You might also like
- Antiarrhythmic DrugsDocument116 pagesAntiarrhythmic DrugsJASMEEN RAVALNo ratings yet
- ACLS PrecourseAssessmentDocument19 pagesACLS PrecourseAssessmentBrigitte Elaine81% (21)
- Atrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesFrom EverandAtrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesRating: 4 out of 5 stars4/5 (1)
- Antiarrhythmic DrugsDocument21 pagesAntiarrhythmic DrugsShoeb Nawaz Khan100% (1)
- Pharmacology 3 - Management of Heart FailureDocument59 pagesPharmacology 3 - Management of Heart Failurealbatros000No ratings yet
- Cardio Lab MedsDocument11 pagesCardio Lab MedsDianne Erika MeguinesNo ratings yet
- Antiarrhythmic Drugs FinalDocument31 pagesAntiarrhythmic Drugs FinalAmanuel Maru50% (2)
- Drugs For Congestive Heart FailureDocument46 pagesDrugs For Congestive Heart Failuresultan khabeeb100% (1)
- Internal Med Board Review Course BK 2013-2014Document564 pagesInternal Med Board Review Course BK 2013-2014Akash Bhatnagar100% (1)
- Prehospital MedicationsDocument123 pagesPrehospital Medicationshilwaalfi100% (1)
- Anti Arrhythmic DrugsDocument91 pagesAnti Arrhythmic DrugsAlex beharuNo ratings yet
- Vasodilators by Hiren PatelDocument28 pagesVasodilators by Hiren PatelHiren_Patel_2427No ratings yet
- Congestive Heart FailureDocument17 pagesCongestive Heart FailureLyana StarkNo ratings yet
- Arrhythmia 2Document31 pagesArrhythmia 2rittvedNo ratings yet
- Antiarrhythmic Drugs 1Document32 pagesAntiarrhythmic Drugs 1AliImadAlKhasakiNo ratings yet
- Ventricular Septal DefectDocument55 pagesVentricular Septal DefecthoneyworksNo ratings yet
- Pharmacology of HypertensionDocument23 pagesPharmacology of HypertensionNandraj123100% (1)
- NCP Chest PainDocument2 pagesNCP Chest PainDOni Corleone87% (38)
- Anti-Arrhythmic Agents For Pharmacy PDFDocument41 pagesAnti-Arrhythmic Agents For Pharmacy PDFKelvinTMaikanaNo ratings yet
- Cardiovascular Pharmacology: Antiarrhythmic DrugsDocument80 pagesCardiovascular Pharmacology: Antiarrhythmic DrugsThái Hoà PhạmNo ratings yet
- Lecture 5 AntiarrhythmicsDocument51 pagesLecture 5 AntiarrhythmicsjawadNo ratings yet
- Congestive Cardiac Failure (1)Document27 pagesCongestive Cardiac Failure (1)Krupasagar Pn PalegarNo ratings yet
- Congestive Cardiac FailureDocument21 pagesCongestive Cardiac FailureKrupasagar Pn PalegarNo ratings yet
- Heart Failure and Antidysrhythmic DrugsDocument38 pagesHeart Failure and Antidysrhythmic DrugsYza Belle RamoNo ratings yet
- 10-11 Treatment of HypertensionDocument11 pages10-11 Treatment of HypertensionHanif GandohNo ratings yet
- Aritmia Dan Kardiotonik Eng UciDocument36 pagesAritmia Dan Kardiotonik Eng UciUci RamadhantyNo ratings yet
- Cholinergic System: e CarbamatesDocument26 pagesCholinergic System: e CarbamatesAcai BoncaiNo ratings yet
- Antiarrhythmic Drugs Class I Sodium Channel Blockers: Disopyramide (Norpace)Document5 pagesAntiarrhythmic Drugs Class I Sodium Channel Blockers: Disopyramide (Norpace)HannaNo ratings yet
- Lec 2 Heart Failure, Angina and Arryth2Document19 pagesLec 2 Heart Failure, Angina and Arryth2Adel AlomarNo ratings yet
- Cardiac ArrhythmiaDocument101 pagesCardiac ArrhythmiaYuvraj ChauhanNo ratings yet
- Congestive Heart Failure: CardiacDocument36 pagesCongestive Heart Failure: CardiacHUZAIFA YAMAANNo ratings yet
- Drugs Used in HF IIDocument40 pagesDrugs Used in HF IIJamal LudinNo ratings yet
- PharmacologyDocument23 pagesPharmacologyAbhisek ChatterjeeNo ratings yet
- Advanced Cardiac Life Support GuideDocument44 pagesAdvanced Cardiac Life Support GuideDeborah Anasthasia PakpahanNo ratings yet
- Anti-Anginal Drugs ExplainedDocument19 pagesAnti-Anginal Drugs ExplainedAnusha ZubairNo ratings yet
- FarmakologiDocument69 pagesFarmakologikekeyirawanNo ratings yet
- Antiaritmia: Frans D. Suyatna Modified by Sulistia 1010 Departemen Farmakologi & Terapeutik FKUIDocument56 pagesAntiaritmia: Frans D. Suyatna Modified by Sulistia 1010 Departemen Farmakologi & Terapeutik FKUIJoshua ObrienNo ratings yet
- Wesam R KadhumDocument31 pagesWesam R Kadhumwisam_1by1No ratings yet
- Ishac M2 Cardio Antihypertensives 2010Document16 pagesIshac M2 Cardio Antihypertensives 2010Franchesca LugoNo ratings yet
- Cardiotonic DrugsDocument67 pagesCardiotonic DrugsLady Mae Ramos100% (1)
- CARDIO Intensive CareDocument6 pagesCARDIO Intensive CareDianne Erika MeguinesNo ratings yet
- Cardio Winter BreakDocument13 pagesCardio Winter Breakmadhungry34No ratings yet
- Obat Gagal Jantung N Anti AnginaDocument42 pagesObat Gagal Jantung N Anti AnginaAyu Devi YantiNo ratings yet
- CVS DiseasesDocument15 pagesCVS DiseasesNaavaNo ratings yet
- Anoosha Roll#21Document19 pagesAnoosha Roll#21Anusha ZubairNo ratings yet
- CVS PharmacologyDocument60 pagesCVS PharmacologyGølà Sèèñàà–baale irraaNo ratings yet
- Anti Arrhythmic DrugsDocument4 pagesAnti Arrhythmic DrugsJane IjeNo ratings yet
- Pharmacology: Unit VIIIDocument92 pagesPharmacology: Unit VIIIChristian Laraya AlayonNo ratings yet
- Heat Failure DrugsDocument8 pagesHeat Failure DrugsDaniel MwiluNo ratings yet
- CHFDocument11 pagesCHFGwendolyn Talahiban LusaraNo ratings yet
- Case 02 Arrhythmias 2Document23 pagesCase 02 Arrhythmias 2pqp7mpk7v6No ratings yet
- Drugs Acting On Cardio Vascular SystemDocument16 pagesDrugs Acting On Cardio Vascular SystemANUSHYA B PSGRKCWNo ratings yet
- beta-blockers-and-calcium-channel-blockersDocument34 pagesbeta-blockers-and-calcium-channel-blockersnevena.stankovic986No ratings yet
- Cardiovascular PharmacologyDocument61 pagesCardiovascular PharmacologyTeeOne920% (1)
- AntiarrhythmicsDocument10 pagesAntiarrhythmicslandita683No ratings yet
- 11A Drugs Acting On The Cardiovascular SystemDocument85 pages11A Drugs Acting On The Cardiovascular SystemJaps De la CruzNo ratings yet
- Pharm Assigment 2Document28 pagesPharm Assigment 2Sarah-kate PatersonNo ratings yet
- Cardio CHF Angina Drugs MegDocument3 pagesCardio CHF Angina Drugs MegJhonny pingolNo ratings yet
- Types & Classes of Antiarrhythmic DrugsDocument7 pagesTypes & Classes of Antiarrhythmic DrugszanderNo ratings yet
- Antihypertensive Agents GuideDocument3 pagesAntihypertensive Agents GuideCharles BayogNo ratings yet
- Anti Hypertensive 20191211Document35 pagesAnti Hypertensive 20191211helloitsmenadNo ratings yet
- Pharmacology ReviewersDocument5 pagesPharmacology ReviewersNeisha Halil VillarealNo ratings yet
- Cardiovascular Pharmacology ReviewDocument5 pagesCardiovascular Pharmacology ReviewNeisha Halil VillarealNo ratings yet
- Holter Monitor RedactedDocument11 pagesHolter Monitor RedactedAnonymous f2WeA3No ratings yet
- PedekgDocument42 pagesPedekgJojo JohnNo ratings yet
- Understanding Tachycardia and Bradycardia ClassificationsDocument18 pagesUnderstanding Tachycardia and Bradycardia ClassificationsZega AgustianNo ratings yet
- Antiarrhythmic Agent - WikipediaDocument23 pagesAntiarrhythmic Agent - WikipediaSai Jeevan SampathiraoNo ratings yet
- Aortic Regurgitation Physical SignsDocument2 pagesAortic Regurgitation Physical SignsMalueth AnguiNo ratings yet
- Nuclear Cases SummaryDocument106 pagesNuclear Cases SummaryAkramNo ratings yet
- Barlows Syndrome PPT AbhishekDocument10 pagesBarlows Syndrome PPT AbhishekAbhishek SagarNo ratings yet
- Neonatal and Pediatric Guidelines Arrhythmia ManagementDocument16 pagesNeonatal and Pediatric Guidelines Arrhythmia ManagementAkhmad HidayatNo ratings yet
- Lutembacher's Syndrome at KolonodaleDocument7 pagesLutembacher's Syndrome at KolonodaleWayan GunawanNo ratings yet
- ACLS 2005 Guidelines SummaryDocument11 pagesACLS 2005 Guidelines Summarygr8_nurseNo ratings yet
- Cardiovascular Signs and Symptoms GuideDocument65 pagesCardiovascular Signs and Symptoms GuideWilliam ApostolNo ratings yet
- Mastering Electocardiograms - Honda-2Document3 pagesMastering Electocardiograms - Honda-2Christian MacielNo ratings yet
- USMLE Step 2 CK Cardiology ReviewDocument27 pagesUSMLE Step 2 CK Cardiology ReviewfilchibuffNo ratings yet
- Simultaneous Atrial and Ventricular Pacing During Narrow Complex Tachycardia - The Janus Response. Which One Is True?Document5 pagesSimultaneous Atrial and Ventricular Pacing During Narrow Complex Tachycardia - The Janus Response. Which One Is True?Sahil HasanNo ratings yet
- Kelompok 16 PBL CVSDocument11 pagesKelompok 16 PBL CVSTutde SedanaNo ratings yet
- CardiomyopathyDocument13 pagesCardiomyopathyRaprnaNo ratings yet
- Pulse and Blood Pressure Measurement QuestionsDocument3 pagesPulse and Blood Pressure Measurement QuestionsHurryNo ratings yet
- Electrocardiographic Exercise Stress Testing PDFDocument15 pagesElectrocardiographic Exercise Stress Testing PDFRafaelDavidVillalbaRodriguezNo ratings yet
- Is The Cardiac Rehabilitation Programme Successful in Serdang Hospital: Patients' PerspectiveDocument3 pagesIs The Cardiac Rehabilitation Programme Successful in Serdang Hospital: Patients' PerspectiveAnanthankumar MunusamyNo ratings yet
- ARITMIA, Gangguan Irama JantungDocument37 pagesARITMIA, Gangguan Irama JantungNovriefta NugrahaNo ratings yet
- Sudden Death From Dilated Cardiomyopathy: Case ReportDocument4 pagesSudden Death From Dilated Cardiomyopathy: Case ReportAnonymous JXEtV98KjPNo ratings yet
- Echocardiography Assessment of Coronary Artery DiseaseDocument28 pagesEchocardiography Assessment of Coronary Artery DiseaseYibeltal AssefaNo ratings yet
- Cardiac Arrhythmias Guide - Causes, Symptoms and Treatment OptionsDocument5 pagesCardiac Arrhythmias Guide - Causes, Symptoms and Treatment OptionsaksinuNo ratings yet
- DR Mervat Aboulmaaty Nabih Professor of Cardiology Ain Shams UniversityDocument51 pagesDR Mervat Aboulmaaty Nabih Professor of Cardiology Ain Shams UniversitySaud ShirwanNo ratings yet
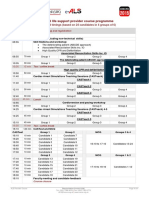
- E-ALS Programme IO ARS (March 2016)Document1 pageE-ALS Programme IO ARS (March 2016)Florentina GasttiNo ratings yet
- Infant Tachycardia ECG Differential DiagnosisDocument5 pagesInfant Tachycardia ECG Differential DiagnosisDeepak KumarNo ratings yet