You might also like
- CLINICAL PRESENTATION OF PERITONEAL MESOTHELIOMADocument5 pagesCLINICAL PRESENTATION OF PERITONEAL MESOTHELIOMAmalvina.sekolonik911No ratings yet
- Unusual Variants of Fibroadenoma Breast Diagnosed on CytologyDocument5 pagesUnusual Variants of Fibroadenoma Breast Diagnosed on CytologyEnvhy WinaNo ratings yet
- Mastitis 2Document4 pagesMastitis 2lolytofarisaNo ratings yet
- Primary Angiosarcoma Breast With Intractable ThrombocytopeniaDocument4 pagesPrimary Angiosarcoma Breast With Intractable ThrombocytopeniaMuneer KhalamNo ratings yet
- Dematos 1997Document6 pagesDematos 1997Ali AmokraneNo ratings yet
- EndometriosisDocument17 pagesEndometriosisIngrid HerreraNo ratings yet
- Sick Lobe 12 GöteborgDocument140 pagesSick Lobe 12 GöteborgDima PathNo ratings yet
- Lipoma of The Uterine Corpus Exceptional Eventuality Combined With An Ovarian ThecomaDocument5 pagesLipoma of The Uterine Corpus Exceptional Eventuality Combined With An Ovarian ThecomaAlex HydronNo ratings yet
- Nephroblastoma: Radiological and Pathological Diagnosis of A Case With Liver MetastasesDocument5 pagesNephroblastoma: Radiological and Pathological Diagnosis of A Case With Liver MetastasesfifahcantikNo ratings yet
- MM in PregnancyDocument8 pagesMM in PregnancyIrma YasminNo ratings yet
- 10 1016@j Bpobgyn 2015 11 014Document17 pages10 1016@j Bpobgyn 2015 11 014Marco Julcamoro AsencioNo ratings yet
- Abdominal Inflammatory Myofibroblastic Tumor: Report On Four Cases and Review of LiteratureDocument6 pagesAbdominal Inflammatory Myofibroblastic Tumor: Report On Four Cases and Review of LiteratureLisma EkayantiNo ratings yet
- Kurtz 2016Document5 pagesKurtz 2016Stevano PattiasinaNo ratings yet
- Giant Uterine Leiomyoma - Case Report and Review of LiteratureDocument3 pagesGiant Uterine Leiomyoma - Case Report and Review of LiteratureMan ManuelNo ratings yet
- A Curious Case of Persistent Mullerian Duct Syndrome (PMDS) With Seminoma: A Report of A Rare CaseDocument6 pagesA Curious Case of Persistent Mullerian Duct Syndrome (PMDS) With Seminoma: A Report of A Rare Casecommon 9943No ratings yet
- Cystic Hygroma of The Neck: Single Center Experience and Literature ReviewDocument6 pagesCystic Hygroma of The Neck: Single Center Experience and Literature ReviewLiv InkNo ratings yet
- Mixed Müllerian Tumor of UterusDocument3 pagesMixed Müllerian Tumor of UterusInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Primary Tuberculosis of Breast in 22 Year Old Female - A Rare Case ReportDocument5 pagesPrimary Tuberculosis of Breast in 22 Year Old Female - A Rare Case ReportInternational Organization of Scientific Research (IOSR)No ratings yet
- Diagnosis and Management of Atypical Endometrial HyperplasiaDocument9 pagesDiagnosis and Management of Atypical Endometrial HyperplasiaagathapradanaNo ratings yet
- Art 1Document15 pagesArt 1Nizam Ul MulkNo ratings yet
- En A16v41n4Document3 pagesEn A16v41n4divyanshu kumarNo ratings yet
- Askin TumorDocument6 pagesAskin TumorGaluh Kresna BayuNo ratings yet
- Embryonal Rhabdomyosarcoma of The Uterine Cervix: Two Cases Report and Literature ReviewDocument7 pagesEmbryonal Rhabdomyosarcoma of The Uterine Cervix: Two Cases Report and Literature ReviewPhn StanleyNo ratings yet
- Uterine Fibroid Mimicking Ovarian TumorDocument3 pagesUterine Fibroid Mimicking Ovarian Tumorasshagab04No ratings yet
- Disgerminom OvarianDocument7 pagesDisgerminom OvarianIfrim MihaelaNo ratings yet
- Krukenberg Tumour Simulating Uterine Fibroids and Pelvic Inflammatory DiseaseDocument3 pagesKrukenberg Tumour Simulating Uterine Fibroids and Pelvic Inflammatory DiseaseradianrendratukanNo ratings yet
- Case ReportDocument5 pagesCase ReportLifia VirginiaNo ratings yet
- Eyelid TattoingDocument15 pagesEyelid Tattoing小島隆司No ratings yet
- Rare Association of A c1-c2 Schwannoma in Pregnant Women About A Case and Literature ReviewDocument4 pagesRare Association of A c1-c2 Schwannoma in Pregnant Women About A Case and Literature ReviewCelebre MualabaNo ratings yet
- Breast Abscess Diagnosis and Minimally Invasive TreatmentDocument13 pagesBreast Abscess Diagnosis and Minimally Invasive Treatmentkelvin aidilfitraNo ratings yet
- 1 s2.0 S0015028201029004 MainDocument2 pages1 s2.0 S0015028201029004 MainMika OikuNo ratings yet
- A Case of Giant Uterine Fibroid in A Toung WomanDocument5 pagesA Case of Giant Uterine Fibroid in A Toung WomanTETINOUNo ratings yet
- Faz Zio 2016Document9 pagesFaz Zio 2016seruniallisaaslimNo ratings yet
- Malignant Mixed Mullerian Tumor Arising From The UDocument5 pagesMalignant Mixed Mullerian Tumor Arising From The UAmin IsmailNo ratings yet
- Malignant Mesothelioma Presenting With Unexplained Recurrent Pleurisy EpisodesDocument4 pagesMalignant Mesothelioma Presenting With Unexplained Recurrent Pleurisy EpisodesNurul NingrumNo ratings yet
- Clinical and Morphological Features of Focal AdenomyosisDocument8 pagesClinical and Morphological Features of Focal AdenomyosisAndika FirmantaraNo ratings yet
- ReferatDocument35 pagesReferatYuni AurraNo ratings yet
- Diagnosis in Oncology: UnusualaspectsofbreastcancerDocument5 pagesDiagnosis in Oncology: UnusualaspectsofbreastcancerLìzeth RamìrezNo ratings yet
- MammoDocument58 pagesMammoNaresh GargNo ratings yet
- Ultrasonographic Assessment of Ovarian Endometrioma: Journal of Medical Ultrasound December 2008Document9 pagesUltrasonographic Assessment of Ovarian Endometrioma: Journal of Medical Ultrasound December 2008muhhasanalbolkiah saidNo ratings yet
- Journal: Nursing Leadership and ManagementDocument9 pagesJournal: Nursing Leadership and ManagementdaliaNo ratings yet
- Primary Fibrosarcoma of Breast: A Rare Case Presentation: Cash ReportDocument4 pagesPrimary Fibrosarcoma of Breast: A Rare Case Presentation: Cash ReportBastiaanNo ratings yet
- Evaluation of Breast Masses Using Mammography and Sonography As First Line InvestigationsDocument3 pagesEvaluation of Breast Masses Using Mammography and Sonography As First Line InvestigationsNata SanjayaNo ratings yet
- A Study To Determine Association of Ovarian Morphology With Endometrial Morphology and Postmenopausal BleedingDocument7 pagesA Study To Determine Association of Ovarian Morphology With Endometrial Morphology and Postmenopausal Bleedingmadhu chaturvediNo ratings yet
- Imaging Features and Diagnosis of Tuberculosis of The BreastDocument6 pagesImaging Features and Diagnosis of Tuberculosis of The Breastdmaja duluuuNo ratings yet
- Pinacetal Primary Uterine AngiosarcomaDocument3 pagesPinacetal Primary Uterine AngiosarcomaIlincaNo ratings yet
- Ad en Om Yo SisDocument6 pagesAd en Om Yo SisMariaa EndahhNo ratings yet
- AbstractDocument1 pageAbstractDerevie Hendryan MoulinaNo ratings yet
- IOSR Journal of Pharmacy (IOSRPHR)Document4 pagesIOSR Journal of Pharmacy (IOSRPHR)IOSR Journal of PharmacyNo ratings yet
- Giant Malignant Phyllodes Tumor of the Breast Case ReportDocument5 pagesGiant Malignant Phyllodes Tumor of the Breast Case Reportsiti qomaria usuNo ratings yet
- Transvaginal Sonography and The Diagnosis of Adenomyosis: Col (DR) Hanifullah KhanDocument8 pagesTransvaginal Sonography and The Diagnosis of Adenomyosis: Col (DR) Hanifullah KhanJilleanneNo ratings yet
- Imaging Features of Postpartum Uterine Rupture: A Case ReportDocument4 pagesImaging Features of Postpartum Uterine Rupture: A Case ReportSadam_fasterNo ratings yet
- EJHM - Volume 89 جامعه الزقازيقDocument9 pagesEJHM - Volume 89 جامعه الزقازيقفاطمة الزهراء أسامةNo ratings yet
- Jin-Young Lee, Dae-Bong Kim, Beom Seok Kwak,* 김어진**: Primary fibrosarcoma of the breast: a case reportDocument12 pagesJin-Young Lee, Dae-Bong Kim, Beom Seok Kwak,* 김어진**: Primary fibrosarcoma of the breast: a case reporteosfieldNo ratings yet
- Massa OavriumDocument3 pagesMassa OavriumAde Gustina SiahaanNo ratings yet
- Gupta 37.7Document38 pagesGupta 37.7Oscar NogueraNo ratings yet
- Ultrasonographic Features of Tuberculous Cervical LymphadenitisDocument6 pagesUltrasonographic Features of Tuberculous Cervical LymphadenitisAisahNo ratings yet
- Stem Cell OsteosarcomaDocument5 pagesStem Cell OsteosarcomaHendrikus Surya Adhi PutraNo ratings yet
- Primary Umbilical Endometriosis. Case Report and Discussion On Management OptionsDocument7 pagesPrimary Umbilical Endometriosis. Case Report and Discussion On Management Optionsari naNo ratings yet
- Diagnosis of Endometrial Biopsies and Curettings: A Practical ApproachFrom EverandDiagnosis of Endometrial Biopsies and Curettings: A Practical ApproachNo ratings yet
- Statement Letter TKDN EnglishDocument1 pageStatement Letter TKDN English"/tmp/upload/b7ba6c5935afd58a114d8ff5e467b9faecf0fc5a60b6599e95ec2666920612624/DSC00025.JPG"0% (1)
- Program Error SistemDocument1 pageProgram Error Sistem"/tmp/upload/b7ba6c5935afd58a114d8ff5e467b9faecf0fc5a60b6599e95ec2666920612624/DSC00025.JPG"No ratings yet
- Semiology - Witness To A SeizureDocument19 pagesSemiology - Witness To A Seizure"/tmp/upload/b7ba6c5935afd58a114d8ff5e467b9faecf0fc5a60b6599e95ec2666920612624/DSC00025.JPG"No ratings yet
- GoutDocument15 pagesGout"/tmp/upload/b7ba6c5935afd58a114d8ff5e467b9faecf0fc5a60b6599e95ec2666920612624/DSC00025.JPG"No ratings yet
- HepatitisDocument55 pagesHepatitisIdiAmadouNo ratings yet
- Critical Reflection Directions and TemplateDocument2 pagesCritical Reflection Directions and TemplateMary LowryNo ratings yet
- Vaccines For Corona Virus Project-1Document28 pagesVaccines For Corona Virus Project-1Ananya PuhanNo ratings yet
- Update Otitis Externa AkutDocument7 pagesUpdate Otitis Externa AkutreyhanrrNo ratings yet
- Celiac Disease: Suggestive Gastrointestinal SymptomsDocument6 pagesCeliac Disease: Suggestive Gastrointestinal SymptomsJean Pierre FakhouryNo ratings yet
- EudraCT Protocol Related Data DictionaryDocument412 pagesEudraCT Protocol Related Data DictionaryremovableNo ratings yet
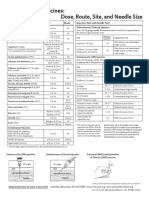
- Injection Site and Needle Size Vaccine Dose RouteDocument1 pageInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaNo ratings yet
- BG Group Standard Health Management BG-ST-HR-SER-004 (HSSE Management System Framework Section 9.1.3)Document18 pagesBG Group Standard Health Management BG-ST-HR-SER-004 (HSSE Management System Framework Section 9.1.3)Sunday Augustine ChibuzoNo ratings yet
- Food & Nutrient Intervention - Specific CVCBDocument52 pagesFood & Nutrient Intervention - Specific CVCBSiti Ika FitrasyahNo ratings yet
- Capstone OutlineDocument3 pagesCapstone Outlineapi-395468231No ratings yet
- Jessica Hernandez CV 2018Document3 pagesJessica Hernandez CV 2018api-441430695No ratings yet
- HPV: Infection, Prevention and Vaccination in India: Ritesh KumarDocument6 pagesHPV: Infection, Prevention and Vaccination in India: Ritesh Kumarsandeep raiNo ratings yet
- Priyanshu - Sarkar - Project Report On Internship ProgramDocument25 pagesPriyanshu - Sarkar - Project Report On Internship ProgramLog InNo ratings yet
- Module 3 - Nursing Assessment in Family Nursing PracticeDocument7 pagesModule 3 - Nursing Assessment in Family Nursing PracticeRogedith DelaRosaNo ratings yet
- UK Patient Metoclopramide Medication LeafletDocument3 pagesUK Patient Metoclopramide Medication Leafletmarisa apriliaNo ratings yet
- Kaiser Ultimate Health Builder Plan provides lifetime healthcareDocument12 pagesKaiser Ultimate Health Builder Plan provides lifetime healthcareLloyd Leonell LabsoNo ratings yet
- Ugaiet2011brochure - PDF KleDocument59 pagesUgaiet2011brochure - PDF Klezuber2022No ratings yet
- Breast Cancer Concept MapDocument2 pagesBreast Cancer Concept MapMaria Cristina100% (1)
- Skill Checklist Using Personal Protective EquipmentDocument2 pagesSkill Checklist Using Personal Protective EquipmentAsep BageurNo ratings yet
- PhenylketonuriaDocument10 pagesPhenylketonuriaMalathy Ravendran100% (1)
- Handwashing Poster PresentationDocument1 pageHandwashing Poster Presentationapi-372418362100% (1)
- Abdominal Distention inDocument45 pagesAbdominal Distention inArif Rahman DmNo ratings yet
- Malaysia PRP Private Hospital LogbookDocument229 pagesMalaysia PRP Private Hospital LogbookAiWeiNo ratings yet
- Sources of Drug InformationDocument36 pagesSources of Drug InformationCristine ChubiboNo ratings yet
- Drug Proving Project InvestigationsDocument8 pagesDrug Proving Project InvestigationsJayNo ratings yet
- Focal Infection Theory: A Focus On Current AspectsDocument7 pagesFocal Infection Theory: A Focus On Current AspectsDiandra Puspa WidyasariNo ratings yet
- Nursing Assessment: 4 StepsDocument2 pagesNursing Assessment: 4 StepsCOLEGIO SOCIEDAD PEDAGOGICA PARA INFANTESNo ratings yet
- A Myth About Anastomotic LeakDocument3 pagesA Myth About Anastomotic LeakAvinash RoyNo ratings yet
- CV Maggies - HungDocument4 pagesCV Maggies - HungDoni HardiansyahNo ratings yet
- Enovate Biolife PortfolioDocument8 pagesEnovate Biolife PortfolioShilpa KhadilkarNo ratings yet
- New Roles Pharmacists: Value-Based Pay Creates OpportunitiesDocument33 pagesNew Roles Pharmacists: Value-Based Pay Creates OpportunitiesAnonymous EAPbx6No ratings yet