You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Management Scrutinizes Variances to Detect Issues and Improve PerformanceDocument3 pagesManagement Scrutinizes Variances to Detect Issues and Improve PerformanceRobert GarlandNo ratings yet
- Diagnostics TestDocument4 pagesDiagnostics TestAnna LeeNo ratings yet
- Introduction To Science: Study Guide For Module No. 1Document6 pagesIntroduction To Science: Study Guide For Module No. 1Kate SolizaNo ratings yet
- Treatise of Plane Geometry Through Geometric Algebra - R G CalvetDocument290 pagesTreatise of Plane Geometry Through Geometric Algebra - R G Calvetw2006y100% (1)
- Void Empires v6Document342 pagesVoid Empires v6SamWissaNo ratings yet
- Draft CSA E-Course SyllabusDocument5 pagesDraft CSA E-Course Syllabussodad27326No ratings yet
- BSBOPS504 Student GuideDocument44 pagesBSBOPS504 Student GuideAhadNo ratings yet
- Um Cat1000p eDocument78 pagesUm Cat1000p eYnomata RusamellNo ratings yet
- Emile Durkheim'in Pragmati̇zm Üzerine Fi̇ki̇rleri̇Document304 pagesEmile Durkheim'in Pragmati̇zm Üzerine Fi̇ki̇rleri̇İlayda ilaydasaglamhotmail.comNo ratings yet
- English - Grade 1Document16 pagesEnglish - Grade 1Michael Jorge Bernales100% (1)
- Motivating & LeadingDocument52 pagesMotivating & LeadingABDUR REHMAN SAITNo ratings yet
- Chapter 4 Kinematics in Two DimensionDocument44 pagesChapter 4 Kinematics in Two DimensionAmar DanialNo ratings yet
- BuildingDocument6 pagesBuildingBassy emke warantyNo ratings yet
- ChromismDocument17 pagesChromismarathinamNo ratings yet
- Use Case Diagram LectureDocument42 pagesUse Case Diagram LectureUMM E RUBABNo ratings yet
- Understanding Human Experiences Through Hermeneutic PhenomenologyDocument28 pagesUnderstanding Human Experiences Through Hermeneutic PhenomenologyKath MercadejasNo ratings yet
- Learner's Activity Sheet Assessment Checklist: Contemporary Philippine Arts From The Regions Quarter 2 - Week 7Document17 pagesLearner's Activity Sheet Assessment Checklist: Contemporary Philippine Arts From The Regions Quarter 2 - Week 7Ken KenNo ratings yet
- Thou Art My Battle Axe: Click HereDocument4 pagesThou Art My Battle Axe: Click HereProphet DonNo ratings yet
- APC200 ECM-ECI v3.5 PDFDocument134 pagesAPC200 ECM-ECI v3.5 PDFCao Lan100% (3)
- NCERT Solutions For Class 6 Social Science History Chapter 1 What Where How and WhenDocument4 pagesNCERT Solutions For Class 6 Social Science History Chapter 1 What Where How and WhenJisha Annie JohnNo ratings yet
- Kalam Cosmological ArgumentDocument12 pagesKalam Cosmological ArgumentGabo GonzálezNo ratings yet
- GL XX Mobil DTE Oil Double Letter SeriesDocument3 pagesGL XX Mobil DTE Oil Double Letter SeriesMuhammad RipandiNo ratings yet
- Ito Super ScienceDocument34 pagesIto Super ScienceMiguel Antonio MiladoNo ratings yet
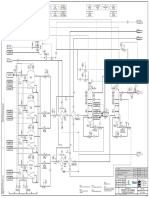
- U36F001N - Process Flow Diagrams Revisio N 17-7-2015Document6 pagesU36F001N - Process Flow Diagrams Revisio N 17-7-2015Osamah AdelNo ratings yet
- Fiji Water and CSR - Green Makeover or "Greenwashing"?Document3 pagesFiji Water and CSR - Green Makeover or "Greenwashing"?Sidharth JainNo ratings yet
- Algebra II NoteDocument1 pageAlgebra II NoteMiyu TakahashiNo ratings yet
- D9520-069 882 - 2015 - 10 - 14 - Bal - enDocument55 pagesD9520-069 882 - 2015 - 10 - 14 - Bal - enmgustavo5No ratings yet
- Evolution Hand OutDocument4 pagesEvolution Hand Outrosana f.rodriguezNo ratings yet
- Carrier Hap 4.8 ManualDocument140 pagesCarrier Hap 4.8 ManualInventor Solidworks50% (2)
- Soil Erosion Control Mechanical MethodsDocument3 pagesSoil Erosion Control Mechanical MethodsRubybharatNo ratings yet