You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Liberty insurance confirmation of non-land transport coverDocument3 pagesLiberty insurance confirmation of non-land transport coverrmateo_caniyasNo ratings yet
- Gentle Yoga For BeginnersDocument20 pagesGentle Yoga For Beginnersk_vasanNo ratings yet
- Orthopedics QuestionsDocument15 pagesOrthopedics QuestionsAbdullaNo ratings yet
- 1-Muscle of Upper Extremeties-TableDocument4 pages1-Muscle of Upper Extremeties-TableJan JeminoNo ratings yet
- Dactyloscopy (Science of Fingerprints)Document45 pagesDactyloscopy (Science of Fingerprints)Angel Villamor Cachero67% (3)
- Secrets of Shaolin Temple Boxing-1Document76 pagesSecrets of Shaolin Temple Boxing-1AlexNo ratings yet
- Tabla:: Basics and Performance TechniquesDocument2 pagesTabla:: Basics and Performance TechniquesFrank AcostaNo ratings yet
- Portrait Posing GuideDocument458 pagesPortrait Posing GuideClaudiu RusuNo ratings yet
- Extraoral Examination 1Document58 pagesExtraoral Examination 1SyaZuWaN JaMiLNo ratings yet
- Cast Types and Maintenance InstructionsDocument32 pagesCast Types and Maintenance InstructionsFerdinand Costales100% (2)
- Hailey Bieber Hand Tattoo - Google Search PDFDocument1 pageHailey Bieber Hand Tattoo - Google Search PDFRezzan TimurNo ratings yet
- Assessing The Neurologic System by Jacquelyn AngelesDocument12 pagesAssessing The Neurologic System by Jacquelyn AngelesGlen CaguranganNo ratings yet
- Sri Kala Bhairava Upasana-Vatuka Bhairava JapaDocument5 pagesSri Kala Bhairava Upasana-Vatuka Bhairava JapaKrishna Kumar100% (6)
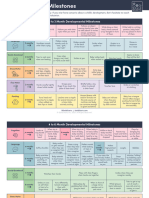
- Solid Starts - Developmental MilestonesDocument6 pagesSolid Starts - Developmental Milestonestohru89No ratings yet
- 7 - HandDocument30 pages7 - Handعاصم مروانNo ratings yet
- Ergonomic Stretches For The OfficeDocument6 pagesErgonomic Stretches For The OfficeDwiki PradiptoNo ratings yet
- Pencil Grasp DevelopmentDocument1 pagePencil Grasp Developmentemisa reskiNo ratings yet
- Jade Body GongDocument16 pagesJade Body Gonganiky30No ratings yet
- Inheritance of Fingerprint Patterns InheritedDocument17 pagesInheritance of Fingerprint Patterns InheritedSanskar SrivastavaNo ratings yet
- Functions of Human MuscleDocument4 pagesFunctions of Human MuscleCatherine EscartinNo ratings yet
- Pal Dan GumDocument5 pagesPal Dan GumJacob Post100% (1)
- Thumb UltrasoundDocument11 pagesThumb Ultrasoundsun flowerrNo ratings yet
- Cambridge Checkpoint Science Skills Builder 7Document25 pagesCambridge Checkpoint Science Skills Builder 7như hải võ54% (41)
- Drills and CeremoniesDocument237 pagesDrills and CeremoniesJovie MasongsongNo ratings yet
- Dim Mak Vital Points From Rick ClarkDocument7 pagesDim Mak Vital Points From Rick Clarknakadakaken100% (1)
- Gaṇeśamātṛkā Nyāsa Mantra DhyānaDocument21 pagesGaṇeśamātṛkā Nyāsa Mantra DhyānaChanchala RaoNo ratings yet
- ZiJiu 2 3 and 5 PDFDocument132 pagesZiJiu 2 3 and 5 PDFJettNo ratings yet
- Pathfinder Drilling and Marching GuideDocument13 pagesPathfinder Drilling and Marching GuideElida Valdez De Jose100% (1)
- Joint Mobilization To The Elbow, Wrist and Hand2Document43 pagesJoint Mobilization To The Elbow, Wrist and Hand2Tripty Khanna Karwal100% (1)
- Dactyloscopy (Q&A)Document15 pagesDactyloscopy (Q&A)Jeneva Castillo Abadilla100% (2)