You might also like
- CloningDocument11 pagesCloningCindy González100% (1)
- Ebook - ENG - PSICOLOGIA The Rorschach Test 1Document10 pagesEbook - ENG - PSICOLOGIA The Rorschach Test 1Carlos Ruiz R.No ratings yet
- ICU Checklist For RoundingDocument1 pageICU Checklist For RoundingViolaNo ratings yet
- Veterinary Pharmacology 2011Document35 pagesVeterinary Pharmacology 2011Satnam singhNo ratings yet
- Oncology Lectures 1 7 DR - FerrolinoDocument24 pagesOncology Lectures 1 7 DR - FerrolinoMiguel Cuevas DolotNo ratings yet
- Cardiovascular DrugsDocument33 pagesCardiovascular DrugsKish Gabriel100% (1)
- ACLS Algorithms Adult 2010 Revised May 31 2011Document12 pagesACLS Algorithms Adult 2010 Revised May 31 2011arturschander3614No ratings yet
- Fallout Fan Bestiary 2Document155 pagesFallout Fan Bestiary 2asa0lambrecht50% (2)
- Abdominal Examination ProcedureDocument5 pagesAbdominal Examination ProcedureAnamul hossainNo ratings yet
- CH 46 Complications of AnaesthesiaDocument29 pagesCH 46 Complications of AnaesthesiaChristian LeepoNo ratings yet
- Onset Positions in Induction of Anesthesia Spinal Anesthesia Nitrous Oxide Respiratory Complications Respiratory ObstructionDocument7 pagesOnset Positions in Induction of Anesthesia Spinal Anesthesia Nitrous Oxide Respiratory Complications Respiratory ObstructionArvin Ian Penaflor50% (2)
- ACLS Primary Survey Guide for Respiratory ArrestDocument34 pagesACLS Primary Survey Guide for Respiratory Arrest강기연100% (1)
- Sinus ArrhythmiaDocument6 pagesSinus ArrhythmiaVincent Maralit MaterialNo ratings yet
- Emergency Drugs KathDocument29 pagesEmergency Drugs Kathmajin655No ratings yet
- Bowel and Bladder EliminationDocument9 pagesBowel and Bladder EliminationApril Urbano-Gabot Alap0% (1)
- Drugs in Cardiac EnmergenciesDocument94 pagesDrugs in Cardiac EnmergenciesVijayan VelayudhanNo ratings yet
- Critical Care Drugs 1Document21 pagesCritical Care Drugs 1Asri ErnadiNo ratings yet
- Blood Pressure RegulationDocument35 pagesBlood Pressure Regulationبراءة أحمد السلاماتNo ratings yet
- Metoprolol Teaching PlanDocument18 pagesMetoprolol Teaching Planapi-419091662No ratings yet
- CardiopathophysiologyDocument63 pagesCardiopathophysiologyapplesncoreNo ratings yet
- Subcutaneous Injection Guidelines: For Needle Length and Gauge SelectionDocument2 pagesSubcutaneous Injection Guidelines: For Needle Length and Gauge SelectionrevinhostingNo ratings yet
- Muscle Relaxants: Topic OutlineDocument8 pagesMuscle Relaxants: Topic OutlineBarda GulanNo ratings yet
- Chan, Johnson - TreatmentGuidelines PDFDocument0 pagesChan, Johnson - TreatmentGuidelines PDFBogdan CarabasNo ratings yet
- Cardiovascular PharmacologyDocument20 pagesCardiovascular PharmacologyAliceAliceNo ratings yet
- HFandVADRoleDocument34 pagesHFandVADRoleJohnNo ratings yet
- Giovanni Maciocia Menorrhagia NotesDocument22 pagesGiovanni Maciocia Menorrhagia Noteshihi12100% (5)
- VASOACTIVE THERAPY GUIDE FOR CRITICALLY ILL PATIENTSDocument26 pagesVASOACTIVE THERAPY GUIDE FOR CRITICALLY ILL PATIENTSlidya agustin100% (1)
- Cardiac MedicationsDocument8 pagesCardiac Medicationsangeline totaram100% (2)
- Physical ExaminationDocument55 pagesPhysical Examinationdakshpanchal26369No ratings yet
- Positive ResultDocument3 pagesPositive Resultநந்தினி வீரப்பெருமாள்No ratings yet
- Common Asthma MedicationsDocument1 pageCommon Asthma MedicationsHeart of the Valley, Pediatric CardiologyNo ratings yet
- Laughing Your Wat Pediatric Board Review Questions and AnswersDocument2 pagesLaughing Your Wat Pediatric Board Review Questions and AnswersAbdul Ghaffar Abdullah100% (1)
- Chapter 5: Analyzing A Rhythm StripDocument7 pagesChapter 5: Analyzing A Rhythm StriptellyNo ratings yet
- HW InotropesDocument3 pagesHW InotropesNatalie YeohNo ratings yet
- Vasoactive Agents For Adult Septic Shock: An Update and ReviewDocument10 pagesVasoactive Agents For Adult Septic Shock: An Update and ReviewntnquynhproNo ratings yet
- Sultan Kudarat Province Enacts Rabies Prevention OrdinanceDocument13 pagesSultan Kudarat Province Enacts Rabies Prevention OrdinanceJimmy C. Andang100% (2)
- Cs-Cardiac-023-Essential Cardiac LabsDocument2 pagesCs-Cardiac-023-Essential Cardiac LabsColeen YraolaNo ratings yet
- AnticoagulantsDocument19 pagesAnticoagulantsOsama ZbedaNo ratings yet
- ECMO and Right Ventricular FailureDocument9 pagesECMO and Right Ventricular FailureLuis Fernando Morales JuradoNo ratings yet
- Basic Anaesthetic Drugs - SheetDocument1 pageBasic Anaesthetic Drugs - SheetOxigen XenonNo ratings yet
- Emergency DrugsDocument9 pagesEmergency DrugsaldwinngNo ratings yet
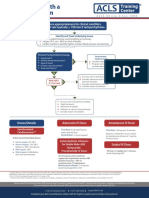
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaDocument1 pageAssess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaSiti Nur R Firda FauziyahNo ratings yet
- Ebp PaperDocument8 pagesEbp Paperapi-250304529No ratings yet
- Invasive Devices On CXRDocument1 pageInvasive Devices On CXRLaurensia Erlina NataliaNo ratings yet
- Guide To Oxygen Delivery SystemDocument3 pagesGuide To Oxygen Delivery SystemDarwin Villestas0% (1)
- Nur 111 Session 6 Sas 1Document12 pagesNur 111 Session 6 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- DRUGS AND DEFIBRILLATION IN CARDIAC ARRESTDocument20 pagesDRUGS AND DEFIBRILLATION IN CARDIAC ARRESTAfrida Sahestina100% (1)
- Best Vasopressor For Advanced Vasodilatory Shock Should Vasopressin Be Part of The MixDocument4 pagesBest Vasopressor For Advanced Vasodilatory Shock Should Vasopressin Be Part of The MixSurachai PraimaiNo ratings yet
- Sinus Bradycardia: I. Sinus Dysrhythmias Description ManagementDocument4 pagesSinus Bradycardia: I. Sinus Dysrhythmias Description ManagementMargueretti Delos ReyesNo ratings yet
- Stroke Pathway For Acute Care ProvidersDocument5 pagesStroke Pathway For Acute Care Providersdremad1974100% (1)
- Cardiac DrugsDocument3 pagesCardiac DrugsRon WoodardNo ratings yet
- EAR First AidDocument4 pagesEAR First Aidr_lakshmi2722No ratings yet
- 1538 Exam 4 Cell Reg & GriefDocument35 pages1538 Exam 4 Cell Reg & GriefJade EdanoNo ratings yet
- Cardiac Examination Inspection, Palpation & Percussion : Dr. Rajesh Bhat UDocument38 pagesCardiac Examination Inspection, Palpation & Percussion : Dr. Rajesh Bhat URanjith RavellaNo ratings yet
- Pre-op Evaluation SummaryDocument1 pagePre-op Evaluation Summarysabbo morsNo ratings yet
- Neurological Examination PDFDocument6 pagesNeurological Examination PDFArif K BashaNo ratings yet
- Assessment FindingsDocument6 pagesAssessment FindingsRoeder CuerdaNo ratings yet
- West Visayas State University: Nursing ProcessDocument4 pagesWest Visayas State University: Nursing ProcessPhylum Chordata100% (1)
- Cardiac Testing Role Risk Stratifying ED Chest PainDocument17 pagesCardiac Testing Role Risk Stratifying ED Chest PainGiorgiana pNo ratings yet
- Nursing Responsibilities For The Patient Will Undergo Cardiac CatheterizationDocument4 pagesNursing Responsibilities For The Patient Will Undergo Cardiac CatheterizationCharlene Jacobe Cornista100% (1)
- Cad ....Document94 pagesCad ....AnanthibalaNo ratings yet
- Eclampsia From MedscapeDocument11 pagesEclampsia From Medscapevicky v. p. wardenaar100% (1)
- Algorithms of Care (Myocardial Infarction)Document3 pagesAlgorithms of Care (Myocardial Infarction)Julius Delos SantosNo ratings yet
- CardioDocument7 pagesCardioGerald AndrinNo ratings yet
- MC RanitidineDocument5 pagesMC RanitidineCliff by the seaNo ratings yet
- Lisinopril, TAB: Generic Name of Medication: Brand/trade Name of MedicationDocument6 pagesLisinopril, TAB: Generic Name of Medication: Brand/trade Name of MedicationCliff by the seaNo ratings yet
- Sertraline TAB Zoloft: Medication CardDocument5 pagesSertraline TAB Zoloft: Medication CardCliff by the seaNo ratings yet
- MC HydroxyzineDocument3 pagesMC HydroxyzineCliff by the seaNo ratings yet
- MC ZolpidemDocument4 pagesMC ZolpidemCliff by the seaNo ratings yet
- MC AtorvastatinDocument3 pagesMC AtorvastatinCliff by the seaNo ratings yet
- MC BudesonideDocument3 pagesMC BudesonideCliff by the seaNo ratings yet
- MC CholecalciferolDocument2 pagesMC CholecalciferolCliff by the seaNo ratings yet
- Ther. Class. PO: (Adults) 5-10 MG Once Daily : AntihypertensivesDocument5 pagesTher. Class. PO: (Adults) 5-10 MG Once Daily : AntihypertensivesCliff by the seaNo ratings yet
- Analgesia. Reduction of Inflammation. Reduction of Fever. Decreased Incidence of Transient Ischemic Attacks and MIDocument2 pagesAnalgesia. Reduction of Inflammation. Reduction of Fever. Decreased Incidence of Transient Ischemic Attacks and MICliff by the seaNo ratings yet
- Vocational Dairy Training CourseDocument65 pagesVocational Dairy Training Coursevinu666No ratings yet
- Uterine CancerDocument2 pagesUterine CancerEllaine JoyceNo ratings yet
- Pathogenesis of Group A Streptococcal InfectionsDocument59 pagesPathogenesis of Group A Streptococcal InfectionsHerdwin Limas IINo ratings yet
- Selection 2the Weird and Wonderful Echidna UpdatedDocument15 pagesSelection 2the Weird and Wonderful Echidna UpdatedShaikha TariqNo ratings yet
- Answers & Solutions: NEET (UG) - 2019Document35 pagesAnswers & Solutions: NEET (UG) - 2019Gowri ShankarNo ratings yet
- CTE - Vitamin A Deficiency in Insectivorous LizardsDocument7 pagesCTE - Vitamin A Deficiency in Insectivorous LizardsLove Gecko100% (1)
- Broiler Production GuideDocument26 pagesBroiler Production GuideManoa Nagatalevu TupouNo ratings yet
- Talking Stick's Effect on HIV/AIDS Prevention Knowledge and Attitudes in TeenagersDocument7 pagesTalking Stick's Effect on HIV/AIDS Prevention Knowledge and Attitudes in TeenagersbaesootzuNo ratings yet
- Hand Hygiene Basic Steriline 11Document37 pagesHand Hygiene Basic Steriline 11Chika Febriani100% (1)
- Effect of Subclinical Mastitis On Milk Composition in The Kenyan Smallholder Dairy HerdsDocument6 pagesEffect of Subclinical Mastitis On Milk Composition in The Kenyan Smallholder Dairy HerdsHenry OgolaNo ratings yet
- Radiology of The Respiratory System: Dr. Dhanti Erma, SpradDocument115 pagesRadiology of The Respiratory System: Dr. Dhanti Erma, SpradSeri Maria UruhaNo ratings yet
- Nardi 2018Document9 pagesNardi 2018guilhermeverdumNo ratings yet
- 10-01 Skin Grafts, Substitutes and Principles of Flaps-1Document78 pages10-01 Skin Grafts, Substitutes and Principles of Flaps-1Mohamed ShalabiNo ratings yet
- Principles of Demineralization Part 1Document30 pagesPrinciples of Demineralization Part 1Kush PathakNo ratings yet
- Robert QuestDocument39 pagesRobert QuestNational Academies of Science, Engineering, and MedicineNo ratings yet
- Community Acquired PneumoniaDocument7 pagesCommunity Acquired PneumoniaJoshuaOng100% (1)
- Late Pregnancy Bleeding (LPB) : Antepartum Hemorrhage (Aph) Dr. A. MutungiDocument3 pagesLate Pregnancy Bleeding (LPB) : Antepartum Hemorrhage (Aph) Dr. A. Mutungikhadzx100% (2)
- Chemistry Class 12 Project AntacidsDocument13 pagesChemistry Class 12 Project AntacidsTanishka SinghNo ratings yet
- Vaginal Discharge in DogsDocument5 pagesVaginal Discharge in DogsDarmawan Prastyo100% (1)
- UtiDocument41 pagesUtiKetaks MooNo ratings yet
- IACUC Handling and Restraint of Small Laboratory AnimalsDocument3 pagesIACUC Handling and Restraint of Small Laboratory AnimalsFirdaus BillyNo ratings yet