You might also like
- Booklet of Osce InformationDocument36 pagesBooklet of Osce InformationKatherine Sullivan100% (1)
- Booklet of Osce InformationDocument36 pagesBooklet of Osce InformationKatherine Sullivan100% (1)
- Booklet of Osce InformationDocument36 pagesBooklet of Osce InformationKatherine Sullivan100% (1)
- Tvl-Ia Automotive Servicing: Quarter 1 - Module 1: Store ManualDocument21 pagesTvl-Ia Automotive Servicing: Quarter 1 - Module 1: Store ManualDarey Reyes100% (2)
- Brinton NietzscheDocument296 pagesBrinton Nietzschej1943No ratings yet
- Adult Learning An OverviewDocument11 pagesAdult Learning An OverviewKhalif AziziNo ratings yet
- Quality of Higher Education in Public and Private Universities in Bangladesh - SubmissionDocument14 pagesQuality of Higher Education in Public and Private Universities in Bangladesh - SubmissionKhondaker Sazzadul Karim67% (3)
- Chenrezig MeditationDocument2 pagesChenrezig MeditationMonge DorjNo ratings yet
- Academic Integrity Issues: Benefits, Challenges, Initiatives and PracticesDocument14 pagesAcademic Integrity Issues: Benefits, Challenges, Initiatives and PracticesGem AmericaNo ratings yet
- Lesson Plan Adjectives Comparative and SuperlativeDocument12 pagesLesson Plan Adjectives Comparative and SuperlativeZeliha TileklioğluNo ratings yet
- NursingDocument10 pagesNursingjames mwangiNo ratings yet
- 1 Hills Beyond A River James Cahill PDFDocument222 pages1 Hills Beyond A River James Cahill PDFLuis Lopez Sanchez100% (1)
- Factors Influencing Students' Choice To Pursue NursingDocument26 pagesFactors Influencing Students' Choice To Pursue NursingAira Shane MargesNo ratings yet
- Gibbs' Reflective Cycle ModelDocument2 pagesGibbs' Reflective Cycle ModelFrancis Obmerga92% (12)
- APC Boosts Polypropylene OperationDocument6 pagesAPC Boosts Polypropylene OperationJuan AlejandroNo ratings yet
- English5 - q1 - Mod2 - Lesson1 - Inferring Meaning of Compound Words Using Context Clues - v3Document20 pagesEnglish5 - q1 - Mod2 - Lesson1 - Inferring Meaning of Compound Words Using Context Clues - v3Wes33% (3)
- Wtg5emp Test Unit 3Document6 pagesWtg5emp Test Unit 3Npt LusoNo ratings yet
- Northwest University Nursing Graduates EmployabilityDocument14 pagesNorthwest University Nursing Graduates EmployabilityMinti BravoNo ratings yet
- Enhancing Learning and Teaching Through Student Feedback in Medical and Health SciencesFrom EverandEnhancing Learning and Teaching Through Student Feedback in Medical and Health SciencesNo ratings yet
- Intro To Marxist Lit Crit Lesson PlanDocument2 pagesIntro To Marxist Lit Crit Lesson Planapi-2828599860% (1)
- s12909 019 1865 7Document8 pagess12909 019 1865 7Vanteamel 25No ratings yet
- Evaluating The Validity of An Integrity-Based Situational Judgement Test For Medical School AdmissionsDocument9 pagesEvaluating The Validity of An Integrity-Based Situational Judgement Test For Medical School Admissionselsy pratama putriNo ratings yet
- Impact of Career Choice Motivation On Academic Burnout in Senior Dental Students: A Cross-Sectional StudyDocument8 pagesImpact of Career Choice Motivation On Academic Burnout in Senior Dental Students: A Cross-Sectional StudyValdimiro LourençoNo ratings yet
- Performance and Attitude of Undergraduate Students of Golestan University of Medical Sciences Towards Cheating in ExamsDocument6 pagesPerformance and Attitude of Undergraduate Students of Golestan University of Medical Sciences Towards Cheating in ExamszahidNo ratings yet
- Jurnal 2Document12 pagesJurnal 2enunzNo ratings yet
- RESEARCH AND UTILIZATION OF FINDINGS IN HIGHER EDUCATIONDocument16 pagesRESEARCH AND UTILIZATION OF FINDINGS IN HIGHER EDUCATIONJonathan Cortez LilangNo ratings yet
- Determinants of Good Academic Performance Among University Students in Ethiopia: A Cross-Sectional StudyDocument9 pagesDeterminants of Good Academic Performance Among University Students in Ethiopia: A Cross-Sectional Studymg generolNo ratings yet
- The Importance of Professional Values From Nursing Students ' PerspectiveDocument7 pagesThe Importance of Professional Values From Nursing Students ' Perspectivecarolinamustapha0No ratings yet
- The Relationship Between Learning Preferences (Styles and Approaches) and Learning Outcomes Among Pre-Clinical Undergraduate Medical StudentsDocument7 pagesThe Relationship Between Learning Preferences (Styles and Approaches) and Learning Outcomes Among Pre-Clinical Undergraduate Medical StudentsCindy JANo ratings yet
- 1 SMDocument9 pages1 SMWigrha Beria PanjaitanNo ratings yet
- Ijebea14 105Document10 pagesIjebea14 105International Association of Scientific Innovations and Research (IASIR)No ratings yet
- Jurnal 8Document9 pagesJurnal 8IRFANNo ratings yet
- Pre-Clerkship Medical Students ' Perceptions of Medical ProfessionalismDocument9 pagesPre-Clerkship Medical Students ' Perceptions of Medical ProfessionalismOliviaNo ratings yet
- Health Services StudyDocument14 pagesHealth Services StudykurukunghuuNo ratings yet
- Survey 1Document10 pagesSurvey 1Najla MohammedNo ratings yet
- JMNPR20230061Document12 pagesJMNPR20230061suryadi suryadiNo ratings yet
- Medical Education - 2022 - Haney - Patients Perspectives On Medical Students Professionalism Blind Spots and PDFDocument12 pagesMedical Education - 2022 - Haney - Patients Perspectives On Medical Students Professionalism Blind Spots and PDFJuanCarlosClaroNo ratings yet
- Jurnal 1Document10 pagesJurnal 1IRFANNo ratings yet
- 2. Undergraduate-level Teaching and Learning (2)Document14 pages2. Undergraduate-level Teaching and Learning (2)Nguyên NguyễnNo ratings yet
- Development of Instrument of Bullying Behaviors in Nursing Education Based On Structured Equation ModelingDocument6 pagesDevelopment of Instrument of Bullying Behaviors in Nursing Education Based On Structured Equation ModelingAmzalmortinNo ratings yet
- Perception Attitude Knowledge and Learning Style PDocument7 pagesPerception Attitude Knowledge and Learning Style PMohibbul HaqueNo ratings yet
- Use of The Social Cognitive Theory To Explain Cheating in College: Implications For Future Health ProfessionalsDocument8 pagesUse of The Social Cognitive Theory To Explain Cheating in College: Implications For Future Health ProfessionalsBRENNETH CANIBELNo ratings yet
- Predictors of Academic Integrity in Occupational Therapy StudentsDocument13 pagesPredictors of Academic Integrity in Occupational Therapy StudentsNataliaNo ratings yet
- Revision_and_validation_of_the_prosocialness_scaleDocument9 pagesRevision_and_validation_of_the_prosocialness_scaleKrishnapriya T SNo ratings yet
- Medical Education - 2015 - Razack - Seeking Inclusion in An Exclusive Process Discourses of Medical School StudentDocument12 pagesMedical Education - 2015 - Razack - Seeking Inclusion in An Exclusive Process Discourses of Medical School StudentoyindamolaogunlanaNo ratings yet
- Self-Efficacy and Clinical Competence of Fourth-Year Nursing Students: A Self-Reported StudyDocument7 pagesSelf-Efficacy and Clinical Competence of Fourth-Year Nursing Students: A Self-Reported StudyissaiahnicolleNo ratings yet
- Chapter 1 Leanne-Rah Inding Bsn3-A - 095557Document8 pagesChapter 1 Leanne-Rah Inding Bsn3-A - 095557Qasra AwaliNo ratings yet
- Unit 6 - Academic Integrity and PlagiarismDocument10 pagesUnit 6 - Academic Integrity and PlagiarismLorraine TaperaNo ratings yet
- Academic Cheating Effect of Student Development ApproachDocument5 pagesAcademic Cheating Effect of Student Development ApproachGuteNo ratings yet
- s12912-023-01470-yDocument9 pagess12912-023-01470-ybenamorhazem746No ratings yet
- Pooja SynopsisDocument11 pagesPooja SynopsispoojaNo ratings yet
- GondarDocument8 pagesGondarYared wolduNo ratings yet
- Professionalism: Plagiarised Letters of Recommendation Submitted For The National Resident Matching ProgramDocument9 pagesProfessionalism: Plagiarised Letters of Recommendation Submitted For The National Resident Matching ProgramUmaNo ratings yet
- SummaryDocument17 pagesSummaryTrang MinhNo ratings yet
- Attitudes About Sickness Presenteeism in Medical Training: Is There A Hidden Curriculum?Document9 pagesAttitudes About Sickness Presenteeism in Medical Training: Is There A Hidden Curriculum?faishal azharNo ratings yet
- Amanda Putri Z-SummarizingDocument4 pagesAmanda Putri Z-SummarizingAmanda putri ZuliantyNo ratings yet
- Sample Study For Correlation DesignDocument9 pagesSample Study For Correlation DesignravenNo ratings yet
- Doctor-Patient Communication Skills: A Survey On Knowledge and Practice of Iranian Family PhysiciansDocument7 pagesDoctor-Patient Communication Skills: A Survey On Knowledge and Practice of Iranian Family PhysiciansBogdan MocreacNo ratings yet
- CVI and CVRDocument9 pagesCVI and CVRchandra yudistira pNo ratings yet
- Cadorin 2017 Instruments Evaluating The Self DirDocument13 pagesCadorin 2017 Instruments Evaluating The Self DirAndrada Marko PoloNo ratings yet
- Chapter 1 3 RevisedDocument23 pagesChapter 1 3 RevisedB E L ANo ratings yet
- Student Nurses Academic Performance Multidimensional ConstructsDocument5 pagesStudent Nurses Academic Performance Multidimensional ConstructsEditor IJTSRDNo ratings yet
- Impact of COVID-19 Pandemic On Dental Academia. Students' Experience in Online Education and Expectations For A Predictable PracticeDocument16 pagesImpact of COVID-19 Pandemic On Dental Academia. Students' Experience in Online Education and Expectations For A Predictable PracticeMatta KongNo ratings yet
- Academic Dishonesty Whose Fault Is It AnywaDocument2 pagesAcademic Dishonesty Whose Fault Is It AnywaAnonymous wGAc8DYl3VNo ratings yet
- Surgical CareerDocument7 pagesSurgical Careermohammadomerkhan96No ratings yet
- The Framework of Systematic Assessment For Resilience (SAR) : Development and ValidationDocument22 pagesThe Framework of Systematic Assessment For Resilience (SAR) : Development and ValidationFaraidoon AminNo ratings yet
- Gamified On Solo (2012-2022)Document10 pagesGamified On Solo (2012-2022)lau dashNo ratings yet
- Determinants of Student LoyaltyDocument13 pagesDeterminants of Student LoyaltyM. NizamNo ratings yet
- UntitledDocument9 pagesUntitledLovelyn VillanuevaNo ratings yet
- How Does COVID 19 Pandemic Inf PDFDocument20 pagesHow Does COVID 19 Pandemic Inf PDFCaren JasonNo ratings yet
- 2021 Zeba Med EduDocument10 pages2021 Zeba Med EduAnupama PathakNo ratings yet
- Jurnal Medical Error PDFDocument8 pagesJurnal Medical Error PDFAidha PutryNo ratings yet
- Chapter 2 Review of Related Literature and Studies PDFDocument6 pagesChapter 2 Review of Related Literature and Studies PDFxjcwzfrifNo ratings yet
- Medsci 06 03 230Document9 pagesMedsci 06 03 230yuriepagayNo ratings yet
- Unila Student EPT Test Results July 2019Document1 pageUnila Student EPT Test Results July 2019Anonymous wGAc8DYl3VNo ratings yet
- Free PPT Templates: Insert The Sub Title of Your PresentationDocument48 pagesFree PPT Templates: Insert The Sub Title of Your PresentationEllo Cannavaro100% (1)
- International Journal of Research & Method in EducationDocument15 pagesInternational Journal of Research & Method in EducationAnonymous wGAc8DYl3VNo ratings yet
- Journal of Oral Biosciences: Honey in Oral Health and Care: A Mini ReviewDocument12 pagesJournal of Oral Biosciences: Honey in Oral Health and Care: A Mini ReviewAnonymous wGAc8DYl3VNo ratings yet
- Assuring The Quality of High-Stakes Undergraduate Assessments of Clinical CompetenceDocument9 pagesAssuring The Quality of High-Stakes Undergraduate Assessments of Clinical CompetenceAnonymous wGAc8DYl3VNo ratings yet
- Simulated and Standardized Patients in Osces: Achievements and Challenges 1992-2003Document9 pagesSimulated and Standardized Patients in Osces: Achievements and Challenges 1992-2003Anonymous wGAc8DYl3VNo ratings yet
- ZX NHSCB SJCDBJMDocument7 pagesZX NHSCB SJCDBJMAnonymous wGAc8DYl3VNo ratings yet
- Teaching Clinical Skills in Developing Countries: Are Clinical Skills Centres The Answer?Document10 pagesTeaching Clinical Skills in Developing Countries: Are Clinical Skills Centres The Answer?Anonymous wGAc8DYl3VNo ratings yet
- The Objective Structured Clinical Examination (OSCE) : AMEE Guide No. 81. Part I: An Historical and Theoretical PerspectiveDocument11 pagesThe Objective Structured Clinical Examination (OSCE) : AMEE Guide No. 81. Part I: An Historical and Theoretical PerspectiveAnonymous wGAc8DYl3VNo ratings yet
- Simulated and Standardized Patients in Osces: Achievements and Challenges 1992-2003Document9 pagesSimulated and Standardized Patients in Osces: Achievements and Challenges 1992-2003Anonymous wGAc8DYl3VNo ratings yet
- Twelve Tips For Organizing An Objective Structured Clinical Examination (OSCE)Document6 pagesTwelve Tips For Organizing An Objective Structured Clinical Examination (OSCE)Anonymous wGAc8DYl3VNo ratings yet
- Assuring The Quality of High-Stakes Undergraduate Assessments of Clinical CompetenceDocument9 pagesAssuring The Quality of High-Stakes Undergraduate Assessments of Clinical CompetenceAnonymous wGAc8DYl3VNo ratings yet
- Objective Structured Clinical Examinations As An Assessment Method in Residency Training Practical ConsiderationsDocument8 pagesObjective Structured Clinical Examinations As An Assessment Method in Residency Training Practical ConsiderationsAnonymous wGAc8DYl3VNo ratings yet
- Skill Based Assessment: ABC of Learning and Teaching in MedicineDocument4 pagesSkill Based Assessment: ABC of Learning and Teaching in MedicineAnonymous wGAc8DYl3VNo ratings yet
- AMEE Guide No 20 The Good Teacher Is More Than A Lecturerð The Twelve Roles of The Teacher PDFDocument14 pagesAMEE Guide No 20 The Good Teacher Is More Than A Lecturerð The Twelve Roles of The Teacher PDFAnonymous wGAc8DYl3VNo ratings yet
- How To Measure The Quality of The OSCE A Review of Metrics - AMEE Guide No. 4Document10 pagesHow To Measure The Quality of The OSCE A Review of Metrics - AMEE Guide No. 4Anonymous wGAc8DYl3VNo ratings yet
- Accreditation Council For Graduate MedicalEducation (ACGME) Milestones-Time For A RevoltDocument2 pagesAccreditation Council For Graduate MedicalEducation (ACGME) Milestones-Time For A RevoltAnonymous wGAc8DYl3VNo ratings yet
- Empathy in Graduate Medical Education Milestones DOIDocument17 pagesEmpathy in Graduate Medical Education Milestones DOIAnonymous wGAc8DYl3VNo ratings yet
- Hubungan Status Gizi Dan Aktivitas Olahraga Dengan Tingkat Kebugaran JasmaniDocument5 pagesHubungan Status Gizi Dan Aktivitas Olahraga Dengan Tingkat Kebugaran JasmaniAnonymous wGAc8DYl3VNo ratings yet
- How To Set Up An OSCEDocument5 pagesHow To Set Up An OSCEAnonymous wGAc8DYl3VNo ratings yet
- Assuring The Quality of High-Stakes Undergraduate Assessments of Clinical CompetenceDocument9 pagesAssuring The Quality of High-Stakes Undergraduate Assessments of Clinical CompetenceAnonymous wGAc8DYl3VNo ratings yet
- Responsible Milestone-Based Educational Handover With Individualized LearningPlan From Undergraduate To Graduate Pediatric Medical EducationDocument10 pagesResponsible Milestone-Based Educational Handover With Individualized LearningPlan From Undergraduate To Graduate Pediatric Medical EducationAnonymous wGAc8DYl3VNo ratings yet
- HSDBCSLK/JDZ ZDocument7 pagesHSDBCSLK/JDZ ZAnonymous wGAc8DYl3V100% (1)
- The Medical Genetics Residency MilestonesDocument4 pagesThe Medical Genetics Residency MilestonesAnonymous wGAc8DYl3VNo ratings yet
- The Medical Genetics Residency MilestonesDocument4 pagesThe Medical Genetics Residency MilestonesAnonymous wGAc8DYl3VNo ratings yet
- ZX NHSCB SJCDBJMDocument7 pagesZX NHSCB SJCDBJMAnonymous wGAc8DYl3VNo ratings yet
- Objective Structured Clinical Examinations As An Assessment Method in Residency Training Practical ConsiderationsDocument8 pagesObjective Structured Clinical Examinations As An Assessment Method in Residency Training Practical ConsiderationsAnonymous wGAc8DYl3VNo ratings yet
- Dr. Atanas Kirjakovski: Social PsychologyDocument33 pagesDr. Atanas Kirjakovski: Social PsychologyAlmirMuratiNo ratings yet
- June Keel Announces RetirementDocument2 pagesJune Keel Announces RetirementDonMashburnNo ratings yet
- Genalyn Puno Cordez Resume for IT Administration PositionDocument4 pagesGenalyn Puno Cordez Resume for IT Administration PositionJay Mark Albis SantosNo ratings yet
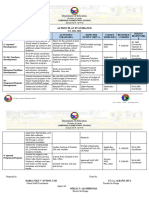
- ACTION PLAN IN GUIDANCE S.Y. 2021-2022Document2 pagesACTION PLAN IN GUIDANCE S.Y. 2021-2022Maria Noly Villotes EntinoNo ratings yet
- Support Vector ClassificationDocument8 pagesSupport Vector Classificationapi-285777244No ratings yet
- Individual Reflection 4Document4 pagesIndividual Reflection 4Urvashi PuraniNo ratings yet
- Ebook PDF Theories of Personality 9th Edition by Jess Feist PDFDocument41 pagesEbook PDF Theories of Personality 9th Edition by Jess Feist PDFflossie.thompson26497% (29)
- Harshal Agrawal - PM ResumeDocument1 pageHarshal Agrawal - PM Resumeapi-354870783No ratings yet
- Left-Handed: Handwriting PagesDocument11 pagesLeft-Handed: Handwriting PagesejoghenetaNo ratings yet
- ACT-R Intro TutorialDocument64 pagesACT-R Intro TutorialSoheil EngineerNo ratings yet
- The Scientific MethodDocument1 pageThe Scientific MethodPaulNo ratings yet
- Premiere Products Exercise Chapter 8 Complete SolutionDocument6 pagesPremiere Products Exercise Chapter 8 Complete SolutionMatthew BeckwithNo ratings yet
- HDC CHÍNH THỨC TIẾNG ANH CHUYÊN 2022Document3 pagesHDC CHÍNH THỨC TIẾNG ANH CHUYÊN 2022Hoàng HuyNo ratings yet
- Handouts IT of Education CompleteDocument523 pagesHandouts IT of Education CompleteNamtu LewanyNo ratings yet
- Individual Project Report On Role of Robotic Process Automation (RPA) in Digital TransformationDocument13 pagesIndividual Project Report On Role of Robotic Process Automation (RPA) in Digital TransformationTest accNo ratings yet
- Daily Lesson Plan 2017/2018 School: Teacher's Name Subject Day / Date Grade/ Class Unit / Lesson Lesson TitleDocument4 pagesDaily Lesson Plan 2017/2018 School: Teacher's Name Subject Day / Date Grade/ Class Unit / Lesson Lesson TitleSHUMAILANo ratings yet
- Student Motivation: Unit - 3Document36 pagesStudent Motivation: Unit - 3RubeenaNo ratings yet
- Social Work NotesDocument4 pagesSocial Work NoteszahidazizNo ratings yet
- Negative Effects of Standardized TestingDocument33 pagesNegative Effects of Standardized TestingmarcaicedoNo ratings yet