB, Smith C.
Attending rounds: A survey of physician
concerning value, barriers, and strategies. attitudes. J Gen Intern Med. 1990;5:229 –233.
References 26 Nair BR, Coughlan JL, Hensley MF. Student
Future research should determine 1 Nahum LH. Medical teaching rounds. Conn and patient perspectives on bedside teaching.
whether faculty development directed at Med. 1966;30:225–226. Med Educ. 1997;31:341–346.
improving bedside clinical and teaching 2 Hill GL, Bowen JC, Copeland EM, 27 Nair BR, Coughlan JL, Hensley MF.
MacFadyen BV, Duke JH Jr, Dudrick SJ. Impediments to bed-side teaching. Med
skills could enhance bedside teaching and Teaching in clinical surgery: At the bedside or Educ. 1998;32:159 –162.
should focus on a variety of learner in the seminar room? J Med Educ. 1977;52: 28 Ramani S, Orlander JD, Strunin L, Barber
outcomes, including knowledge 595–597. TW. Whither bedside teaching? A focus
Academic Medicine, Vol. 83, No. 3 / March 2008 263
Clinical Teaching
group study of clinical teachers. Acad Med. 35 Cox K. Planning bedside teaching—5. 41 Ramani S. Twelve tips to improve bedside
2003;78:384 –390. Debriefing after clinical interaction. Med J teaching. Med Teach. 2003;25:112–115.
29 McLeod PJ. A successful formula for ward Aust. 1993;158:571–572. 42 Janicik RW, Fletcher KE. Teaching at the
rounds. Can Med Assoc J. 1986;134:902–904. 36 Cox K. Planning bedside teaching— 6. Bedside: A New Model. Med Teach. 2003;25:
30 Kroenke K. Attending rounds: Guidelines for Reflection on the clinical experience. Med J 127–130.
teaching on the wards. J Gen Intern Med. Aust. 1993;158:607– 608. 43 Patton MQ. Qualitative research and
1992;7:68 –75. 37 Cox K. Planning bedside teaching—7. evaluation methods. Thousand Oaks, Calif:
31 Cox K. Planning bedside teaching—1. Explication of the clinical experience. Med J Sage Publications; 2002.
Aust. 1993;158:789 –790.
Overview. Med J Aust. 1993;158:280 –282. 44 Ludmerer KM. Learning to Heal. The
38 Cox K. Planning bedside teaching— 8.
32 Cox K. Planning bedside teaching—2. Development of American Medical
Deriving working rules for next time. Med J
Preparation before entering the wards. Med J Education. Baltimore, Md: The Johns
Aust. 1993;159:64 – 65.
Aust. 1993;158:355–357. 39 Ende J. What if Osler were one of us? Hopkins University Press; 1985.
33 Cox K. Planning bedside teaching—3. Inpatient teaching today. J Gen Intern Med. 45 Knowles MS. Self-Directed Learning: A Guide
Briefing before seeing the patient. Med J Aust. 1997;12(suppl 2):41– 48. for Learners and Teachers. New York, NY:
1993;158:417– 418. 40 Mooradian NL, Caruso JW, Kane GC. Association Press; 1975.
34 Cox K. Planning bedside teaching— 4. Increasing the time faculty spend at the 46 Brown JS, Collins A, Duguid P. Situated
Teaching around the patient. Med J Aust. bedside during teaching rounds. Acad Med. cognition and the culture of learning. Educ
1993;158:493– 495. 2001;76:200. Res. 1989;18:32– 42.
Correction
In the article “Beyond the Dual Degree: Development of a Five-Year Program in Leadership for Medical Undergraduates,” in the
January 2008 issue of Academic Medicine, an author’s name was misspelled. The correct authors are: Gerald E. Crites, MD, MEd,
James R. Ebert, MD, MBA, and Richard J. Schuster, MD, MMM.
264 Academic Medicine, Vol. 83, No. 3 / March 2008
You might also like
- EEG Spike-Wave Pattern in Childhood EpilepsyDocument4 pagesEEG Spike-Wave Pattern in Childhood EpilepsyjumasriNo ratings yet
- Whoqol: User ManualDocument106 pagesWhoqol: User Manualclaimstudent3515No ratings yet
- Short StatureDocument32 pagesShort Statureclaimstudent3515100% (1)
- Dr. Shazia Aurangzeb Assistant Professor in Paeds KTHDocument42 pagesDr. Shazia Aurangzeb Assistant Professor in Paeds KTHclaimstudent3515No ratings yet
- Cerebral Palsy in Pakistani Children: A Hospital Based SurveyDocument8 pagesCerebral Palsy in Pakistani Children: A Hospital Based Surveyclaimstudent3515No ratings yet
- Acuteabdomenseminar 160617111757 PDFDocument38 pagesAcuteabdomenseminar 160617111757 PDFclaimstudent3515No ratings yet
- Fine Needle Aspiration Cyto (FNAC): Procedure, Uses, RisksDocument90 pagesFine Needle Aspiration Cyto (FNAC): Procedure, Uses, Risksclaimstudent3515No ratings yet
- Handling Specimens for PathologyDocument23 pagesHandling Specimens for Pathologyclaimstudent3515No ratings yet
- Fine Needle Aspiration Cyto (FNAC): Procedure, Uses, RisksDocument90 pagesFine Needle Aspiration Cyto (FNAC): Procedure, Uses, Risksclaimstudent3515No ratings yet
- Two Concepts of FreedomDocument28 pagesTwo Concepts of Freedomclaimstudent3515No ratings yet
- A. Flutter, AFDocument80 pagesA. Flutter, AFclaimstudent3515No ratings yet
- Measuring Health: Methods for Assessing Quality of Life and Health OutcomesDocument44 pagesMeasuring Health: Methods for Assessing Quality of Life and Health Outcomesclaimstudent3515No ratings yet
- 5 - Ventricular Tachyarrhythmias DoneDocument79 pages5 - Ventricular Tachyarrhythmias Doneclaimstudent3515No ratings yet
- 12 - Pitutary DiseasesDocument38 pages12 - Pitutary Diseasesclaimstudent3515No ratings yet
- Learning Professionalism PerspectivesDocument8 pagesLearning Professionalism Perspectivesclaimstudent3515No ratings yet
- First Steps For Managing An Outbreak of Acute Diarrhoea: Don'T ForgetDocument8 pagesFirst Steps For Managing An Outbreak of Acute Diarrhoea: Don'T Forgetclaimstudent3515No ratings yet
- Bachelor of Medicine and Bachelor of Surgery (MB BS)Document24 pagesBachelor of Medicine and Bachelor of Surgery (MB BS)claimstudent3515No ratings yet
- Zeeshan QureshiDocument4 pagesZeeshan Qureshiclaimstudent3515No ratings yet
- Calcium For Mbbs StudentsDocument17 pagesCalcium For Mbbs Studentsclaimstudent3515No ratings yet
- Which Stats TestDocument2 pagesWhich Stats Testaby251188No ratings yet
- PedsQL4 0PCDocument2 pagesPedsQL4 0PCRuth FebrinaNo ratings yet
- Thyroid CADocument10 pagesThyroid CAclaimstudent3515No ratings yet
- Graphical Analysis and Errors - MBLDocument7 pagesGraphical Analysis and Errors - MBLclaimstudent3515No ratings yet
- Lesson 33: Horizontal & Vertical Circular ProblemsDocument5 pagesLesson 33: Horizontal & Vertical Circular Problemsclaimstudent3515No ratings yet
- Lesson 33: Horizontal & Vertical Circular ProblemsDocument5 pagesLesson 33: Horizontal & Vertical Circular Problemsclaimstudent3515No ratings yet
- Lec24 Conservation LawsDocument20 pagesLec24 Conservation LawsReddyvari VenugopalNo ratings yet
- Magnetic Field FactsheetDocument4 pagesMagnetic Field Factsheetclaimstudent3515No ratings yet
- MutationsDocument13 pagesMutationsclaimstudent3515No ratings yet
- Lec24 Conservation LawsDocument20 pagesLec24 Conservation LawsReddyvari VenugopalNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- CME Programme: Attendence Made CompulsoryDocument10 pagesCME Programme: Attendence Made CompulsoryVivek PoojaryNo ratings yet
- Hospital Patient Satisfaction QuestionnaireDocument3 pagesHospital Patient Satisfaction QuestionnaireprinceNo ratings yet
- AHM 250 SummaryDocument116 pagesAHM 250 SummaryDinesh Anbumani100% (5)
- Health & Wellness - Indian Perspective 2014 PDFDocument64 pagesHealth & Wellness - Indian Perspective 2014 PDFSamir DashputreNo ratings yet
- Report FernandezDocument3 pagesReport Fernandezrohitkamath7No ratings yet
- CSMA (Central Services Medical Attendance)Document16 pagesCSMA (Central Services Medical Attendance)Vaishu YadavNo ratings yet
- AMA SpecialtyByTOPS 12-9-10Document10 pagesAMA SpecialtyByTOPS 12-9-10bmartindoyle6396No ratings yet
- NF Clinical Nurse CHNDocument4 pagesNF Clinical Nurse CHNMelissa DumantayNo ratings yet
- Guidelines For PhysiciansDocument34 pagesGuidelines For PhysiciansSajid KhanNo ratings yet
- Pages From G.3.15 - Medical Emergency Response - UnlockedDocument13 pagesPages From G.3.15 - Medical Emergency Response - UnlockedSHAILENDRANo ratings yet
- Vaibhav Super Specialty HospitalDocument101 pagesVaibhav Super Specialty Hospitalvaibhavkamdar100% (6)
- Psthe 1Document111 pagesPsthe 1Angelica RicoNo ratings yet
- Dental Specialtiesespecilidad Dental - Passive VoiceDocument5 pagesDental Specialtiesespecilidad Dental - Passive VoiceAna Maria Mesones AlvitresNo ratings yet
- Mmha EcoDocument54 pagesMmha EcoAlfredo De Ocampo JrNo ratings yet
- Consultant General SurgeryDocument2 pagesConsultant General SurgeryMohamed AbbasNo ratings yet
- Chits Website UKDocument26 pagesChits Website UKChits Website UK100% (1)
- List of Medical Facilities in India: WWW - Gov.ukDocument81 pagesList of Medical Facilities in India: WWW - Gov.ukShah PratikNo ratings yet
- 02 Annex A - July 2020 AST Traineeship Information PDFDocument5 pages02 Annex A - July 2020 AST Traineeship Information PDFClarissa CheongNo ratings yet
- Australian Medical Council (Amc) Exam (Brief Overview)Document11 pagesAustralian Medical Council (Amc) Exam (Brief Overview)ahmerNo ratings yet
- Visions of Paulding County 2012Document27 pagesVisions of Paulding County 2012PauldingProgressNo ratings yet
- NKTI Physician Directory: Anesthesiology SpecialistsDocument126 pagesNKTI Physician Directory: Anesthesiology SpecialistsThebestearldom0% (1)
- Manipal Health Enterprises Meeting NoticeDocument106 pagesManipal Health Enterprises Meeting NoticeAmarnadh KinthaliNo ratings yet
- Coping With Schizophreni A Guide For Patients Families and CaregiversDocument9 pagesCoping With Schizophreni A Guide For Patients Families and CaregiversAathi PathmanathanNo ratings yet
- Types of DoctorsDocument5 pagesTypes of DoctorsPranav Teja100% (1)
- ePIC 2011Document281 pagesePIC 2011Serge RavetNo ratings yet
- Where Can A Surgeon PublishDocument12 pagesWhere Can A Surgeon PublishSiddharth DorairajanNo ratings yet
- Ow To:: How To Apply For Certificate of Eligibility For Specialist Registration (CESR)Document2 pagesOw To:: How To Apply For Certificate of Eligibility For Specialist Registration (CESR)Sanjeev GargNo ratings yet
- Resumen - Act 14 - Ley de Incentivos para La Retención y Retorno de Profesionales MédicosDocument1 pageResumen - Act 14 - Ley de Incentivos para La Retención y Retorno de Profesionales MédicosEdgardo VázquezNo ratings yet
- Canadian Medical Residency FM Guide For CarmsDocument234 pagesCanadian Medical Residency FM Guide For CarmsJatinder Singh100% (1)
- Skyline Medical Trauma Center Site Visit ReportDocument8 pagesSkyline Medical Trauma Center Site Visit ReportUSA TODAY NetworkNo ratings yet