You might also like
- Lung Growth and Development: Suchita Joshi, Sailesh KotechaDocument6 pagesLung Growth and Development: Suchita Joshi, Sailesh KotechaAditya SanjayaNo ratings yet
- 12 Lung DevelopmentDocument36 pages12 Lung Developmentf3er3No ratings yet
- Neonatal Pulmonary PhysiologyDocument6 pagesNeonatal Pulmonary PhysiologyAnapaolaNo ratings yet
- Ultrasound in Obstet Gyne - 2002 - Laudy - The Fetal Lung 1 Developmental AspectsDocument7 pagesUltrasound in Obstet Gyne - 2002 - Laudy - The Fetal Lung 1 Developmental AspectsRafael JustinoNo ratings yet
- Neonatal Respiration PhysiologyDocument6 pagesNeonatal Respiration PhysiologyRaja Ahmad Rusdan MusyawirNo ratings yet
- Neonatal Respiratory Care: Moderated By: Shyam Krishnan Presented By: A Sampath KumarDocument62 pagesNeonatal Respiratory Care: Moderated By: Shyam Krishnan Presented By: A Sampath KumarPrethy PhilipNo ratings yet
- Malformaciones Congenitas Neoreviews - 2016 - May - 17 (5) - E263Document10 pagesMalformaciones Congenitas Neoreviews - 2016 - May - 17 (5) - E263valentina rojasNo ratings yet
- RDS Ppts 2021Document37 pagesRDS Ppts 2021Mohammad NajjarNo ratings yet
- 1 (Lung Development)Document12 pages1 (Lung Development)Dr.sonuNo ratings yet
- ExamView - Chapter - 0124Document2 pagesExamView - Chapter - 0124Devin MckayNo ratings yet
- ExamView - Chapter - 01Document2 pagesExamView - Chapter - 01Devin MckayNo ratings yet
- Fetal Cardiopulmonary Development OutlineDocument7 pagesFetal Cardiopulmonary Development OutlineRLibdehNo ratings yet
- Askep (RDS) Atmawira Massi (Kep B 2021)Document20 pagesAskep (RDS) Atmawira Massi (Kep B 2021)Mama WiraNo ratings yet
- Developmental Biology of The Pulmonary Circulation: Alison HislopDocument10 pagesDevelopmental Biology of The Pulmonary Circulation: Alison HislopMarcela RodriguezNo ratings yet
- Management of Congenital Lung Malformations 2022 Clinic PerinatolDocument20 pagesManagement of Congenital Lung Malformations 2022 Clinic PerinatolAna Maria Fidelis Silva camposNo ratings yet
- Congenital Cystic Adenomatoid Malformation (CCAM)Document7 pagesCongenital Cystic Adenomatoid Malformation (CCAM)sarguss14No ratings yet
- Diagnostic and Management of Hyaline Membrane Disease: August 2018Document11 pagesDiagnostic and Management of Hyaline Membrane Disease: August 2018Bella MonichaNo ratings yet
- Human Lung DevelopmentDocument20 pagesHuman Lung DevelopmentMila KarmilaNo ratings yet
- Pediatric and Neonatal Respiratory Care DevelopmentDocument205 pagesPediatric and Neonatal Respiratory Care DevelopmentAlexander Santiago ParelNo ratings yet
- 1molecular DeterminantsDocument16 pages1molecular DeterminantsSelene GlezNo ratings yet
- Developmental Physiology - Lung Function During Growth and Development From Birth To Old Age by Calogero 2010Document15 pagesDevelopmental Physiology - Lung Function During Growth and Development From Birth To Old Age by Calogero 2010Fe TusNo ratings yet
- 4Document7 pages4UgaugaaNo ratings yet
- Embryo Development Lungs+Body CavityDocument8 pagesEmbryo Development Lungs+Body CavityKingNo ratings yet
- Lecture 1 - Development of Respiratory SystemDocument27 pagesLecture 1 - Development of Respiratory SystemRachmad MusyaffaNo ratings yet
- Respiratory Distress in The NewbornDocument146 pagesRespiratory Distress in The NewbornAmit RamrattanNo ratings yet
- Introduction To Physiological Changes in NEONATAL AND PEDIATRIC RESPICARE James Astrologo LamusaoDocument88 pagesIntroduction To Physiological Changes in NEONATAL AND PEDIATRIC RESPICARE James Astrologo LamusaoDanao, Aira A.No ratings yet
- Neonatal Respiratory Distress Syndrome: July 2020Document12 pagesNeonatal Respiratory Distress Syndrome: July 2020Ahmed ElhadiNo ratings yet
- M.03 Respiratory Disorders of Children Part 1 (Dr. Tandoc) (10-26-20)Document7 pagesM.03 Respiratory Disorders of Children Part 1 (Dr. Tandoc) (10-26-20)VanessaNo ratings yet
- Respiratory System Development - EmbryologyDocument1 pageRespiratory System Development - EmbryologyRicardo david Reyes alvarezNo ratings yet
- Development of Respiratory System: Dr. Saeed Vohra & Dr. Sanaa AlshaarawyDocument26 pagesDevelopment of Respiratory System: Dr. Saeed Vohra & Dr. Sanaa AlshaarawyChristineNo ratings yet
- Kelompok 1 Kelas 3C AskepDocument39 pagesKelompok 1 Kelas 3C AskepWidya KusumaningrumNo ratings yet
- All About RespiratoryDocument69 pagesAll About RespiratoryMarcellina Awing100% (1)
- Management of Respiratory Distress Syndrome: An Update: Ricardo J Rodriguez MDDocument9 pagesManagement of Respiratory Distress Syndrome: An Update: Ricardo J Rodriguez MDIndah Afriani NasutionNo ratings yet
- ALVIRA 2017_Can We Understand the Pathobiology of Bronchopulmonary DysplasiaDocument11 pagesALVIRA 2017_Can We Understand the Pathobiology of Bronchopulmonary DysplasiaRafael JustinoNo ratings yet
- Test Bank For Neonatal and Pediatric Respiratory Care 4th Edition Brian K Walsh DownloadDocument3 pagesTest Bank For Neonatal and Pediatric Respiratory Care 4th Edition Brian K Walsh DownloadLowell Garcia100% (27)
- Embryonic 8wks (3-7wks) Lung Hypoplasia, TEF Pseudoglandular 16 Wks CDH Canalicular 24 Wks Surfactant def-RDSDocument40 pagesEmbryonic 8wks (3-7wks) Lung Hypoplasia, TEF Pseudoglandular 16 Wks CDH Canalicular 24 Wks Surfactant def-RDSMischief ManagerNo ratings yet
- LP RDS Di Rsud DayaDocument6 pagesLP RDS Di Rsud DayaRoberto Asmat SelungNo ratings yet
- STEM CELLS Translational Med - 2021 - Ushakumary - Resident Interstitial Lung Fibroblasts and Their Role in Alveolar StemDocument12 pagesSTEM CELLS Translational Med - 2021 - Ushakumary - Resident Interstitial Lung Fibroblasts and Their Role in Alveolar StemDheerendra K PandeyNo ratings yet
- Warren 2009 RDSDocument13 pagesWarren 2009 RDSCIRUABCNo ratings yet
- Bronchioles Then Divide Into Three TypesDocument3 pagesBronchioles Then Divide Into Three TypesJeremy EvansNo ratings yet
- 20 - Development of Respiratory SystemDocument33 pages20 - Development of Respiratory SystemDr.B.B.GosaiNo ratings yet
- Respiratory Distress SyndromeDocument3 pagesRespiratory Distress SyndromeAshNo ratings yet
- Respiratory Distress SyndromeDocument9 pagesRespiratory Distress SyndromeRamina HiponiaNo ratings yet
- SILVA 2015 - Recent Advances in The Mechanismo of Lung Alveolarization and The Pathogenesis of BPDDocument34 pagesSILVA 2015 - Recent Advances in The Mechanismo of Lung Alveolarization and The Pathogenesis of BPDRafael JustinoNo ratings yet
- Congenital Diaphragmatic HerniaDocument4 pagesCongenital Diaphragmatic HerniaJulio AltamiranoNo ratings yet
- 3 RestrictiveLungDiseasesDocument14 pages3 RestrictiveLungDiseasesSaiaDaphiNo ratings yet
- Bronchopulmonary Dysplasia and Chronic Lung Disease of Infancy: Strategies For Prevention and ManagementDocument13 pagesBronchopulmonary Dysplasia and Chronic Lung Disease of Infancy: Strategies For Prevention and ManagementArsy Mira PertiwiNo ratings yet
- Embryology of Respiratory System NotesDocument3 pagesEmbryology of Respiratory System NotesJulienne Sanchez-SalazarNo ratings yet
- 3-Embryology of Respiratory SystemDocument25 pages3-Embryology of Respiratory SystemNur HikmahNo ratings yet
- Vipin Sharma Embryogenesis of Respiratory SystemDocument31 pagesVipin Sharma Embryogenesis of Respiratory SystemRitvik SharmaNo ratings yet
- Ncma113 Finals-ReviewerDocument84 pagesNcma113 Finals-ReviewerYu AnNo ratings yet
- Control of BreathingDocument12 pagesControl of BreathingAbeer SallamNo ratings yet
- Embryo Exam 2: Respiratory System: Download The Android App!Document4 pagesEmbryo Exam 2: Respiratory System: Download The Android App!AzizNo ratings yet
- Respiratory ARC3 2pathophysiologyDocument22 pagesRespiratory ARC3 2pathophysiologyYashmine CastrenceNo ratings yet
- PAPER - Lung OrganogenesisDocument93 pagesPAPER - Lung OrganogenesisDhinta Dwi YuliantiNo ratings yet
- Bronchopulmonary Dysplasia: An Update: Anita Bhandari and Vineet BhandariDocument5 pagesBronchopulmonary Dysplasia: An Update: Anita Bhandari and Vineet BhandariPatricius Berry Harsono PutraNo ratings yet
- RODRIGUES-CASTILLO 2018 - Understanding Alveolarization To Induce Lung RegenerationDocument11 pagesRODRIGUES-CASTILLO 2018 - Understanding Alveolarization To Induce Lung RegenerationRafael JustinoNo ratings yet
- Prematuridad Extream y Enfermedad Respiratoria Del AdultoDocument1 pagePrematuridad Extream y Enfermedad Respiratoria Del Adultocarlos felipe gonzalez soteloNo ratings yet
- Pulmonary Endocrine Pathology: Endocrine Cells and Endocrine Tumours of the LungFrom EverandPulmonary Endocrine Pathology: Endocrine Cells and Endocrine Tumours of the LungNo ratings yet
- Lung Development Biological and Clinical Perspectives: Biochemistry and PhysiologyFrom EverandLung Development Biological and Clinical Perspectives: Biochemistry and PhysiologyPhilip FarrellNo ratings yet
- Amin Ch2 Pathology of The Renal Pelvis and UreterDocument34 pagesAmin Ch2 Pathology of The Renal Pelvis and UretersandyNo ratings yet
- NZClinicalGuidelinesStrokeManagement2010ActiveContents PDFDocument347 pagesNZClinicalGuidelinesStrokeManagement2010ActiveContents PDFsandyNo ratings yet
- Editorial: Ureteropelvic Junction Obstruction (Upjo) in InfantsDocument2 pagesEditorial: Ureteropelvic Junction Obstruction (Upjo) in InfantssandyNo ratings yet
- Pathophysiology of RDSDocument5 pagesPathophysiology of RDSsandyNo ratings yet
- 10 1 1 525 6842Document6 pages10 1 1 525 6842sandyNo ratings yet
- APJMT Volume 4 Issue 2 Pages 58-63Document6 pagesAPJMT Volume 4 Issue 2 Pages 58-63sandyNo ratings yet
- Jpn. J. Clin. Oncol.-2007-Iwamoto-79-89Document11 pagesJpn. J. Clin. Oncol.-2007-Iwamoto-79-89Muhammad SyaifullahNo ratings yet
- APJMT Volume 4 Issue 2 Pages 58-63Document6 pagesAPJMT Volume 4 Issue 2 Pages 58-63sandyNo ratings yet
- Puj ObstructionDocument2 pagesPuj ObstructionsandyNo ratings yet
- 10 1 1 525 6842Document6 pages10 1 1 525 6842sandyNo ratings yet
- BMED3100 Fall16 HW4-keyDocument2 pagesBMED3100 Fall16 HW4-keyAnonymous yWHBqVa3No ratings yet
- Mechanical Ventilation Mechanical Ventilation: Dr. Ravi Gadani MS, Fmas Dr. Ravi Gadani MS, FmasDocument35 pagesMechanical Ventilation Mechanical Ventilation: Dr. Ravi Gadani MS, Fmas Dr. Ravi Gadani MS, FmasRaviNo ratings yet
- Bilevel VentilationDocument18 pagesBilevel VentilationBonehead7No ratings yet
- PulmoVista 500 - APPLICATION - Estimate Possible Overdistension - 032018Document2 pagesPulmoVista 500 - APPLICATION - Estimate Possible Overdistension - 032018tomNo ratings yet
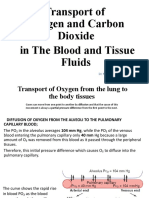
- Transport of Oxygen and Crabon Dioxid in The Blood and Tissue FluidDocument19 pagesTransport of Oxygen and Crabon Dioxid in The Blood and Tissue FluidSAKARIYE MAXAMEDNo ratings yet
- Septic ShockDocument3 pagesSeptic ShockYuvi Rociandel LUARDONo ratings yet
- CH 25 Respiration Study GuideDocument2 pagesCH 25 Respiration Study Guide99646qbkdwNo ratings yet
- Introduction To Pediatric VentilationDocument41 pagesIntroduction To Pediatric Ventilationedderj2585No ratings yet
- Bio1 Respiratory System 1Document41 pagesBio1 Respiratory System 1Camela Kim Domider TenorioNo ratings yet
- Mechanical Ventilation Airway Pressure Release Ventilation Checklist Respiratory Therapy - 070420Document3 pagesMechanical Ventilation Airway Pressure Release Ventilation Checklist Respiratory Therapy - 070420shubham2812No ratings yet
- COPD PathophysiologyDocument1 pageCOPD PathophysiologyJustin Ahorro-Dionisio33% (3)
- Oxygen Therapy GuidelinesDocument19 pagesOxygen Therapy GuidelinesAyuna Rahmani0% (1)
- Case Study Near DrowningDocument6 pagesCase Study Near DrowningNashwa Fathira0% (1)
- Ineffective Airway Clearance Pneumonia Nursing Care PlanDocument1 pageIneffective Airway Clearance Pneumonia Nursing Care Planjustin_sane100% (4)
- (Draeger) DYK Infographic - Recruitment Maneuvers (Sustained Inflation - 40 by 40) en (2023)Document1 page(Draeger) DYK Infographic - Recruitment Maneuvers (Sustained Inflation - 40 by 40) en (2023)ConstantineSemenchukNo ratings yet
- AARC Clinical Practice Guideline: Incentive SpirometryDocument10 pagesAARC Clinical Practice Guideline: Incentive SpirometrytruptimptNo ratings yet
- Aerobic Respiration: Chemiosmosis and Electron Transport ChainDocument17 pagesAerobic Respiration: Chemiosmosis and Electron Transport ChainAihk kenneth BaronaNo ratings yet
- Circulation and Respiration Revision EOYDocument2 pagesCirculation and Respiration Revision EOYSwetha SureshNo ratings yet
- Respiration in Organisms - Others - CBSE7B - Respiration in Organisms - Test - 01Document2 pagesRespiration in Organisms - Others - CBSE7B - Respiration in Organisms - Test - 01Vansh BhallaNo ratings yet
- Tugas Bahasa Inggris Ii: Adinda Dwi Pangestu 18. 156. 01. 11. 002 2A KeperawatanDocument5 pagesTugas Bahasa Inggris Ii: Adinda Dwi Pangestu 18. 156. 01. 11. 002 2A KeperawatanAdinda Dwi PangestuNo ratings yet
- Diaphragmatic BreathingDocument3 pagesDiaphragmatic BreathingrobinjudeNo ratings yet
- ESICM Guidelines On Acute Respiratory Distress Syndrome - Definition, Phenotyping and Respiratory Support StrategiesDocument33 pagesESICM Guidelines On Acute Respiratory Distress Syndrome - Definition, Phenotyping and Respiratory Support StrategiesAbenamar VelardeNo ratings yet
- Mechanical Ventilation - Chapter 2Document2 pagesMechanical Ventilation - Chapter 2Raninda JuliantiNo ratings yet
- Control of Breathing: DR - Anto MathewDocument44 pagesControl of Breathing: DR - Anto Mathewanto mathewNo ratings yet
- Oxidative Phosphorylation V Inhibitors and UncouplersDocument15 pagesOxidative Phosphorylation V Inhibitors and UncouplersIffatnazNo ratings yet
- The ABC of Weaning Failure - A Structured ApproachDocument9 pagesThe ABC of Weaning Failure - A Structured ApproachArul ShanmugamNo ratings yet
- Electron Transport Chain and ChemiosmosisDocument3 pagesElectron Transport Chain and ChemiosmosisAddisNo ratings yet
- Respiration in Plants: Fact/Definition Type QuestionsDocument12 pagesRespiration in Plants: Fact/Definition Type QuestionsAditya DeshmukhNo ratings yet
- Day 117-119d Cellular Respiration Active NotesDocument4 pagesDay 117-119d Cellular Respiration Active NotesYousif AlaniNo ratings yet
- Arterial Blood Gas Analysis: Dr. Rakesh Chandra Chaurasia PG3 Ims, Bhu Moderator Dr. YashpalDocument34 pagesArterial Blood Gas Analysis: Dr. Rakesh Chandra Chaurasia PG3 Ims, Bhu Moderator Dr. YashpalArmaanjeet SinghNo ratings yet