You might also like
- AnophthalmiaDocument6 pagesAnophthalmialeny zabidiNo ratings yet
- Anotia/Microtia: Minnesota Department of Health Fact Sheet November 2005Document3 pagesAnotia/Microtia: Minnesota Department of Health Fact Sheet November 2005Carlos Santiago VivenzaNo ratings yet
- Pediatrics 2003 Cunningham 436 40Document7 pagesPediatrics 2003 Cunningham 436 40Putu Agus GrantikaNo ratings yet
- Thesis On Birth DefectsDocument6 pagesThesis On Birth Defectsafloblnpeewxby100% (2)
- Thesis Statement For Birth DefectsDocument6 pagesThesis Statement For Birth Defectsashleygomezalbuquerque100% (2)
- Fetal Alcohol Exposure: Birth Fetus Teratogen Prenatal Diagnosis Genetic Vitamin Glucose OvulationDocument9 pagesFetal Alcohol Exposure: Birth Fetus Teratogen Prenatal Diagnosis Genetic Vitamin Glucose OvulationyoaaryanNo ratings yet
- Hearing Screening Pediatrics 2009Document14 pagesHearing Screening Pediatrics 2009Francisco ValleNo ratings yet
- HSC 430 Childhood Disease PaperDocument10 pagesHSC 430 Childhood Disease Paperapi-502687231No ratings yet
- Ismail 25 5Document6 pagesIsmail 25 5Shivani DubeyNo ratings yet
- Newborn Hearing ScreeningDocument3 pagesNewborn Hearing ScreeningHamam KusumaganiNo ratings yet
- Congenital MalformationsDocument20 pagesCongenital Malformationsnsrafel0No ratings yet
- Cerebral Palsy and The Effects On The Oral Cavity: Jessica Heberlie Dhyg Iv - L. HeblDocument7 pagesCerebral Palsy and The Effects On The Oral Cavity: Jessica Heberlie Dhyg Iv - L. Heblapi-546773895No ratings yet
- ECC and Nursing InterventionsDocument8 pagesECC and Nursing Interventionssaima anwarNo ratings yet
- DownloadDocument11 pagesDownloadhasan nazzalNo ratings yet
- Chrisanthopoulos Marika 300453 Cleft Lip and PalateDocument14 pagesChrisanthopoulos Marika 300453 Cleft Lip and PalateCharles IppolitoNo ratings yet
- Neonatal Tooth With Riga-Fide Disease Affecting Breastfeeding: A Case ReportDocument4 pagesNeonatal Tooth With Riga-Fide Disease Affecting Breastfeeding: A Case ReportbanyubiruNo ratings yet
- Holistic Nutrition: Inside OutDocument39 pagesHolistic Nutrition: Inside OutpasinNo ratings yet
- Introduction To English For Law (TLE 0813)Document11 pagesIntroduction To English For Law (TLE 0813)ilham naylaNo ratings yet
- Kelainan BawaanDocument111 pagesKelainan BawaanrinafanesNo ratings yet
- Special Needs Research PaperDocument9 pagesSpecial Needs Research Paperapi-663276816No ratings yet
- Paediatric Guidelines Oral Injury in Young ChildrenDocument2 pagesPaediatric Guidelines Oral Injury in Young Childrenrare781No ratings yet
- Maximizing Auditory SlidesDocument18 pagesMaximizing Auditory SlidesARUNGREESMANo ratings yet
- Bab IDocument5 pagesBab IWahyu Eka WidiantyNo ratings yet
- Abstract 1Document5 pagesAbstract 1api-643672878No ratings yet
- Early Childhood Caries (ECC) : Allison Restauri, RDH, BSDH EDU 653 1 1 - 0 3 - 2 0 1 2Document25 pagesEarly Childhood Caries (ECC) : Allison Restauri, RDH, BSDH EDU 653 1 1 - 0 3 - 2 0 1 2Justforkiddslaserdental ChNo ratings yet
- Cerebral Palsy Research PaperDocument7 pagesCerebral Palsy Research Paperapi-663723303No ratings yet
- Early Childhood Caries (ECC) and Neglect in Child Care: Analysis of An Italian SampleDocument8 pagesEarly Childhood Caries (ECC) and Neglect in Child Care: Analysis of An Italian SampleMohammad Nor AnwarNo ratings yet
- Written Assignment 1Document5 pagesWritten Assignment 1api-401934380No ratings yet
- Maternal Caries Experience Influences Offspring's Early Childhood Caries-A Birth Cohort StudyDocument9 pagesMaternal Caries Experience Influences Offspring's Early Childhood Caries-A Birth Cohort StudyAkhila ReddyNo ratings yet
- US Surgeons Remove Huge Tumor Off Haitian Girl's FaceDocument5 pagesUS Surgeons Remove Huge Tumor Off Haitian Girl's Faceapi-26570979No ratings yet
- Newborn Screening Saves LivesDocument14 pagesNewborn Screening Saves LivesSheilah Mae PadallaNo ratings yet
- Upper and Lower Limb Reduction DefectsDocument5 pagesUpper and Lower Limb Reduction DefectsAnonymous MWd5UOUuiyNo ratings yet
- Omamuli Congenital Limb AbnormalitiesDocument11 pagesOmamuli Congenital Limb Abnormalitiesfrank davidNo ratings yet
- Explain Why Some Mothers Lose Their Tooth/teeth Because of Multi-Pregnancy? Please Cite Some Concrete Evidences. (20 Points)Document2 pagesExplain Why Some Mothers Lose Their Tooth/teeth Because of Multi-Pregnancy? Please Cite Some Concrete Evidences. (20 Points)Luis Gatchalian LacanilaoNo ratings yet
- Health Problems in AdolescentsDocument32 pagesHealth Problems in AdolescentsToyour EternityNo ratings yet
- David's Presentation On Congenital Limb Anomlies - Docx 23Document11 pagesDavid's Presentation On Congenital Limb Anomlies - Docx 23frank davidNo ratings yet
- Care of The Patient With Congenital Anomalies 3Document60 pagesCare of The Patient With Congenital Anomalies 3ladydianamacNo ratings yet
- MeningomyeloceleDocument42 pagesMeningomyeloceleSundaraBharathiNo ratings yet
- South University Tampa PA Interview Article PDFDocument6 pagesSouth University Tampa PA Interview Article PDFsteinway007No ratings yet
- Oral Health 1-3&5Document38 pagesOral Health 1-3&5Umar FarouqNo ratings yet
- HearinglossfactsheetDocument2 pagesHearinglossfactsheetapi-239968581No ratings yet
- Ome 2004Document20 pagesOme 2004Novy Sylvia WardanaNo ratings yet
- Faktor Tumbang (English)Document3 pagesFaktor Tumbang (English)Dwi Puji AstutiNo ratings yet
- Jo CPD 2023011901Document6 pagesJo CPD 2023011901vinayakamagazineshousepvtltdNo ratings yet
- Critical Care Nursing ClinicsDocument133 pagesCritical Care Nursing ClinicsJune DumdumayaNo ratings yet
- Genetic Evaluation For Craniofacial ConditionsDocument21 pagesGenetic Evaluation For Craniofacial ConditionsMarcela Cano RicardoNo ratings yet
- Prevalence of The Cleft Lip and Palate Among Newborn Babies in Sulaimani Obstetrics and Gynecological HospitalDocument3 pagesPrevalence of The Cleft Lip and Palate Among Newborn Babies in Sulaimani Obstetrics and Gynecological HospitalIOSRjournalNo ratings yet
- Thornley Et Al 2020 Fatores Associados ECC Coorte IJPDDocument26 pagesThornley Et Al 2020 Fatores Associados ECC Coorte IJPDNajara RodriguesNo ratings yet
- Pediatric Nursing - Early Childhood Caries Risk Factors and Prevention StrategiesDocument1 pagePediatric Nursing - Early Childhood Caries Risk Factors and Prevention StrategiesLjubomirErdoglijaNo ratings yet
- Down Syndrome (Case Presentation Output)Document6 pagesDown Syndrome (Case Presentation Output)Jommel Ryan Corpus LumibaoNo ratings yet
- Research Paper The Association Between Prenatal Smoking and Hypodontia Linda Morelos Kaylee HughesDocument8 pagesResearch Paper The Association Between Prenatal Smoking and Hypodontia Linda Morelos Kaylee Hughesapi-567500877No ratings yet
- Medical Management of Children With Down SyndromeDocument8 pagesMedical Management of Children With Down SyndromeMariana OrozcoNo ratings yet
- CDC Birth Defects Affect 1 in 33 BabiesDocument4 pagesCDC Birth Defects Affect 1 in 33 BabiesTessa Safitri KotoNo ratings yet
- Jurnal Kesehatan Gigi: Dental Treatment Consideration in Pregnant WomenDocument8 pagesJurnal Kesehatan Gigi: Dental Treatment Consideration in Pregnant WomenindahNo ratings yet
- What is GastroschisisDocument6 pagesWhat is GastroschisisAnonymous MWd5UOUuiyNo ratings yet
- Newborns Hearing Screening Methods ComparedDocument13 pagesNewborns Hearing Screening Methods ComparedCitra LyadhaNo ratings yet
- Health Brochure Comprehensive OverviewDocument12 pagesHealth Brochure Comprehensive Overviewعبدالرحمن سالم بن مخاشنNo ratings yet
- Viewer Question: Doctor's Response:: Definition of Urinary Tract Infection in ChildrenDocument6 pagesViewer Question: Doctor's Response:: Definition of Urinary Tract Infection in ChildrenFrizky Ronald Tua MarbunNo ratings yet
- Managing Common Aches and Pains in Kids: A Parent's Handbook: Health, #9From EverandManaging Common Aches and Pains in Kids: A Parent's Handbook: Health, #9No ratings yet
- Paediatric Dentistry for the General Dental PractitionerFrom EverandPaediatric Dentistry for the General Dental PractitionerSondos AlbadriNo ratings yet
- Apps and Website Link For Nutrimet Course 27 NovDocument1 pageApps and Website Link For Nutrimet Course 27 NovAnonymous MWd5UOUuiyNo ratings yet
- Fenton2013 Preterm Growth Chart (Girls)Document2 pagesFenton2013 Preterm Growth Chart (Girls)Anonymous MWd5UOUuiyNo ratings yet
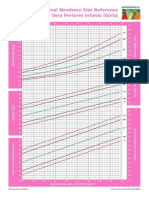
- Intergrowth21 Newborn Size Reference Charts (Girls)Document2 pagesIntergrowth21 Newborn Size Reference Charts (Girls)Anonymous MWd5UOUuiyNo ratings yet
- Upper and Lower Limb Reduction DefectsDocument5 pagesUpper and Lower Limb Reduction DefectsAnonymous MWd5UOUuiyNo ratings yet
- Jadwal Dokter AnakDocument1 pageJadwal Dokter AnakAnonymous MWd5UOUuiyNo ratings yet
- International Postnatal Growth Standards For Preterm Infants (Girls)Document2 pagesInternational Postnatal Growth Standards For Preterm Infants (Girls)Raji MohanNo ratings yet
- Intergrowth21 Postnatal Growth Standards For Preterm Infants (Boys)Document2 pagesIntergrowth21 Postnatal Growth Standards For Preterm Infants (Boys)Anonymous MWd5UOUuiyNo ratings yet
- Bukti Pelatihan PpraDocument17 pagesBukti Pelatihan PpraAnonymous MWd5UOUuiyNo ratings yet
- Pentingnya CP Di RS Untuk Akses Obat KronisDocument27 pagesPentingnya CP Di RS Untuk Akses Obat KronisAnonymous MWd5UOUuiyNo ratings yet
- What is GastroschisisDocument6 pagesWhat is GastroschisisAnonymous MWd5UOUuiyNo ratings yet
- Diaphragmatic HerniaDocument4 pagesDiaphragmatic HerniaAnonymous MWd5UOUuiyNo ratings yet
- Hypospadias Explained: Birth Defect GuideDocument5 pagesHypospadias Explained: Birth Defect GuideAnonymous MWd5UOUuiyNo ratings yet
- What is Craniosynostosis? Birth Defect ExplainedDocument8 pagesWhat is Craniosynostosis? Birth Defect ExplainedAnonymous MWd5UOUuiyNo ratings yet
- What Are Anotia and Microtia?Document7 pagesWhat Are Anotia and Microtia?Anonymous MWd5UOUuiyNo ratings yet
- Atrial Septal DefectDocument5 pagesAtrial Septal DefectAnonymous MWd5UOUuiyNo ratings yet
- M CHAT R FollowupDocument21 pagesM CHAT R FollowupAnonymous MWd5UOUuiyNo ratings yet
- What Are Anotia and Microtia?Document7 pagesWhat Are Anotia and Microtia?Anonymous MWd5UOUuiyNo ratings yet
- AnencephalyDocument9 pagesAnencephalyAnonymous MWd5UOUuiyNo ratings yet
- Chi Square TestDocument75 pagesChi Square Testdrmsupriya091159100% (1)
- Summary of Powerpoint Presentation On ObesityDocument2 pagesSummary of Powerpoint Presentation On ObesityYolieNo ratings yet
- PDF Lecture 9 Benign Soft Tissue TumorsDocument131 pagesPDF Lecture 9 Benign Soft Tissue TumorsMuhammad Rizqi100% (1)
- Mekanisme Resistensi Antibiotik - 2014Document10 pagesMekanisme Resistensi Antibiotik - 2014ArdieNo ratings yet
- Bacteriophages - Biology and Applns - E. Kutter, A. Sulakvelidze (CRC, 2005) WW PDFDocument485 pagesBacteriophages - Biology and Applns - E. Kutter, A. Sulakvelidze (CRC, 2005) WW PDFMădă Iorga100% (2)
- Non-Mendelian Inheritance Practice ProblemsDocument3 pagesNon-Mendelian Inheritance Practice ProblemsAnonymous 7NT1wDj100% (1)
- The Dark Side of WheatDocument77 pagesThe Dark Side of WheatSayer JiNo ratings yet
- Cerebellar LesionsDocument3 pagesCerebellar LesionsMary100% (1)
- Industrial HealthDocument22 pagesIndustrial HealthPraveen Kumar RNo ratings yet
- Plant Pathogens Principles of Plant PathologyDocument376 pagesPlant Pathogens Principles of Plant PathologyChirag GuptaNo ratings yet
- CH 11 - Study GuideDocument4 pagesCH 11 - Study Guideapi-342334216No ratings yet
- Komplemen Dan SitokinDocument38 pagesKomplemen Dan SitokinBantuinAku KakNo ratings yet
- BAMU B.pharmcy Second Year Syllabus 2007Document37 pagesBAMU B.pharmcy Second Year Syllabus 2007Gajanan VaishnavNo ratings yet
- Genetically Modified Bacteria Treat Digestive DiseaseDocument6 pagesGenetically Modified Bacteria Treat Digestive DiseaseRutba SafdarNo ratings yet
- Hiv-1 Quant PCRDocument62 pagesHiv-1 Quant PCRyousrazeidan1979No ratings yet
- Pharmacology MCQ PebcDocument36 pagesPharmacology MCQ Pebcsnowden1100% (6)
- Maple Syrup Urine DiseaseDocument13 pagesMaple Syrup Urine Diseasenurdann100% (1)
- DNA Profiling Gizmo Student Exploration SheetDocument5 pagesDNA Profiling Gizmo Student Exploration SheetCarter BonesNo ratings yet
- Lab 07 HandoutDocument10 pagesLab 07 HandoutShyNo ratings yet
- Necrotizing FasciitisDocument8 pagesNecrotizing Fasciitishdev1993No ratings yet
- Normal Bone Anatomy and PhysiologyDocument9 pagesNormal Bone Anatomy and PhysiologyElsa GonçalvesNo ratings yet
- Advanced Prostate Cancer: Treatment Advances and Future DirectionsDocument14 pagesAdvanced Prostate Cancer: Treatment Advances and Future DirectionsMishel Rodriguez GuzmanNo ratings yet
- All in One - Espring For New ClientDocument34 pagesAll in One - Espring For New Clientdocuments_diamond01No ratings yet
- AQA B Psychology-Anxiety Disorders - An Introduction To Phobias & ExplanationsDocument5 pagesAQA B Psychology-Anxiety Disorders - An Introduction To Phobias & Explanationswarsan bidarNo ratings yet
- Current Primary Open-Angle Glaucoma Treatments and Future DirectionsDocument13 pagesCurrent Primary Open-Angle Glaucoma Treatments and Future DirectionsBenediktus BayuNo ratings yet
- The Reproductive SystemDocument119 pagesThe Reproductive SystemAshis karmakar100% (10)
- Neurocognitive Tests ExplainedDocument68 pagesNeurocognitive Tests ExplainedShahida Darkhawasti100% (1)
- Clinical Success of Deproteinization in Hypocalcified Amelogenesis ImperfectaDocument7 pagesClinical Success of Deproteinization in Hypocalcified Amelogenesis ImperfectaMelisa GuerraNo ratings yet
- AutoGenomics Intl-AACC, LADocument63 pagesAutoGenomics Intl-AACC, LAmohdkhairNo ratings yet
- Evolution Biology IntroductionDocument22 pagesEvolution Biology IntroductionConstance Viloria100% (1)