You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- RhesusDocument1 pageRhesuswedishaNo ratings yet
- Puerperal SepsisDocument1 pagePuerperal Sepsiswedisha100% (1)
- PromDocument1 pagePromwedishaNo ratings yet
- Management of Normal Labour ChartDocument1 pageManagement of Normal Labour ChartwedishaNo ratings yet
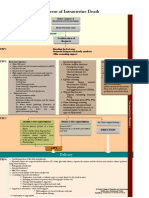
- IUDDocument1 pageIUDwedishaNo ratings yet
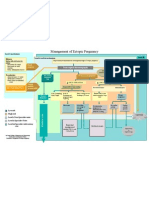
- EctopicpregnancyDocument1 pageEctopicpregnancywedisha100% (1)
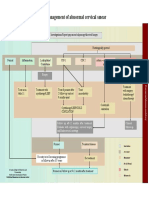
- CINDocument1 pageCINwedishaNo ratings yet
- Management of Abnormal Uterine Bleeding Peripheral Unit: Female Presenting To A With AUBDocument1 pageManagement of Abnormal Uterine Bleeding Peripheral Unit: Female Presenting To A With AUBwedishaNo ratings yet
- APHDocument1 pageAPHwedishaNo ratings yet
- BreechDocument1 pageBreechAraceli Ecot CalunodNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Sukie BCHDocument16 pagesSukie BCHapi-309519730No ratings yet
- ACOG Opinion On IAIDocument13 pagesACOG Opinion On IAIGladys GarciaNo ratings yet
- DESSERTATIONDocument9 pagesDESSERTATIONKinjal VasavaNo ratings yet
- Crane and Hord-SmithDocument26 pagesCrane and Hord-SmithJackNo ratings yet
- Chapter 1 MCNDocument14 pagesChapter 1 MCNLawrence NemirNo ratings yet
- The Effect of Birth Ball Exercises During PregnancDocument8 pagesThe Effect of Birth Ball Exercises During Pregnancmona khosraviNo ratings yet
- Normal Labour AND Delivery: Prof DR Mohd Azhar MNDocument90 pagesNormal Labour AND Delivery: Prof DR Mohd Azhar MNLiezel CauilanNo ratings yet
- H-Mole Chapter I-VDocument103 pagesH-Mole Chapter I-VJoevence Gazo CuaresmaNo ratings yet
- Review On Breast Engorgement and Its ManagementDocument3 pagesReview On Breast Engorgement and Its ManagementEditor IJTSRDNo ratings yet
- 4 FasesDocument4 pages4 FasesFERTIL CONEXIONNo ratings yet
- Hyperglycemia in PregnancyDocument17 pagesHyperglycemia in PregnancyIza WidzNo ratings yet
- Causes of MiscarriageDocument7 pagesCauses of MiscarriageClaire Nimor VentulanNo ratings yet
- Incomplete AbortionDocument37 pagesIncomplete AbortionGerarld Immanuel Kairupan100% (1)
- Menstrual Cycle LP - 1st CODocument8 pagesMenstrual Cycle LP - 1st COEsther Mae Ann TrugilloNo ratings yet
- Consent Advice Laparoscopic Tubal OcclusionDocument2 pagesConsent Advice Laparoscopic Tubal OcclusionKathJamesNo ratings yet
- Perineal Techniques During The Second Stage of Labour For Reducing Perineal Trauma (Review)Document118 pagesPerineal Techniques During The Second Stage of Labour For Reducing Perineal Trauma (Review)Ppds ObgynNo ratings yet
- Dra Juson Labor & DeliveryDocument153 pagesDra Juson Labor & DeliveryaringkinkingNo ratings yet
- Literature Study: Oketani Massage To The Flow of Breast MilkDocument2 pagesLiterature Study: Oketani Massage To The Flow of Breast MilkmarisaNo ratings yet
- Introduction To Cytology and Cytological Techniques-Dbb40103 2019Document41 pagesIntroduction To Cytology and Cytological Techniques-Dbb40103 2019Bintu AmirudinNo ratings yet
- L P APHDocument11 pagesL P APHmoni khatkarNo ratings yet
- Treatment of Thin Endometrium With Hysteroscopic Autologous Platelet Rich Plasma Injection 54wNDocument3 pagesTreatment of Thin Endometrium With Hysteroscopic Autologous Platelet Rich Plasma Injection 54wNSci Technol100% (1)
- Management of Pregnancy Related BleedingDocument75 pagesManagement of Pregnancy Related BleedingChuah Wei Hong100% (1)
- Group 2 Case Study 5 QuestionsDocument6 pagesGroup 2 Case Study 5 QuestionsChadd Vyllmorr VillarinNo ratings yet
- Detailed Record of CPD Activities Name: Ooi Siew Thin IC NO:620423-02-5398 Position/Gred: Jururawat 42 From (Month/Year) : August 2018 To 2019Document2 pagesDetailed Record of CPD Activities Name: Ooi Siew Thin IC NO:620423-02-5398 Position/Gred: Jururawat 42 From (Month/Year) : August 2018 To 2019MrS DNo ratings yet
- Carboprost TromethamineDocument2 pagesCarboprost TromethamineDeathDefying DonutNo ratings yet
- Journal Expulsion of IUDDocument12 pagesJournal Expulsion of IUDericNo ratings yet
- MBFHIDocument48 pagesMBFHIRough Ael100% (2)
- Placental Abruption PresentationDocument30 pagesPlacental Abruption PresentationNafisat AdepojuNo ratings yet
- Regodos Stages of LaborDocument91 pagesRegodos Stages of LaborIan Cyrus RegodosNo ratings yet
- VaginitisDocument16 pagesVaginitisMae Christelle Hamoy100% (2)