You might also like
- East Anglia: Cambridge (200 Word Limit) Please Upload CV For The Cambridge AFPDocument7 pagesEast Anglia: Cambridge (200 Word Limit) Please Upload CV For The Cambridge AFPYasir Qadhi's Complete Seerah Series0% (1)
- Overview of The Nervous System: OutlineDocument15 pagesOverview of The Nervous System: OutlineYasir Qadhi's Complete Seerah SeriesNo ratings yet
- Needs Assessment MBBS4Document67 pagesNeeds Assessment MBBS4Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Abu Bakr Al-Siddiq Part 2 - Pre-Islam Life & Conversion Story Dr. Yasir QadhiDocument8 pagesAbu Bakr Al-Siddiq Part 2 - Pre-Islam Life & Conversion Story Dr. Yasir QadhiYasir Qadhi's Complete Seerah Series100% (2)
- Abu Bakr Al-Siddiq Part 3 - The Blessings, Battles & Hadith On Abu Bakr Dr. Yasir QadhiDocument9 pagesAbu Bakr Al-Siddiq Part 3 - The Blessings, Battles & Hadith On Abu Bakr Dr. Yasir QadhiYasir Qadhi's Complete Seerah Series100% (2)
- ABC of DermatologyDocument149 pagesABC of DermatologyAndreea Alexandru100% (14)
- Best Tract SummaryDocument38 pagesBest Tract Summarynon_zenseNo ratings yet
- Seerah 104 - The 1st Rightful Khalifah of Islam Part 2 Election of Abu Bakr - DR Yasir QadhiDocument8 pagesSeerah 104 - The 1st Rightful Khalifah of Islam Part 2 Election of Abu Bakr - DR Yasir QadhiYasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 97 - Maria The Copt & Death of Ibrahim - Dr. Yasir Qadhi - 19th Nov 2014Document7 pagesSeerah of Prophet Muhammad 97 - Maria The Copt & Death of Ibrahim - Dr. Yasir Qadhi - 19th Nov 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of The Prophet Muhammad PBUH by Yasir Qadhi - Compilation of The Entire SeriesDocument776 pagesSeerah of The Prophet Muhammad PBUH by Yasir Qadhi - Compilation of The Entire SeriesYasir Qadhi's Complete Seerah Series96% (78)
- Abu Bakr Al-Siddiq The Successor of The Prophet - Part 1 Family Background Dr. Yasir QadhiDocument7 pagesAbu Bakr Al-Siddiq The Successor of The Prophet - Part 1 Family Background Dr. Yasir QadhiYasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 98 - Marital Dispute With The Wives - Dr. Yasir Qadhi - 3rd December 2014Document8 pagesSeerah of Prophet Muhammad 98 - Marital Dispute With The Wives - Dr. Yasir Qadhi - 3rd December 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 101 - The Death of Prophet Muhammad Dr. Yasir Qadhi 24th Jan 2015Document14 pagesSeerah of Prophet Muhammad 101 - The Death of Prophet Muhammad Dr. Yasir Qadhi 24th Jan 2015Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah 103 - The 1st Rightful Khalifah of Islam Part 1 Incident of The Scrolls - DR Yasir QadhiDocument4 pagesSeerah 103 - The 1st Rightful Khalifah of Islam Part 1 Incident of The Scrolls - DR Yasir QadhiYasir Qadhi's Complete Seerah Series100% (2)
- Seerah of Prophet Muhammad 100 - The Farewell Hajj - Dr. Yasir Qadhi - 21st January 2015Document12 pagesSeerah of Prophet Muhammad 100 - The Farewell Hajj - Dr. Yasir Qadhi - 21st January 2015Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 92 - Battle of Tabuk 5 Dr. Yasir Qadhi 15th October 2014Document8 pagesSeerah of Prophet Muhammad 92 - Battle of Tabuk 5 Dr. Yasir Qadhi 15th October 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 99 - Verse of Sword & Hajj of Abu Bakr - Dr. Yasir Qadhi - 10th Dec 2014Document9 pagesSeerah of Prophet Muhammad 99 - Verse of Sword & Hajj of Abu Bakr - Dr. Yasir Qadhi - 10th Dec 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 96 - The Year of Delegations - Part 3 Dr. Yasir Qadhi - 12th Nov 2014Document8 pagesSeerah of Prophet Muhammad 96 - The Year of Delegations - Part 3 Dr. Yasir Qadhi - 12th Nov 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 87 - Battle of Tabuk 1 - Dr. Yasir Qadhi 20th August 2014Document7 pagesSeerah of Prophet Muhammad 87 - Battle of Tabuk 1 - Dr. Yasir Qadhi 20th August 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 95 - The Year of Delegations - Part 2 Dr. Yasir Qadhi 5th Nov 2014Document7 pagesSeerah of Prophet Muhammad 95 - The Year of Delegations - Part 2 Dr. Yasir Qadhi 5th Nov 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 94 - The Year of Delegations - Part 1 Dr. Yasir Qadhi 29th Oct 2014Document6 pagesSeerah of Prophet Muhammad 94 - The Year of Delegations - Part 1 Dr. Yasir Qadhi 29th Oct 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 85 - Miracles of Prophet Muhammad Dr. Yasir Qadhi 28th May 2014Document10 pagesSeerah of Prophet Muhammad 85 - Miracles of Prophet Muhammad Dr. Yasir Qadhi 28th May 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 89 - Story of Ka'b B. Malik Dr. Yasir Qadhi 3rd September 2014Document8 pagesSeerah of Prophet Muhammad 89 - Story of Ka'b B. Malik Dr. Yasir Qadhi 3rd September 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 93 - Tafsir of Surat At-Tawbah & Tabuk Dr. Yasir Qadhi 22nd Oct 2014Document9 pagesSeerah of Prophet Muhammad 93 - Tafsir of Surat At-Tawbah & Tabuk Dr. Yasir Qadhi 22nd Oct 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammed 91 - Battle of Tabuk 4 - Dr. Yasir Qadhi 17th September 2014Document7 pagesSeerah of Prophet Muhammed 91 - Battle of Tabuk 4 - Dr. Yasir Qadhi 17th September 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 90 - Battle of Tabuk 3 Dr. Yasir Qadhi 10th September 2014Document8 pagesSeerah of Prophet Muhammad 90 - Battle of Tabuk 3 Dr. Yasir Qadhi 10th September 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 88 - Battle of Tabuk 2 Dr. Yasir Qadhi 27th August 2014Document7 pagesSeerah of Prophet Muhammad 88 - Battle of Tabuk 2 Dr. Yasir Qadhi 27th August 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 84 - Conversion of Ka'b Ibn Zuhayr Dr. Yasir Qadhi 7th May 2014Document7 pagesSeerah of Prophet Muhammad 84 - Conversion of Ka'b Ibn Zuhayr Dr. Yasir Qadhi 7th May 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Seerah of Prophet Muhammad 86 - Recap & Lessons From Hunayn & Ta'if Dr. Yasir Qadhi 13 Aug 2014Document8 pagesSeerah of Prophet Muhammad 86 - Recap & Lessons From Hunayn & Ta'if Dr. Yasir Qadhi 13 Aug 2014Yasir Qadhi's Complete Seerah SeriesNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Adrenergic Drugs Classification and UsesDocument2 pagesAdrenergic Drugs Classification and UsesSunshine_Bacla_4275No ratings yet
- LASIK Eye Surgery Free Consumer GuideDocument8 pagesLASIK Eye Surgery Free Consumer GuideJohn SusonNo ratings yet
- CGHS Rates 2014 - AhmadabadDocument72 pagesCGHS Rates 2014 - AhmadabadJayakrishna ReddyNo ratings yet
- Optical Correction of Aphakia in Children: Review ArticleDocument12 pagesOptical Correction of Aphakia in Children: Review Articleaisa mutiaraNo ratings yet
- TTM As5000brochureDocument12 pagesTTM As5000brochureAphichetNo ratings yet
- LaryngoceleDocument7 pagesLaryngoceleM Grecu CeptureanuNo ratings yet
- NCP Epidural HemDocument32 pagesNCP Epidural HemKatrina PonceNo ratings yet
- SD HospitalDocument2 pagesSD HospitalSam PowelNo ratings yet
- Closed Tibia and Fibula Fractures in 44-Year-Old Male PatientDocument25 pagesClosed Tibia and Fibula Fractures in 44-Year-Old Male Patientleonard0% (1)
- Focus ChartingDocument46 pagesFocus ChartingIsmail Alnemr100% (5)
- Medical Prioritization ProcessDocument20 pagesMedical Prioritization ProcessIGDNo ratings yet
- Treating Paranoid OrganizationDocument6 pagesTreating Paranoid Organizationredpsych103100% (2)
- Leonard Lawrence Statement To General Medical CouncilDocument6 pagesLeonard Lawrence Statement To General Medical CouncilgranitoNo ratings yet
- ESAS - Edmonton Symptom Assessment SystemDocument4 pagesESAS - Edmonton Symptom Assessment Systemkamenrider belalangtempurNo ratings yet
- Epilepsy PresentationDocument10 pagesEpilepsy Presentationapi-346838508No ratings yet
- Oral Versus Topical NSAIDs in Rheumatic DiseasesDocument21 pagesOral Versus Topical NSAIDs in Rheumatic DiseasesAnonymous so6ZnlKywNo ratings yet
- Cprmse SCCLDocument18 pagesCprmse SCCLRavi Kumar DukkipatiNo ratings yet
- AXR PresentationDocument30 pagesAXR PresentationLalit KumarNo ratings yet
- Dorothy M. Adcock, MDDocument4 pagesDorothy M. Adcock, MDพอ วิดNo ratings yet
- Nerve Entrapment - UpdateDocument17 pagesNerve Entrapment - UpdatealobrienNo ratings yet
- Updated Resume Kelly oDocument2 pagesUpdated Resume Kelly oapi-254046653No ratings yet
- Vincent Mosca - Clubfoot Guide For ParentsDocument3 pagesVincent Mosca - Clubfoot Guide For ParentsCatalin FloreaNo ratings yet
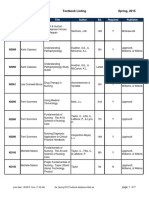
- BFLSON Course Textbook ListingDocument7 pagesBFLSON Course Textbook ListingWina ViqaNo ratings yet
- Current JobsDocument24 pagesCurrent JobsFatima SajidNo ratings yet
- Twin Block 3Document2 pagesTwin Block 3GisselaMaldonadoNo ratings yet
- ICU LogbookDocument37 pagesICU Logbookrinus5100% (1)
- Borgstein ENTbookDocument191 pagesBorgstein ENTbookdokhenNo ratings yet
- A Clinical Decision Support Framework ForDocument5 pagesA Clinical Decision Support Framework FordineshshaNo ratings yet
- Case Study SLDocument5 pagesCase Study SLCharmie Mei Paredes-RoqueNo ratings yet