You might also like
- Orig UAP Docs 200-208Document85 pagesOrig UAP Docs 200-208Mary Mae JeremiasNo ratings yet
- Securing A Building PermitDocument4 pagesSecuring A Building PermitGenver HoraNo ratings yet
- Health Building Note 00-01 General Design Guidance For Healthcare BuildingsDocument77 pagesHealth Building Note 00-01 General Design Guidance For Healthcare Buildingshashim.mjNo ratings yet
- Mid-Rise Wood Construction GuideDocument44 pagesMid-Rise Wood Construction GuideJosé Eduardo BaravelliNo ratings yet
- CsiDocument9 pagesCsiyamanta_rajNo ratings yet
- HKCICDocument27 pagesHKCICAnonymous 37PvyXCNo ratings yet
- QS RFPDocument16 pagesQS RFPdwivedi.p.kNo ratings yet
- MIT Thesis Guidelines For Kinetic Architecture PDFDocument73 pagesMIT Thesis Guidelines For Kinetic Architecture PDFSamya Rakshit0% (1)
- NEW FGI Residential Guidelines PDFDocument327 pagesNEW FGI Residential Guidelines PDFzahidNo ratings yet
- Upgrading 3311kV Substation - BoQDocument21 pagesUpgrading 3311kV Substation - BoQRicky ChangNo ratings yet
- Ceiling DiffusersDocument21 pagesCeiling DiffusersMonal MuthusamyNo ratings yet
- Plumbing Technology, Design & Installation - Plumbing and MechanicalDocument2 pagesPlumbing Technology, Design & Installation - Plumbing and Mechanicalstaryk0% (1)
- Sustainable Building Technical Manual Part II PDFDocument0 pagesSustainable Building Technical Manual Part II PDFjopaypagasNo ratings yet
- Project Supervision and AdministratioinDocument26 pagesProject Supervision and AdministratioinSIMEON AJULONo ratings yet
- Building Economics: Theory and PracticeDocument13 pagesBuilding Economics: Theory and PracticeVinMohNo ratings yet
- Facilities Standards For The Public Buildings ServiceDocument32 pagesFacilities Standards For The Public Buildings ServicesbrionesNo ratings yet
- Pre-Tender Review: Infrastructure Finance, and Capital Works (IFCW) Quality Checklist Buiding Projects Pre-Tender ReviewDocument16 pagesPre-Tender Review: Infrastructure Finance, and Capital Works (IFCW) Quality Checklist Buiding Projects Pre-Tender ReviewUsman Shahid100% (1)
- Trends in ConstructionDocument12 pagesTrends in ConstructionRoopendraKumar100% (1)
- Specification-Module 1Document6 pagesSpecification-Module 1BaijuNo ratings yet
- Total ( ) /M % of Total: Substructure 2,558,000 120.09 7.40%Document3 pagesTotal ( ) /M % of Total: Substructure 2,558,000 120.09 7.40%pancaekaNo ratings yet
- Fabtech - Cleanroom Modular PanelsDocument6 pagesFabtech - Cleanroom Modular Panelsrasukumar100% (1)
- Checklist For Finishing Activities: Room AreaDocument4 pagesChecklist For Finishing Activities: Room AreaAdnanNo ratings yet
- Building Regulations: Unit 17Document5 pagesBuilding Regulations: Unit 17Brandon WaraNo ratings yet
- Fgi Presentation Mishe Ec 2019-12-13Document46 pagesFgi Presentation Mishe Ec 2019-12-13Kibedi Faisal MenyaNo ratings yet
- ALDAR HQDocument6 pagesALDAR HQpillaiwarmNo ratings yet
- The Complete Guide To Construction Management: Course ManualDocument49 pagesThe Complete Guide To Construction Management: Course ManualJosé Pedro Agonia100% (1)
- Convan Fitout Banatu 5Document2 pagesConvan Fitout Banatu 5Eron ManNo ratings yet
- Globalization of Architectural Practice and World City NetworksDocument10 pagesGlobalization of Architectural Practice and World City NetworksHarneet KaurNo ratings yet
- Project Manager or Construction ManagerDocument4 pagesProject Manager or Construction Managerapi-78915684No ratings yet
- NZ BIM Handbook Project BIM Brief ExampleDocument9 pagesNZ BIM Handbook Project BIM Brief ExampleSaidWebbeNo ratings yet
- Basics of High-Performance Building Design - Sam Hui PDFDocument60 pagesBasics of High-Performance Building Design - Sam Hui PDF185412No ratings yet
- 0932-2 Garage - Pricing Specs 10 - 0517Document674 pages0932-2 Garage - Pricing Specs 10 - 0517blutec13No ratings yet
- Proposed Two Storey Residence ReportDocument27 pagesProposed Two Storey Residence ReportchorgedNo ratings yet
- 02aschematic DesignDocument12 pages02aschematic DesignJasman EsmonNo ratings yet
- HVAC Peak Load Calculation Methods - History and ComparisonsDocument9 pagesHVAC Peak Load Calculation Methods - History and ComparisonsAnonymous 73gEYyEtLNo ratings yet
- Bcin Document DisplayDocument1 pageBcin Document DisplaymasithaNo ratings yet
- Start A New Project: Demolition Floor Plan'Document8 pagesStart A New Project: Demolition Floor Plan'api-412335502No ratings yet
- Germany Guideline SBDocument123 pagesGermany Guideline SBlockas222No ratings yet
- Century City Mall & Retail Design GuidelinesDocument62 pagesCentury City Mall & Retail Design GuidelinesPat RonquilloNo ratings yet
- Conduit LengthDocument3 pagesConduit LengthmanishNo ratings yet
- Engineering Services Guidelines - Sydney PDFDocument130 pagesEngineering Services Guidelines - Sydney PDFFawaaz KhurwolahNo ratings yet
- Ac 001 List of DrawingsDocument1 pageAc 001 List of Drawingswael hassanNo ratings yet
- Core and Shell FacilitiesDocument7 pagesCore and Shell Facilitiesapi-412335502No ratings yet
- Buildcost Construction Cost - Guide 2014Document7 pagesBuildcost Construction Cost - Guide 2014DiaszNo ratings yet
- SLIA PART III Exam - Case - Study - Chapter 01Document12 pagesSLIA PART III Exam - Case - Study - Chapter 01Lakmal GalagodaNo ratings yet
- Building Automation FutureDocument9 pagesBuilding Automation FutureppsatsNo ratings yet
- FDocument19 pagesFFrans van der MerweNo ratings yet
- Classroom Design GuidelinesDocument46 pagesClassroom Design Guidelinesmkrmalathi963No ratings yet
- Trimo FTV Catalog System of Horizontal FacadesDocument24 pagesTrimo FTV Catalog System of Horizontal FacadessertackcdgNo ratings yet
- Cad StandardsDocument18 pagesCad StandardsPat BautistaNo ratings yet
- Case Study 3 Analysis (K Shanika Dilini)Document4 pagesCase Study 3 Analysis (K Shanika Dilini)Shanika Dilini Pathigoda100% (1)
- Improve Site ConstructabilityDocument4 pagesImprove Site ConstructabilitylizaNo ratings yet
- Project Implementation Case Study KPIsDocument15 pagesProject Implementation Case Study KPIsqis qusNo ratings yet
- Preview 66 23 en-CA 0 July 2016 CONSTRUCTION MANUAL With Retail PDFDocument145 pagesPreview 66 23 en-CA 0 July 2016 CONSTRUCTION MANUAL With Retail PDFhosam01No ratings yet
- Section 23 82 19 - Fan Coil UnitsDocument5 pagesSection 23 82 19 - Fan Coil UnitsSaber ElkassasNo ratings yet
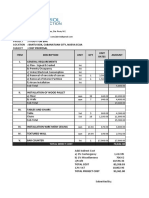
- Item No. Description Quantity: Summary of Financial ProposalDocument14 pagesItem No. Description Quantity: Summary of Financial ProposalmarkalvinbonNo ratings yet
- PA PDF Schedule 12 Design Management PlanDocument18 pagesPA PDF Schedule 12 Design Management PlanbujangmiayamNo ratings yet
- Integrated Farming System: A ReviewDocument12 pagesIntegrated Farming System: A ReviewIndian Journal of Veterinary and Animal Sciences RNo ratings yet
- Laporan OjtDocument77 pagesLaporan OjtDimasQiNo ratings yet
- Drinking Water StandardDocument2 pagesDrinking Water StandardNoorul Mufas Mn100% (1)
- Material Safety Data Sheet "Cut Back Bitumen": Section 1: Product and Company IdentificationDocument4 pagesMaterial Safety Data Sheet "Cut Back Bitumen": Section 1: Product and Company IdentificationPecel LeleNo ratings yet
- Summer's TowerDocument8 pagesSummer's TowerSum SumNo ratings yet
- Myth / Fact: Known and Suspected Terrorists / Special Interest Aliens - Homeland SecurityDocument4 pagesMyth / Fact: Known and Suspected Terrorists / Special Interest Aliens - Homeland SecurityRoger OgdenNo ratings yet
- Cybersecurity Case 4Document1 pageCybersecurity Case 4Gaurav KumarNo ratings yet
- Effects of Job Evaluation On Workers' Productivity: A Study of Ohaukwu Local Government Area, Ebonyi State, NigeriaDocument6 pagesEffects of Job Evaluation On Workers' Productivity: A Study of Ohaukwu Local Government Area, Ebonyi State, Nigeriafrank kipkoechNo ratings yet
- 10 PDFDocument5 pages10 PDFIndira BanerjeeNo ratings yet
- Guerrero vs. CA - DigestDocument2 pagesGuerrero vs. CA - DigestMarionnie SabadoNo ratings yet
- Meltdown: The New Normal Call of The Wild Gear of The YearDocument93 pagesMeltdown: The New Normal Call of The Wild Gear of The YearAppaeommasaranghaeNo ratings yet
- Safety Data Sheet for Anionic Polymer LiquidDocument6 pagesSafety Data Sheet for Anionic Polymer LiquidZi Wei LeongNo ratings yet
- 17 "Flow" Triggers That Will Increase Productivity - Tapping Into Peak Human Performance in BusinessDocument7 pages17 "Flow" Triggers That Will Increase Productivity - Tapping Into Peak Human Performance in BusinessFilipe RovarottoNo ratings yet
- OSI Network Layer ProtocolsDocument29 pagesOSI Network Layer Protocolsa NaniNo ratings yet
- Prateek Chhabra - (C.V.) 22-08Document4 pagesPrateek Chhabra - (C.V.) 22-08PrateekNo ratings yet
- The Piezoelectric EffectDocument10 pagesThe Piezoelectric EffectDmytro RakNo ratings yet
- OBURE Understanding How Reits Market WorksDocument3 pagesOBURE Understanding How Reits Market WorksJohn evansNo ratings yet
- IM-100 IM-202 IM-300 IM-400 IM-500 Operating and Programming - TOCDocument6 pagesIM-100 IM-202 IM-300 IM-400 IM-500 Operating and Programming - TOCRudinHarianto0% (1)
- Ruskin Bond's Haunting Stories CollectionDocument5 pagesRuskin Bond's Haunting Stories CollectionGopal DeyNo ratings yet
- Mid-Term Test RemedialDocument2 pagesMid-Term Test RemedialgaliihputrobachtiarzenNo ratings yet
- Barangay Budget Authorization No. 11Document36 pagesBarangay Budget Authorization No. 11Clarissa PalinesNo ratings yet
- Design InfographicDocument1 pageDesign InfographicHarNo ratings yet
- Partnership Formation EssentialsDocument2 pagesPartnership Formation EssentialsRodolfo ManalacNo ratings yet
- ASTMH Exam Brochure 18 FNLDocument17 pagesASTMH Exam Brochure 18 FNLNgô Khánh HuyềnNo ratings yet
- 947 - Apperntiship Adani Airport - 31-08-2023Document2 pages947 - Apperntiship Adani Airport - 31-08-2023Deep PatelNo ratings yet
- Efficient Three Phase X3-Max Inverters from SolaX for Industrial and Residential UseDocument2 pagesEfficient Three Phase X3-Max Inverters from SolaX for Industrial and Residential UseMuhammad FaruqNo ratings yet
- BITUMINOUS MIX DESIGNDocument4 pagesBITUMINOUS MIX DESIGNSunil BoseNo ratings yet
- Over 20 free and paid Pathfinder 2E character sheet optionsDocument1 pageOver 20 free and paid Pathfinder 2E character sheet optionsravardieresudNo ratings yet
- Best Practices in Non-Revenue Water en FinalDocument96 pagesBest Practices in Non-Revenue Water en FinalEddiemtonga100% (1)
- Minimize audit risk with pre-engagement activitiesDocument2 pagesMinimize audit risk with pre-engagement activitiesAnonymityNo ratings yet