You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- 150 Question Labce Quez. 1 PDFDocument87 pages150 Question Labce Quez. 1 PDFadvance ascpNo ratings yet
- Microbiology Practice Test IDocument13 pagesMicrobiology Practice Test ISidharta Chatterjee100% (4)
- Chapter 41 Hematologic ProblemsDocument6 pagesChapter 41 Hematologic ProblemsUSC Upstate Nursing CoachesNo ratings yet
- Assessment of The Hematologic SystemDocument36 pagesAssessment of The Hematologic SystemUSC Upstate Nursing CoachesNo ratings yet
- Case StudyDocument27 pagesCase Studychinnitah15No ratings yet
- Biopharmaceutical LexiconDocument65 pagesBiopharmaceutical Lexiconryu_chile28234No ratings yet
- Communicable Disease ReviewerDocument18 pagesCommunicable Disease ReviewerMicah Jonah Elicaño100% (1)
- Assessment of Hematologic Disorders - Physical AssessmentDocument3 pagesAssessment of Hematologic Disorders - Physical AssessmentUSC Upstate Nursing CoachesNo ratings yet
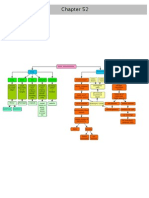
- Ch. 52 Musculoskeletal AssessmentDocument28 pagesCh. 52 Musculoskeletal AssessmentUSC Upstate Nursing CoachesNo ratings yet
- Cheat Sheet RevisedDocument2 pagesCheat Sheet RevisedUSC Upstate Nursing Coaches100% (3)
- Assessment of Hematologic Disorders: Patient HistoryDocument3 pagesAssessment of Hematologic Disorders: Patient HistoryUSC Upstate Nursing CoachesNo ratings yet
- Lupus, Sclerosis, Lymes, Fibromyalgia GoutDocument2 pagesLupus, Sclerosis, Lymes, Fibromyalgia GoutUSC Upstate Nursing CoachesNo ratings yet
- Chapter 52 Bone ClassificationsDocument1 pageChapter 52 Bone ClassificationsUSC Upstate Nursing CoachesNo ratings yet
- Compilation of Class 10.26.10Document13 pagesCompilation of Class 10.26.10USC Upstate Nursing CoachesNo ratings yet
- Musculoskeletal ProblemsDocument12 pagesMusculoskeletal ProblemsUSC Upstate Nursing CoachesNo ratings yet
- Memory Pics: RenalDocument8 pagesMemory Pics: RenalUSC Upstate Nursing CoachesNo ratings yet
- HIV - AIDS, Allergies, AutoimmunityDocument6 pagesHIV - AIDS, Allergies, AutoimmunityUSC Upstate Nursing CoachesNo ratings yet
- Sulfonylurea Agents (Diabinese, Glucotrol, Diabeta) : 2. Meglitinide Analogues (Prandin)Document11 pagesSulfonylurea Agents (Diabinese, Glucotrol, Diabeta) : 2. Meglitinide Analogues (Prandin)Kristin EdwardsNo ratings yet
- Memory Pics Hematology OncologyDocument28 pagesMemory Pics Hematology OncologyKristin EdwardsNo ratings yet
- Memory Pics: MusculoskeletalDocument17 pagesMemory Pics: MusculoskeletalUSC Upstate Nursing CoachesNo ratings yet
- Memory Pics: NeurologicalDocument12 pagesMemory Pics: NeurologicalUSC Upstate Nursing CoachesNo ratings yet
- Memory Pics: SensoryDocument12 pagesMemory Pics: SensoryUSC Upstate Nursing CoachesNo ratings yet
- CH 52: Musculoskeletal Assessment (Per Amendolair)Document27 pagesCH 52: Musculoskeletal Assessment (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- CH 54 AmputationsDocument12 pagesCH 54 AmputationsUSC Upstate Nursing CoachesNo ratings yet
- Chapter 19Document6 pagesChapter 19USC Upstate Nursing CoachesNo ratings yet
- Chapter 21Document4 pagesChapter 21USC Upstate Nursing CoachesNo ratings yet
- CH 53: Musculoskeletal Problems (Per Amendolair)Document32 pagesCH 53: Musculoskeletal Problems (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- Male Reproductive ProblemsDocument6 pagesMale Reproductive ProblemsUSC Upstate Nursing CoachesNo ratings yet
- Interventions For Clients With Hematologic ProblemsDocument50 pagesInterventions For Clients With Hematologic ProblemsUSC Upstate Nursing CoachesNo ratings yet
- CH 54: Musculoskeletal Trauma (Per Amendolair)Document54 pagesCH 54: Musculoskeletal Trauma (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- CH 41: Hematological Assessment (Per Amendolair)Document28 pagesCH 41: Hematological Assessment (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- Chapter 22: Crossword (Per Black)Document3 pagesChapter 22: Crossword (Per Black)USC Upstate Nursing CoachesNo ratings yet
- White Blood Cells (WBC) TotalDocument1 pageWhite Blood Cells (WBC) TotalUSC Upstate Nursing CoachesNo ratings yet
- Experiment 1:: Serial Dilution and Agglutination ReactionDocument35 pagesExperiment 1:: Serial Dilution and Agglutination ReactionJuvial DavidNo ratings yet
- Autoimmunity: Causes, Mechanisms and DiseasesDocument35 pagesAutoimmunity: Causes, Mechanisms and DiseasesFadli FadelNo ratings yet
- Basic Histocompatibility Testing Methods: Kathryn J. TinckamDocument23 pagesBasic Histocompatibility Testing Methods: Kathryn J. TinckamRajitha SiriwardenaNo ratings yet
- Quantitative Flow Cytometry in The Clinical LaboratoryDocument20 pagesQuantitative Flow Cytometry in The Clinical Laboratorykmaher8256No ratings yet
- 5.2 PhysDocument39 pages5.2 PhysshivaniNo ratings yet
- Adel Elkady (Editor) - Infections in Pregnancy - An Evidence-Based Approach-Cambridge University Press (2019)Document216 pagesAdel Elkady (Editor) - Infections in Pregnancy - An Evidence-Based Approach-Cambridge University Press (2019)Putri RamadhaniNo ratings yet
- ANPH M3 CU15. Lymphatic SystemDocument22 pagesANPH M3 CU15. Lymphatic Systemmark tuazonNo ratings yet
- Ih Lec M9 11Document27 pagesIh Lec M9 11m65b6hf9ffNo ratings yet
- Iap Guide Book On Immunization 2009 - 2010Document175 pagesIap Guide Book On Immunization 2009 - 2010bapsamits100% (1)
- Frequencies 171.160 Hz, 174.989 Hz, and 1185.131 Hz may help combat COVID-19Document28 pagesFrequencies 171.160 Hz, 174.989 Hz, and 1185.131 Hz may help combat COVID-19Stere StereNo ratings yet
- How to Infuse HYQVIA with a PumpDocument38 pagesHow to Infuse HYQVIA with a PumpShaya NirenbergNo ratings yet
- General Principles of Microbial Pathogenesis: MicrobiologyDocument5 pagesGeneral Principles of Microbial Pathogenesis: MicrobiologyAbi SulitNo ratings yet
- Microbiology Pangan Ikani 2006Document64 pagesMicrobiology Pangan Ikani 2006Ooy Theboys'saNo ratings yet
- Polimiositis y Dermatomiositis FisiopatologiaDocument13 pagesPolimiositis y Dermatomiositis FisiopatologiaMargarita ChavezNo ratings yet
- Immunology For Pharmacy Students PDFDocument199 pagesImmunology For Pharmacy Students PDFandirio7486No ratings yet
- v170 v174 v175 Flockscreen Ai Instruction For Use v1Document7 pagesv170 v174 v175 Flockscreen Ai Instruction For Use v1Nader SedighiNo ratings yet
- Plasma Physiology (1-2020) by DR Khaled A AbulfadleDocument9 pagesPlasma Physiology (1-2020) by DR Khaled A AbulfadleUzama Binu AliNo ratings yet
- B lymphocyte antibody isotypes guide infection detectionDocument4 pagesB lymphocyte antibody isotypes guide infection detectionMartha LeivaNo ratings yet
- 02 - Classification and Functions of Simple and Complex ProteinsDocument34 pages02 - Classification and Functions of Simple and Complex ProteinselizaviraniNo ratings yet
- Alvarez - 2004 - Integrated Approaches For Detection of Plant Pathogenic Bacteria and Diagnosis of Bacterial DiseasesDocument30 pagesAlvarez - 2004 - Integrated Approaches For Detection of Plant Pathogenic Bacteria and Diagnosis of Bacterial DiseasesJimmy SimpsonNo ratings yet
- Influenza Vaccine StudyDocument61 pagesInfluenza Vaccine StudyFrancheska Nadine MagonciaNo ratings yet
- Modul Eoh3401 PJJ 2016Document162 pagesModul Eoh3401 PJJ 2016Gene RodeNo ratings yet
- AllerjamDocument60 pagesAllerjamgpawankumar@rediffmail.com100% (2)
- Topic 1 Antibody Structure & FunctionDocument56 pagesTopic 1 Antibody Structure & Functionmidhungbabu88No ratings yet
- Krishgen-Coronavirus Catalog v21.09.20Document16 pagesKrishgen-Coronavirus Catalog v21.09.20KRISHGEN BIOSYSTEMSNo ratings yet